
Abstract
Background
The role of p16INK4a as a surrogate marker for screening human papillomavirus (HPV) in esophageal squamous cell carcinoma (ESCC) remains controversial.
Methods
A comprehensive search of EMBASE, PubMed, China National Knowledge Infrastructure and China Biology Medicine was performed from inception to December 27, 2015. A random-effects model was applied to the pooled odds ratios (ORs) with 95% confidence intervals (CIs).
Results
Ten studies were identified (985 cases). The pooled results showed no significant relationship between p16INK4a expression and HPV infection in ESCC based on overall HPV types (OR: 1.79, 95% CI: 0.69-4.66, p = 0.235). Subgroup analysis by HPV detection method showed no statistical significance in either the polymerase chain reaction (PCR) (OR: 1.65, 95% CI: 0.83-3.30, p = 0.154) or in situ hybridization (ISH) group (OR: 2.58, 95% CI: 0.03-268.14, p = 0.689). The pooled OR of the sensitivity analysis ranged from 1.27 (95% CI: 0.58-2.84) to 2.32 (95% CI: 0.95-5.64). Of these studies, 6 involved only high-risk human papillomavirus types (HR-HPV), HPV16 or HPV18. However, similar observations were made for HR-HPV (OR = 1.31, 95% CI: 0.26-6.59, p = 0.741). Subgroup analysis again showed no statistical significance in the PCR group (OR: 0.95, 95% CI: 0.25-3.64, p = 0.940) and ISH group (OR: 2.58, 95% CI: 0.03-268.14, p = 0.689). Sensitivity analysis showed that the pooled OR ranged from 0.69 (95% CI: 0.21-2.22) to 1.89 (95% CI: 0.33-10.86).
Conclusions
p16INK4a is not a reliable screening marker of HPV infection in ESCC. Further multicenter, large-sample and well-matched prospective studies are still required to illuminate the possible etiological roles of HPV in ESCC.
Introduction
Esophageal carcinoma ranks ninth in cancer incidence and sixth in cancer mortality around the world (1). A recent study carried out by the International Agency for Research on Cancer (IARC) showed that there are approximately 455,800 new cases of esophageal carcinoma and 400,200 related deaths each year. Esophageal squamous cell carcinoma (ESCC) has been identified as the most common pathological type (more than 90%) (1, 2). According to the recorded clinical data, human papillomavirus (HPV) has been detected in a large number of patients with ESCC (3).
HPV is a spherical DNA virus that only infects human beings; it has more than 130 genotypes, most notable among which HPV16 and HPV18. Previous studies have established HPV as an etiological factor in cervical neoplasms (4-5-6), along with being a significant risk factor in head and neck squamous cell carcinoma (7), particularly oropharyngeal squamous cell carcinoma (8, 9). HPV has been suggested to be a risk factor for ESCC since the presence of HPV in ESCC was first mentioned by Syrjänen in the 1980s (10). This virus possesses 2 identified oncogenes, E6 and E7. E6 has been demonstrated to inactivate p53 and thus plays an important role in the development of cancer. E7 also showed notable oncogenic potential by its ability to inactivate retinoblastoma tumor suppressor actions (11). E6 and E7 can prompt the cell to enter S-phase, leading to cell-cycle interruption and proliferation and subsequently oncogenesis, and eventually inducing upregulation of p16INK4a expression to levels that can be detected readily by immunohistochemistry (IHC) (12).
Previous studies have demonstrated that p16INK4a is highly expressed in oropharyngeal squamous cell carcinoma patients who have been infected by HPV (12-13-14). Additionally, p16INK4a was also strongly expressed in patients with head and neck squamous cell carcinoma (7, 15) and patients with cervical squamous cell carcinoma (16, 17) who had been infected by HPV. Based on these results, p16INK4a is mostly regarded as a screening marker in squamous cell carcinoma in patients infected with HPV (12, 16, 17, 13-14-15). Nonetheless, the role of p16INK4a as a surrogate marker of HPV infection in ESCC remains controversial.
Numerous studies have researched the role of p16INK4a in HPV-infected ESCC patients, but there are still no final and consistent conclusions. Among the included studies, some (18-19-20-21-22) suggested that p16INK4a may play an important role in the development of ESCC in patients infected with HPV, but others (23-24-25-26-27) hold an opposite view. It is therefore necessary to perform quantitative aggregation of these results. In an attempt to clarify the controversy, we undertook this meta-analysis to evaluate the relationship between p16INK4a expression and HPV in ESCC.
Materials and methods
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) checklist (Supplementary Table S1 - PRISMA checklist. Available online at www.biological-markers.com) (28).
Search Strategy
An independent search was done by 2 authors for studies from the following databases: EMBASE, PubMed, China National Knowledge Infrastructure (CNKI) and China Biology Medicine (CBM) from inception to December 27, 2015. The search strategies used combinations of the following search terms: (“esophageal squamous cell carcinoma” OR “oesophageal squamous cell carcinoma” OR “esophageal carcinoma” OR “esophageal cancer” OR “carcinoma of esophagus”) AND (“HPV” OR “human papillomavirus”) AND (“p16INK4a” OR “p16INK4a protein” OR “p16” OR “p16INK4a gene”). Only human studies were considered. No language or date-of-publication restrictions were imposed. In addition, a manual search was done by checking the references of relevant studies to identify additional potential studies. Any divergence was resolved through discussion and consensus with a third author.
Eligibility Criteria
Three authors evaluated the studies obtained with the independent search. Divergences were solved by discussion between authors. The eligibility criteria were as follows: (i) studies in which patients were diagnosed with ESCC by pathological diagnosis; (ii) studies explicitly describing the method of HPV DNA detection, which mainly included polymerase chain reaction (PCR) and in situ hybridization (ISH) amplification methods; (iii) randomized controlled trials, case-control studies, and prospective cohort studies; (iv) studies in which the sample size was no less than 5 individuals; (v) studies that reported the relationship between p16INK4a expression and HPV infection in ESCC. If a study was reported in duplication, we selected the one which provided more relevant information. Review articles without data, case reports, letters, and studies on animals and other cancers were excluded.
Data Extraction
Data extraction was carried out independently by 4 authors according to an accepted standard. Subsequently, the collected data were cross-checked by 2 additional authors and discrepancies were solved by discussion. For each article, we extracted in detail the following data: author information, date of publication, name of journal, study design, study country or area, sample size, characteristics of patients, types of primers and specimens, HPV types, method of HPV detection, p16INK4a detection method, and definition of p16INK4a expression. Subsequently, we imported the collected data into a standardized Microsoft Office Excel file.
Quality Assessment
The quality of the established studies was systematically assessed by 4 reviewers using the Newcastle-Ottawa Scale (NOS) criteria (www.ohri.ca/programs/clinical_epidemiology/oxford.asp). A star system for quality assessment was used that contains 3 sections: selection (0-4); comparability (0-2); and exposure (0-3) (29). The aggregate stars ranged from 0 to 9. Studies with at least 5 stars were included in our meta-analysis, and those with more than 7 stars were regarded as high-quality studies. We again resolved any disagreement through discussion between the authors.
Statistical Analysis
Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to estimate the relationship between p16INK4a expression and HPV infection in ESCC. Statistical tests were two-sided and p values less than 0.05 were considered statistically significant. We used the inconsistency (I2) test and Cochran's Q-test to calculate heterogeneity between studies. I2 values <25%, 25%-50%, 50%-75%, and >75% were supposed to have no heterogeneity, low heterogeneity, moderate heterogeneity, and high heterogeneity, respectively (30). If significant heterogeneity was observed (I2>50% or p value of the Q-test <0.1), a random-effects model was applied; otherwise, a fixed-effects model was used (31). To assess the stability of the pooled results, sensitivity analysis was applied. To explore the sources of heterogeneity, subgroup analyses were done.
The potential publication bias was assessed by means of the funnel plots of Egger's and Begg's tests. If the funnel plot was asymmetric or the p value of Egger's tests >0.5, this was regarded as no publication bias. Stata version 12.0 (StataCorp LP) (www.stata.com) was used for all statistical analyses in the study.
Results
Search Results
A total of 83 potentially relevant studies were initially identified based on our predefined search strategy. After excluding duplicates and screening titles and abstracts, 27 articles were chosen for further detailed evaluation, and 56 articles were excluded for the following reasons: duplicates (n = 28); review or systematic review (n = 5); reported on esophageal precancerous lesions (n = 5); reported on esophageal squamous papilloma (n = 4); reported on head and neck squamous cell carcinoma (n = 5); reported on esophageal adenocarcinoma and Barrett's esophagus (n = 4); reported on cell metabolism (n = 5). After reviewing the full text in detail, we removed 17 studies for the following reasons: lack of detailed information regarding p16 protein (n = 7); reported the same study (n = 5); conference poster (n = 1); conference abstract (n = 2) ; lack of control information on HPV-negative cases (n = 1); reported genetic alterations of esophageal carcinoma (n = 1). A total of 10 articles involving 235 cases and 750 controls (985 ESCC cases), which were published between 2006 and 2014, were eligible and included in this meta-analysis (18-19-20-21-22-23-24-25-26-27). The process of inclusion and exclusion was performed according to the PRISMA statement (32). The flowchart of the literature selection process is shown in Figure 1.

Flowchart of the study selection process in the meta-analysis.
Study Characteristics and Quality Assessment
The main characteristics of the included studies are summarized in Table I. Of these studies, 6 reported only on high-risk types of human papillomavirus (HR-HPV), i.e., HPV16 or HPV18 (18, 20-21-22, 24, 26). The others focused on multiple HPV types (19, 23, 25, 27). Eight studies were published in English (18-19-20, 23-24-25-26-27) and 2 in Chinese (21, 22). The patients in these studies came from different countries including China (18, 20-21-22, 24, 27), Brazil (23), Japan (19), Pakistan (19), Sweden (25), Colombia (19, 26), and Chile (26). Formalin-fixed, paraffin-embedded (FFPE) samples were used to detect HPV DNA by means of PCR or ISH amplification; p16INK4a expression was detected by IHC.
Characteristics of the study selection process in the meta-analysis

HPV = human papillomavirus; PCR = polymerase chain reaction; ISH = in situ hybridization; IHC = immunohistochemistry; FFPE = formalin-fixed, paraffin-embedded samples; NA = data not available.
Type-specific (TS) primers (SP16, SP18) which were primers within the E7 ORF, to amplify HPV16 and HPV18, respectively; BS primers mainly included general primers, consensus primers, GP5/6, MY09/11, SPF1, and SPF10.
Quality assessment was judged on the basis of the Newcastle-Ottawa Scale (1-9 stars) for non-randomized studies.
Table II summarizes the details of quality assessment. The aggregate stars of the included studies ranged from 6 to 9. Six of the 10 studies were identified as high quality, as shown in Table I.
Quality assessment of non-randomized controlled trials based on the Newcastle-Ottawa scoring system

A maximum of 2 stars can be given for comparability.
Meta-Analysis Results
Association between p16INK4a Expression and Overall-HPV-Type Infection in ESCC
Ten studies (18-19-20-21-22-23-24-25-26-27) assessed the potential association between p16INK4a expression and overall HPV types (types 1, 6, 11, 16, 18, 33, 35, 42, 45, 51, 52, 66, 68, 73 and 82) in ESCC. p16INK4a was detected in 39.6% of the HPV-positive and 20.5% of the HPV-negative specimens. As there was significant heterogeneity between studies (I2 = 82.7%, p<0.0001), the random-effects model was used. As shown in Figure 2A, the pooled analysis showed no significant association between p16INK4a expression and HPV infection in ESCC based on overall HPV types (OR: 1.79, 95% CI: 0.69-4.66, p = 0.235). To explore the sources of the significant heterogeneity, subgroup analysis was performed by HPV detection method. The results indicated no statistical significance in either the PCR (OR: 1.65, 95% CI: 0.83-3.30, p = 0.154) or ISH group (OR: 2.58, 95% CI: 0.03-268.14, p = 0.689) (Fig. 2B). The result of subgroup analysis can explain only approximately 30% of the heterogeneity.

Forest plot of the present meta-analysis evaluating the relationship between p16INK4a expression and HPV in ESCC by means of a random-effects model. (
Sensitivity analysis was performed to evaluate the stability of the pooled results. The pooled OR was found to range from 1.27 (95% CI: 0.58-2.84) to 2.32 (95% CI: 0.95-5.64). As shown in Figure 3A, the pooled results were very stable and no single article significantly influenced the pooled OR.

Sensitivity analyses of the summary odds ratio (ORs) to evaluate the stability of the meta-analysis. Every round indicates the pooled OR when the left study was omitted in the meta-analysis. The lengths of every broken line represent the respective 95% CIs. (
Association between p16INK4a Expression and HR-HPV Infection in ESCC
Six studies reported data regarding the relationship between p16INK4a expression and HR-HPV types (HPV16 or HPV18) in ESCC (18, 20-21-22, 24, 26). In these studies, p16INK4a was found in 45.1% of the HPV-positive and 37.4% of the HPV-negative specimens. Since significant heterogeneity was identified between studies (I2 = 89.6%, p<0.0001), the random-effects model was applied. As shown in Figure 2C, the pooled OR showed no significant relationship between p16INK4a expression and HR-HPV in ESCC (OR: 1.31, 95% CI: 0.26-6.59, p = 0.741). Owing to the significant heterogeneity between these studies, subgroup analysis was conducted again based on the HPV detection method to explore the sources of the heterogeneity. As shown in Figure 2D, no significant association between p16INK4a expression and HR-HPV in ESCC was found in either the PCR (OR: 0.95, 95% CI: 0.25-3.64, p = 0.940) or ISH group (OR: 2.58, 95% CI: 0.03-268.14, p = 0.689).
We conducted sensitivity analysis to assess the influence of each individual study. It indicated that the pooled OR did not vary substantially. As shown in Figure 3B, the pooled OR ranged from 0.69 (95% CI: 0.21-2.22) to 1.89 (95% CI: 0.33-10.86), suggesting that the pooled results were also stable regarding HR-HPV types.
Publication Bias
There was no evidence of any publication bias in our meta-analysis. As shown in Figure 4A and 4B, Begg's funnel plot in evaluating the relationship between p16INK4a expression and overall HPV types in ESCC was symmetrical (Begg's test p = 0.592), and the Egger test showed a p value of 0.722 (95% CI: -5.16-7.12). Begg's funnel plot in assessing the association between p16INK4a expression and HR-HPV in ESCC was also symmetrical (Begg's test p = 0.707), and the p value of the Egger test was >0.5 (p = 0.772, 95% CI: -13.41-16.79) (Fig. 4C, 4D). These results attested the absence of any obvious publication biases in the present meta-analysis.
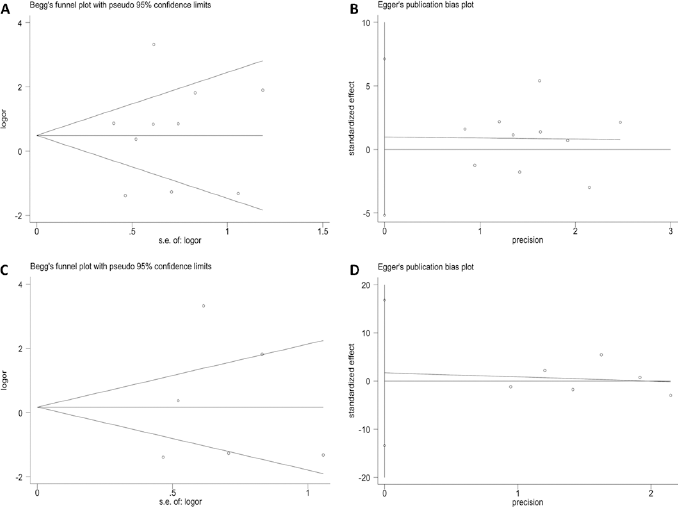
Begg's funnel plot of the present meta-analysis (
Discussion
p16INK4a is widely used as a surrogate marker for screening HPV infection in various squamous cell carcinomas (12, 16, 17, 13-14-15). However, there has been controversy about the detection of HPV in ESCC (18-19-20-21-22-23-24-25-26-27). We performed a meta-analysis of the available published literature regarding the potential association between p16INK4a expression and HPV-based ESCC. The results clearly ruled out any significant relationship between p16INK4a and HPV infection in ESCC. Notably, p16INK4a was not a reliable marker of HPV infection in ESCC.
Overall, p16INK4a was detected in 39.6% of the HPV-positive and 20.5% of the HPV-negative specimens when all HPV types were included. The result of the pooled OR (1.79, 95% CI: 0.69-4.66) that we obtained from the random-effects analysis strongly indicated there was no association between p16INK4a expression and HPV infection in ESCC. Additionally, owing to the significant heterogeneity between studies, sensitivity analysis was performed, which showed that the pooled OR was stable and no obvious change occurred when any individual article was omitted.
Numerous methods of HPV detection are used today, but the optimal testing method has yet to be clearly defined. Walline et al (33) conducted a study comparing several commonly used HPV assessment tools and showed that PCR with its low DNA requirement (5 ng) is effective for testing small tissue samples, high throughput screening, fast recognition of HPV types, and has high specificity and sensitivity; ISH on the other hand has high specificity among known HPV-positive tumors but comparatively low sensitivity and can miss HPV-containing tumors as assessed by other methods. Therefore, we performed stratified analyses based on the HPV detection methods. No significant differences were found between the PCR (OR: 1.65, 95% CI: 0.83-3.30, p = 0.154) and ISH groups (OR: 2.58, 95% CI: 0.03-268.14, p = 0.689).
More than 130 HPV types have been identified to date and these types have been classified into high-risk and low-risk genotypes (34). Previous studies showed that HR-HPV types, especially HPV16 and HPV18, were most strongly associated with ESCC (35-36-37-38). As mentioned previously, only 6 studies in our meta-analysis investigated whether HPV16/18 affected p16INK4a expression, and found p16INK4a in 45.1% of the HR-HPV-positive and 37.4% of the HR-HPV-negative specimens. Therefore, we also evaluated the relationship between p16INK4a expression and HPV16/18 infection in ESCC. When we conducted a subgroup analysis by HPV detection method, we found no statistical significance in either the PCR group or ISH group. Sensitivity analysis by omitting individual studies alternately indicated that the pooled OR was very stable. Furthermore, the quality of the included studies was judged adequate and the tests did not identify any publication bias, which indicated that the pooled results’ bias is probably negligible. All these observations support and strengthen our findings.
In 2013, Michaelsen et al (39) conducted a systematic review of the role of p16INK4a as a marker of transcriptionally active HPV in ESCC and the regional prevalence of HPV in ESCC. They collected 8 articles that were published between 2006 and 2012. In a pooled analysis with Fisher's exact test for the 8 studies providing p16INK4a data on both HPV-positive and HPV-negative specimens, the sensitivity of p16INK4a expression as a marker of HPV DNA was 0.35 and the specificity 0.67 (39). In comparison, 10 articles published between 2006 and 2014 were included in our study, with 985 ESCC specimens collected from more than 12 different countries or regions. A random-effects model was used to pool the OR to estimate the association between p16INK4a expression and HPV infection in ESCC. Our study first investigated the relationship between p16INK4a expression and HPV infection in ESCC through meta-analysis. Moreover, we assessed the influence of overall HPV types and HR-HPV on p16INK4a expression in ESCC. Additionally, we used the PRISMA checklist to improve the standardization of the present study and provide the detailed selection process of our meta-analysis. Collectively, neither overall HPV nor HR-HPV was related to p16INK4a expression in ESCC.
There are some limitations to the present analysis that need to be acknowledged. First, DNA was extracted from FFPE samples in the majority of the included studies. It is well known that FFPE tissues are a highly valuable source of genetic material for molecular analysis, but frequently genetic material in those samples is highly degraded, which influences the PCR amplication (40). Thus, it may be challenging to extract a sufficient number of DNA fragments and reduce the HPV positivity rate. Second, there was marked heterogeneity among the included studies, which might be explained by variations in the study population, geographic location, types of specimens and primers, and HPV detection method. To address this issue, we adopted the random-effects model to combine data and performed a meta-analysis stratified by HPV detection method. However, considerable heterogeneity remained when we performed subgroup analyses by HPV detection method. In addition, sensitivity analyses were conducted to test the stability of the pooled OR and the pooled OR proved very stable. Third, we could not exclude confounders that may affect the HPV prevalence in ESCC cases because few of the included studies provided information on confounders such as age, sex difference, smoking, alcohol consumption, financial situation, level of education, lifestyle and diet. Finally, we did not perform subgroup analyses by geographic location, study population, specimen type, and type of primers because several studies did not provide sufficient information. Further studies should focus on these issues and we will conduct further research to obtain more information on these aspects.
In conclusion, our results demonstrated no significant association between p16INK4a expression and HPV infection in ESCC, and showed that p16INK4a is not a reliable screening marker in HPV-associated ESCC. Most importantly, this meta-analysis provides useful information and important evidence for the diagnosis of HPV infection in ESCC in the future. However, further multicenter, large-sample and well-matched prospective studies are still required to illuminate the possible etiological roles of HPV in ESCC.
Footnotes
Acknowledgment
We are grateful to Zhi-Qiang Lu (School of Life Sciences, Lanzhou University, Gansu Province, China) for his advice on study design and data analysis.
Financial support: The study was not supported by any sources.
Conflict of interest: The authors declare that they have no conflict of interest.