
Abstract
Objective
Numerous studies have focused on the prognostic roles of CD24 and CD44 in breast cancer, but the results have been equivocal. The aim of this study was to gain better insight into the relationship between expression of CD24 and of CD44, either alone or in combination, and prognostic parameters in breast cancer.
Methods
Publications addressing the associations of CD24 or CD44 expression with survival outcome in breast cancer were selected for the meta-analysis according to defined criteria. Studies were pooled and odds ratios (ORs) or hazard ratios (HRs) were calculated. Publication bias and sensitivity analyses were also conducted.
Results
Sixteen studies comprising 5,697 breast cancer cases were included in our meta-analysis. Overall, CD24 overexpression was significantly associated with histological grade (OR = 1.52; 95% CI 1.12-2.06, p = 0.007), stage (OR = 1.74; 95% CI 1.27-2.40, p<0.001), shortened overall survival (HR = 1.48; 95% CI 1.21-1.80, p<0.001) and disease-free survival (HR 1.45, 95% CI 1.19-1.76, p<0.001), while no such association was observed when we limited our analysis to CD44 and CD44+/CD24- phenotypes. Subgroup analyses for CD24 according to the studies categorized by ethnicity, staining patterns and follow-up period were also conducted, and supported the stability of the prognostic role of CD24.
Conclusions
Our study demonstrated that the putative stem cell marker CD24 was significantly associated with worse survival based on the obtained data. In particular, CD24 may play a role in tumorigenesis and cancer progression. However, further large-scale studies are needed to confirm these findings.
Introduction
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among females, accounting for 1.38 million (23%) of the total new cancer cases and 458,400 (14%) of the total cancer deaths based on the GLOBOCAN 2008 estimates (1). Although various treatments have been used for breast cancer, such as chemotherapy, radiation and hormone therapy, the prognosis of advanced breast cancer is still poor, with an average median survival time of less than 30 months (2). This is mainly due to a lack of effective and specific biomarkers. There is a clear need for the identification of new genes and molecules that are strongly associated with breast cancer progression and prognosis. This would allow to develop novel chemotherapeutic or biological agents targeting potential molecular markers, and improve the survival outcome of breast cancer patients.
The identification of cancer stem cell (CSC) niches in tumor tissues is acquiring great prognostic value, mainly because breast carcinogenesis may be the result of deregulation of molecular pathways controlling self-renewal of mammary epithelial cells (3). Tumorigenic breast CSCs were first distinguished by Al-Hajj et al (4) as having a CD44+/CD24–/low phenotype. CD24 is a small, heavily glycosylated mucin-like glycosylphosphatidyl-inositol-linked cell surface protein that has been detected in various types of carcinomas, including B-cell lymphoma, renal cell carcinoma, lung cancer, nasopharyngeal carcinoma, hepatocellular carcinoma, bladder carcinoma, glioma, epithelial ovarian cancer and breast cancer, whereas it is rarely expressed in normal tissues (5–9). CD44 is a transmembrane glycoprotein that is associated with aggressive tumor behavior in breast cancer (10, 11). Numerous studies have focused on the roles of CD24 and CD44 in breast cancer with respect to overall survival (OS) and/or disease-free survival (DFS) (12–27), but the results have been controversial. As meta-analysis is an essential tool for accurately and reliably summarizing evidence, we conducted this meta-analysis to gain better insight into the direct relationship between the expression of CD24 and CD44, either alone or in combination, and patients' survival status. Furthermore, we tried to investigate the correlations of CD24 and CD44 expression with patients' clinical characteristics, which, to the best of our knowledge, has not been previously performed.
Materials and methods
Literature search
Studies were identified via an electronic search of PubMed, Embase, Web of Science and Cochrane Library (updated to May 1, 2016). The search terms were breast cancer, CD24, CD44, prognostic, prognosis and survival, while the syntax used for the search was ((“CD24”[All Fields] OR “CD44”[All Fields]) AND (“breast cancer”[All Fields]) AND (“prognosis”[All Fields] OR “prognostic”[All Fields]) OR “survival”[All Fields])). The languages were limited to English. We also used a manual reference search for relevant articles, including original articles and reviews, to identify additional studies.
Selection criteria
A study was included if it met the following inclusion criteria: (a) full text publication evaluated the association between either OS or other prognostic factors and the expression of CD24 or CD44 or CD44+/CD24–/low phenotype in breast cancer; (b) hazard ratios (HRs) and their 95% confidence intervals (CIs) for OS or other prognostic factors had to be reported or could be computed from the data presented; (c) the most recent report or the most informative one was included to avoid duplicate publications. Reviews, conference abstracts and comments were excluded for insufficient data.
Data extraction
The final set of articles was assessed independently by 2 investigators (ZW and QW). Disagreements between reviewers were resolved by consensus. The following information was extracted from each study: first author, year of publication, country, number of patients, numbers of different clinical and pathological parameters, detection methods, cutoff, follow-up period and HR with 95% CI. Some of the published articles did not provide HR and 95% CI directly. In such cases, 2 reviewers (ZW and YW) independently digitized and extracted the data through the Kaplan-Meier curves using GetData Graph Digitizer 2.24 (http://getdata-graph-digitizer.com), and then reconstructed the HR and its variance (GraphPad Software, Inc.).
Statistical analysis
Odds ratios (ORs) with 95% CIs were used to estimate the associations between the putative stem cell markers (CD24 or CD44) and general prognostic markers for breast cancer including tumor size, histological grade, stage and nodal status. The HR with its variance estimates (95% CI) was extracted or calculated to evaluate the correlations between CD24 or CD44 or CD44+/CD24–/low phenotype and breast cancer survival outcome. The chi–square-based Q test with the inconsistency index I2 was used to detect statistically significant heterogeneity across studies. When a significant Q test (p<0.05 or I2>50%) indicated heterogeneity among studies, the random-effects model (DerSimonian-Laird method) was used for the meta-analysis; otherwise, the fixed-effects model (Mantel-Haenszel method) was chosen. One-way sensitivity analysis was conducted to assess the stability of the results by deleting 1 study at a time to reflect the influence of the individual data set on the pooled HR (28). The publication bias was tested by Begg's funnel plots, whose symmetry was further assessed using Egger's linear regression method (29). All statistical tests were 2-sided and p<0.05 was taken to indicate a statistically significant result. All analyses were performed with the Stata software, version 12.0 (StataCorp LP) and Review Manager software, version 5.3 (Cochrane Collaboration).
Results
Selection and characteristics of studies
After the initial literature search, a total of 618 potentially relevant citations were retrieved. Three hundred forty-five articles were excluded after the first screening based on abstracts or titles, since they were reviews, abstracts, letters to the editor, animal or in vitro studies, or duplications, leaving 273 studies for further evaluation. After carefully reading the full-text articles, we excluded 257 articles for not being relevant to the current topic or lacking sufficient survival data. As a result, 16 articles for a total of 20 eligible studies comprising 5,697 breast cancer cases were included in this meta-analysis (12–27). The main characteristics of the enrolled studies are summarized in Table I. Briefly, sample sizes ranged from 50 to 1,681. Of the 16 articles, 7 were from Europe, 7 from Asia and 2 from America. Only 1 study used immunofluorescent technique to detect CD24 and CD44 (16). In the other studies (12-15, 17-27), expression of CD24 and CD44 in breast cancer was assessed using immunohistochemistry (IHC).
Characteristics of studies included in the meta-analysis
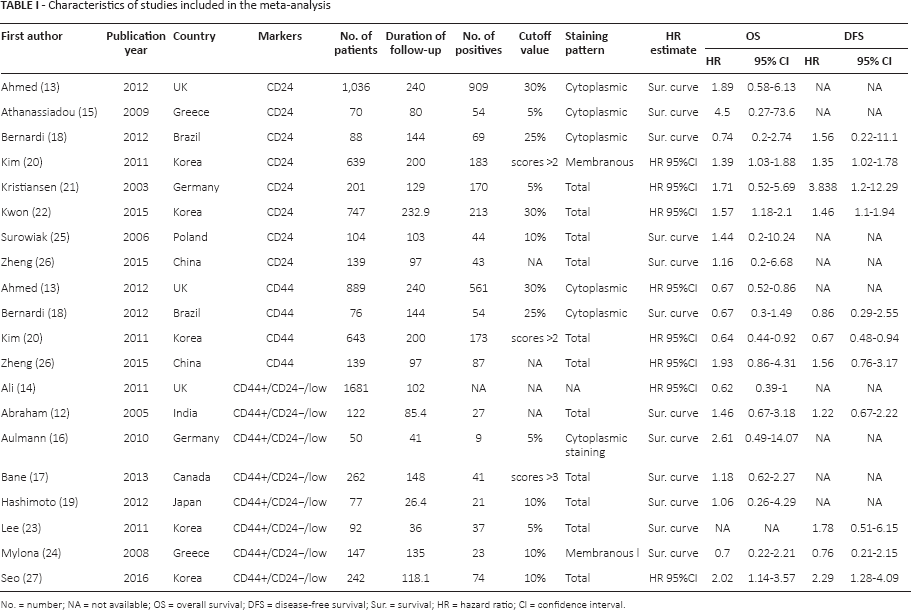
No. = number; NA = not available; OS = overall survival; DFS = disease-free survival; Sur. = survival; HR = hazard ratio; CI = confidence interval.
Meta-analysis results
The prognostic effect of CD24 on survival in breast cancer
OS was reported in 8 studies (13, 15, 18, 20–22, 25, 26) with a total of 3,024 breast cancer patients. The meta-analysis of all these studies confirmed a significant association between CD24 and worse OS with a pooled HR of 1.48 (95% CI 1.21-1.80, p<0.001) (Fig. 1). Data for DFS were reported in 4 studies (18, 20–22). The pooled analyses for DFS were similar, both pointing to a decreased survival associated with high CD24 expression (HR = 1.45, 95% CI 1.19-1.76, p<0.001) (Fig. 2). Our results indicated that CD24 was an independent prognostic factor in patients with breast cancer.
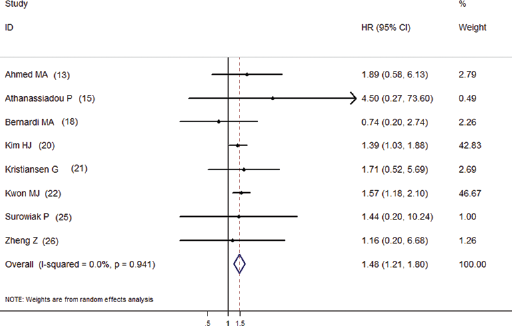
The association between CD24 overexpression and overall survival of breast cancer stratified by HR estimation. The summary HRs and 95% CIs according to the random-effects estimations are shown.
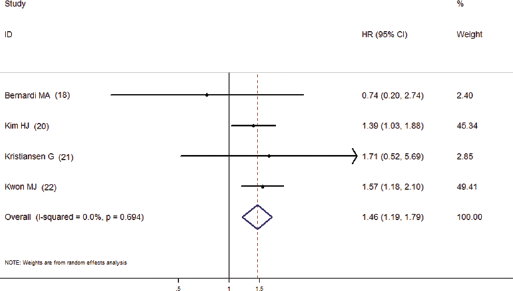
The association between CD24 overexpression and disease-free survival of breast cancer stratified by HR estimation. The summary HRs and 95% CIs according to the random-effects estimations are shown.
The prognostic effect of CD44 on survival in breast cancer
OS was reported in 4 studies (13, 18, 20, 26) with a total of 1,747 patients. The meta-analysis of all these studies did not show a significant association between CD44 and OS with a pooled HR of 0.76 (95% CI 0.54-1.08, p = 0.129). Data for DFS were reported in 3 studies (18, 20, 26). The pooled analyses for DFS were similar, showing no survival effect associated with high CD44 expression (HR = 0.92, 95% CI 0.52-1.61, p = 0.75).
The prognostic effect of CD44+/CD24–/low phenotype on survival in breast cancer
OS was reported in 7 studies with a total of 2,673 breast cancer patients (12, 14, 16, 17, 19, 24, 27). No significant association was observed between CD44+/CD24–/low phenotype and OS with a pooled HR of 1.16 (95% CI 0.75-1.79, p = 0.51). Likewise, the pooled data for DFS from 4 studies (12, 23, 24, 27) also showed no association with CD44+/CD24–/low phenotype (HR = 1.53, 95% CI 0.98-2.39, p = 0.06).
Subgroup analysis for CD24
We also conducted subgroup analyses for CD24 based on ethnicity, staining patterns and follow-up period (Tab. II). When patients were grouped according to ethnicity, overexpression of CD24 was associated with poor OS in Asian populations with combined HR 1.48 (95% CI 1.20-1.82, p<0.001) but not in non-Asian populations (HR = 1.48, 95% CI 0.78-2.84, p = 0.232). In the subgroup analysis according to CD24 staining pattern as defined by the studies' authors, the combined HRs of the studies defining cytoplasmic staining as positive for OS was 1.39 (95% CI 0.60-3.21, p = 0.438). The combined HR was 1.56 (95% CI 1.19-2.06, p = 0.001) based on studies defining total staining as positive. Furthermore, we aggregated the studies separately according to the follow-up period. The association between CD24 and poor OS was found only for studies with a longer follow-up period (≥120 months) (HR = 1.47, 95% CI 1.21-1.80, p<0.001).
Summarized HRs of subgroup analyses for CD24 on breast cancer overall survival
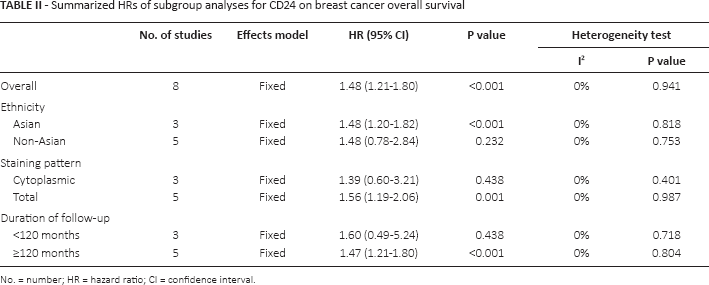
No. = number; HR = hazard ratio; CI = confidence interval.
CD24 expression and clinical features
To gain further insight into the role of CD24 as a biological marker, we investigated the correlation between CD24 expression level and clinical characteristics including tumor size, nodal status, histological grade and stage. All the above data had been pooled to calculate the ORs. We did not find that CD24 expression was significantly correlated with tumor size or nodal status. However, the correlation results for histological grade and stage were evidently significant. The combined ORs of studies about histological grade and stage were 1.52 (95% CI 1.12-2.06, p = 0.007) and 1.74 (95% CI 1.27-2.40, p<0.001), respectively. These results are summarized in Table III.
Meta-analyses assessing the association between high CD24 expression and clinical features
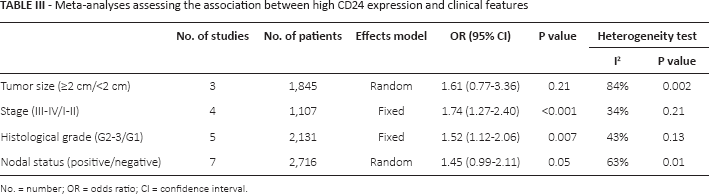
No. = number; OR = odds ratio; CI = confidence interval.
Publication bias and sensitivity analyses
Publication bias of our meta-analysis was assessed by Begg's funnel plot and Egger's test. In all included studies, no funnel plot asymmetry was observed, with p = 0.921 in Egger's test (Fig. 3), indicating no evidence of a significant publication bias. Sensitivity analyses were performed by omitting 1 study at a time to check if individual studies affected the final results. All the results were not materially altered.
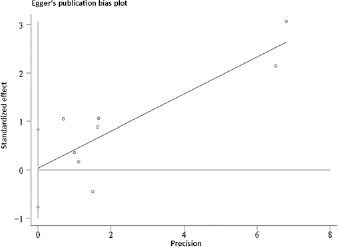
Egger's funnel plot to detect publication bias on the overall estimate.
Discussion
Previous studies have suggested that the expression of CD24 and CD44 was closely related to tumor metastasis, proliferation, invasion and progression (30, 31), but the prognostic value of both markers in breast cancer is still unclear due to the presence of controversial results in different studies. Therefore, the present meta-analysis was performed to summarize all the available research that compared the survival outcomes of breast cancer patients according to the expression status of CD24 and CD44.
The pooled data in this meta-analysis showed promising prognostic value of CD24 detected in tumor samples for both OS and DFS. Breast cancer patients with elevated CD24 expression had a 1.48 times higher risk of poor prognosis compared with patients without high CD24 expression. However, when we limited our analysis to CD44 and CD44+/CD24–/low phenotype, the expression was not associated with survival. Although no significant heterogeneity was detected in this meta-analysis for OS and DFS, a stratified subgroup analysis for CD24 was performed to increase the homogeneity. The results suggested that CD24 was a poor prognostic indicator in Asian populations but not in non-Asian populations. Immunolocalization of CD24 also reflected different clinical significance. Overexpression of total CD24 was found to correlate with poor survival, while cytoplasmic expression was not an independent marker for survival, suggesting that the prognostic value of CD24 positivity was stronger when the analysis focused on total CD24 staining. Moreover, when the follow-up period was taken into account, we found that the association was significant for studies with longer follow-up (≥120 months), while no significant association was observed for studies with follow-up periods <120 months, indicating that the CD24 expression status might be more valuable in predicting long-term outcome of breast cancer.
As CD24 showed a significant association with poor OS and DFS outcomes in breast cancer patients, further investigation into the correlations between CD24 and clinicopathological features was performed. In the present meta-analysis, CD24 overexpression was significantly associated with histological grade and clinical stage, while ORs for tumor size and nodal status were not significant. In studies on breast cancer cell lines in vivo, CD24 was found to act as a ligand for P-selectin on the lung vascular endothelium (32). Tumor cells with increased CD24 expression acquired the capacity to form stabilized platelet-tumor thrombi and then adhered to endothelial cells at the metastatic sites, which protected tumor cells from destruction and promoted tissue penetration and tumor extravasation (33, 34). In addition, CD24 was revealed to positively correlate with tumorigenesis and cancer progression in gene expression profiling studies (35). Thus, our results are in line with those of basic studies. Although the mechanism of cancer progression caused by expressional alterations remains unknown, CD24 overexpression may be considered as a marker of breast cancer that indicates invasiveness. However, correlation of high CD24 expression with tumor size or nodal status was not observed. These discrepancies might be due to the different sample cohorts studied, as well as to the relatively small number of studies included. Hence, large sample sizes must be reanalyzed to draw firm conclusions.
Several studies indicated that high CD44 expression is associated with poor prognosis and might be considered a target for therapy in breast cancer (36, 37). Moreover, CD44+/CD24–/low breast cancer cell lines have highly invasive and metastatic properties (38, 39) and thus should correlate with poor prognosis. On the other hand, it has been documented that a CD44-negative cell population might be related to unfavorable clinical outcome. Lopez et al (40) provided in vivo evidence that loss of CD44 promoted distant metastasis. In the present meta-analysis, the pooled data showed no influence of a CD44+ or CD44+/CD24–/low immunophenotype on OS or DFS in breast cancer patients. However, due to limited information provided by the included studies, we could not perform further investigations into the prognostic roles of these molecules in different cancer subtypes because the CD44/CD24 expression profiles showed considerable variability within breast cancer subtypes (20). Klingbeil et al (41) reported that CD44 expression is particularly enriched in estrogen receptor (ER)-negative, progesterone receptor (PR)-negative and/or human epidermal growth factor receptor 2 (HER2)-negative breast cancers, which have the worst clinical prognosis and outcome. Therefore, these results highlight the need for larger-sample studies to answer the question of whether CD44 is a true prognostic marker of patients' outcome or a predictive marker of sensitivity to therapy.
We made an effort to conduct a comprehensive analysis, but some limitations need to be acknowledged. First of all, although we tried to identify all relevant data, potential publication and reporting bias were unavoidable since only fully published studies and studies in English were included. Second, most survival outcomes were calculated from Kaplan-Meier curves, which may have introduced some imprecision. Third, in the assessment of biomarkers, the use of a standard threshold is of great importance. Although immunohistochemistry was the most commonly applied method, there was no consistent standard for cutoff values in our eligible studies, which might have caused clinical and statistical heterogeneity. Fourth, breast cancer patients had received different treatments and this may have influenced their survival. It was reported that the hazard associated with CSC-positive cases treated with adjuvant chemotherapy was different from that of cases where no chemotherapy was given (14, 25). Nevertheless, most of the published studies lacked required data regarding patient treatment, which could produce additional inconsistencies and cause potential selection bias. Therefore, treatment should be taken into consideration as a stratification factor in future studies and questions relating to the therapeutic effect of CSC-enriched tumors should be best addressed in the context of randomized clinical trials. Last but not least, due to the lack of adequate information, we were unable to perform subgroup analyses based on breast cancer subtypes (e.g., ER/PR/HER2 negative or positive). As there might be associations between CD24 (and also CD44) and other prognostic markers including ER, PR and HER2 (41–43), the exact value of CD24 or CD44 expression status needs to be determined by appropriate multivariate and stratified analyses.
In summary, despite the above limitations, the combined data of our meta-analysis demonstrated that the putative stem cell marker CD24 was significantly associated with worse survival based on the currently obtained data. In particular, CD24 may play a role in tumorigenesis and cancer progression. However, these findings must be interpreted with caution when used in clinical practice, since the reported associations were diverse. Larger well-designed prospective cohort studies are needed to further evaluate the association between CD24 and the survival of patients with breast cancer.
Footnotes
Financial support: This study was supported by Projects in the Science and Technology Pillar Program from the Department of Science and Technology of Sichuan Province (2015SZ0151).
Conflict of interest: None.