
Abstract
Introduction
The aim of this investigation was to determine whether alterations in mitochondrial DNA (mtDNA) copy number in colon cancer were associated with clinicopathological parameters and postsurgical outcome.
Methods
By quantitative real-time PCR assay, the mtDNA copy number was detected in a cohort of colon cancer and matched adjacent colon tissues (n = 162).
Results
The majority of patients had higher mtDNA content in colon cancer tissues than matched adjacent colon tissues. Moreover, high mtDNA content in tumor tissues was associated with larger tumor size, higher serum CEA level, advanced TNM stage, vascular emboli, and liver metastases. Further survival curve analysis showed that high mtDNA content was related to the worst survival in patients with colon cancer at advanced TNM stage.
Conclusions
High mtDNA content is a potential effective factor of poor prognosis in patients with advanced stage colon cancer.
Introduction
Colon cancer is one of the most common malignant tumors; it was estimated that about 96,830 new cases and 39,590 colon cancer–related deaths occurred in the United States in 2014 (1). Colon cancer is the fifth cancer in China, and its incidence has shown a sharp increase over the last decade (2). Patients suffering from colon cancer are often diagnosed at an advanced stage, which results in a poor prognosis. Curative surgery is the major treatment strategy for colon cancer (3); however, high rates of distant metastasis and local recurrence lead to poor outcome after radical resection. Thus, there is a crucial need to establish novel postsurgical prognostic biomarkers with higher specificity and sensitivity for colon cancer.
Mitochondrial DNA (mtDNA) is a 16.6-kb, double-stranded circular DNA that contains an approximately 1.1-kb non-coding displacement loop (D-loop) region encompassing nucleotide position 16024-576, and modulates its own replication and transcription (4). Mitochondria are cytoplasmic organelles controlling the cell energy metabolism and cellular homeostasis, such as the generation of ATP via respiration and oxidative phosphorylation (OXPHOS), the production of reactive oxygen species (ROS), and cell apoptosis (5). Because of its lack of protection from histone proteins, inadequate DNA repair system, and exposure to high levels of ROS, mtDNA usually suffers from 10-fold higher damage or mutation than nuclear DNA (6). Damage or mutation of mtDNA can result in acceleration of ROS generation via impairment of the OXPHOS system and consequently enhance further DNA damage or mutation, which contributes to cancer initiation and progression (7). There is a growing body of studies showing alterations of mtDNA copy numbers in various cancers. For instance, the mtDNA copy number was found to be increased in laryngeal cancer tissues compared with normal laryngeal tissues (8). Zhang et al detected an association between increased mtDNA content in tumor tissues and poor survival in patients with late stage gastric cancer (9). Warowicka et al demonstrated that the mtDNA copy number increased during cervical cancer development in contrast to the matched tissues in the control group (10). However, the relationship between mtDNA copy number and postsurgical outcome of colon cancer patients remains unclear. In the present investigation, we measured the mtDNA content in 162 pairs of colon cancer and matched adjacent colon tissues, and analyzed the association between mtDNA copy number in tumor tissues, clinicopathological characteristics, and prognosis after surgery.
Methods
Patients and Specimens
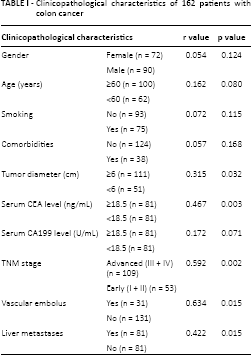
Written informed consent was obtained from all patients involved in this study. The ethics committee of the First Affiliated Hospital of Xian Jiaotong University approved all protocols according to the Helsinki Declaration of 1964 No. 20080331, 28 May 2008. A total of 162 colon cancer patients treated by surgical resection between 2009 and 2010 at the First Hospital of Xian Jiaotong University were recruited. None of the patients received chemotherapy or radiotherapy before surgery. Colon cancer and matched adjacent colon tissues (>2 cm distance from the resection margin) were collected during the operation and immediately stored in paraformaldehyde. The final diagnosis of colon cancer was confirmed by at least 2 senior pathologists at the Department of Pathology of the First Affiliated Hospital of Xian Jiaotong University according to the World Health Organization criteria. Clinical data were obtained from the medical records; the details are presented in Table I.
Clinicopathological characteristics of 162 patients with colon cancer
Dna Preparation
Colon cancer and adjacent normal tissues were dissected at 5 μm and then treated with xylene for 12 hours at 25°C to remove the paraffin. After that, tissues were digested with 1% sodium dodecyl sulfate and concentrated proteinase K at 48°C for 72 hours. Genomic DNA was isolated from the tissues followed by standard phenol-chloroform extraction and ethanol precipitation, and stored at -80°C until use (9).
mtDNA Copy Number Analysis
The mtDNA copy number was detected in the genomic DNA samples from 162 pairs of colon cancer and adjacent normal tissues by quantitative real-time PCR assay (qRT-PCR). The primers and TaqMan probes for the MT-ND1 and β-actin genes are described in Table II. PCR assays were performed in a reaction system of 20 μL with 67 mM Tris base, 2.5 mM MgCl2, 10 mM 2-mercaptoethanol, 0.1% DMSO, 0.2 mM each of dATP, dCTP, dGTP and dTTP, 16.6 mM ammonium sulfate, 600 nM each of primers, 200 nM TaqMan probe, 0.6 unit platinum Taq polymerase, and 2% Rox Reference Dye. Human leukocyte DNA was used to build the standard curve. β-actin was run in parallel to control for equal loading. The relative mtDNA copy number was obtained as described previously (9).
The sequences of primer and TaqMan probe in this investigation

Data Analysis and Statistics
Differences in mtDNA content between colon cancer tissues and adjacent colon tissues were compared by the Mann-Whitney U-test. The association between mtDNA in colon cancer tissues and clinical features was analyzed using Spearman's rank test. Multivariate models were then developed that adjusted for the most important covariates including gender, age, TNM stage, serum CEA and CA199 level, tumor diameter, and vascular emboli. The Kaplan-Meier survial curve was evaluated by the log-rank test to analyze differences in postsurgical outcome. Multivariate analysis was performed by means of SPSS v13.0 (SPSS Inc.), and the PRISM 4 software (GraphPad) was used for other statistical analyses.
Results
mtDNA Copy Number in Colon Cancer
The mtDNA content was investigated in tumor tissues and matched adjacent colon tissues from 162 colon cancer patients by qRT-PCR. mtDNA was found to be higher in tumor tissues than adjacent colon tissues in 135 of 162 (83.3%) patients (Fig. 1A). The relative mean mtDNA content was significantly higher in colon cancer tissues (10.20 ± 0.39 copies) than control colon tissues (4.80 ± 0.19 copies) (Fig. 1B; p<0.001). The median value of mtDNA in colon cancer tissues was 9.65 copies (range: 0.12-35.00 copies) versus 4.56 copies (range: 0.12-35.00 copies) in adjacent colon tissues. The mtDNA content in right-sided colon cancer with a mean value of 11.0 ± 0.52 copies was significantly higher than in adjacent colon tissues (4.6 ± 0.33 copies). Similar results were found for left-sided colon cancer, which showed 9.8 ± 0.73 copies vs. 5.1 ± 0.21 copies in adjacent control tissues.
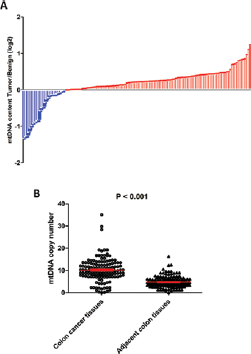
The mtDNA copy number was aberrantly increased in tumor tissues compared with adjacent colon tissues from 162 colon cancer patients. mtDNA content in tumor tissues was higher than in adjacent colon tissues in 135 (83.3%) patients (displayed by log2) (
Differences of mtDNA Copy Number in Colon Cancer Tissues with Diverse Clinicopathological Features
Next, we examined the mtDNA content in colon cancer tissues with different clinicopathological features. No significant difference in mtDNA content was observed between male and female patients (Fig. 2; p = 0.761). Similarly, no difference was found when the mtDNA content was compared between older (≥60 years) and younger patients (<60 years) (p = 0.445). Intriguingly, the mtDNA copy number was increased in colon cancer with a more malignant behavior. As shown in Figure 2, tumors with a greater diameter (≥6 cm) contained significantly more mtDNA than those with a smaller diameter (<6 cm) (p = 0.012). Patients at TNM stage III and IV had more mtDNA content than those at TNM stage I and II (p = 0.029). Using the median value of serum CEA (18.5 ng/mL) as the cutoff, the 162 patients were divided into 2 groups: a high CEA and a low CEA group. There were more mtDNA copies in tumor tissues from patients of the high CEA group than of the low CEA group (p = 0.048). The 162 colon cancer patients were also divided into a high CA199 group and a low CA199 group, where we chose the median value of serum CA199 (35.2 U/mL) as the cutoff point. Interestingly, there was no significant difference in mtDNA copy numbers in tumor tissues between the high CA199 group and low CA199 group (p = 0.055). There was more mtDNA content in tumors with vascular emboli than in those without vascular emboli (p = 0.002). Finally, after analyzing the follow-up data, we found that patients suffering from postsurgical liver metastases had higher mtDNA copy numbers than those without liver metastases (p<0.001).
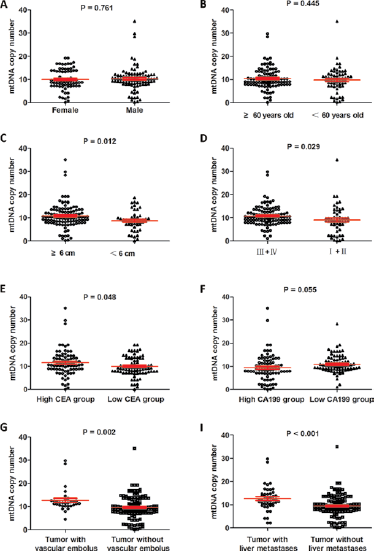
The Spearman rank test indicated no significant difference in mtDNA content between male and female patients (
Relationship of mtDNA Content to Clinicopathological Characteristics of Colon Cancer Patients
We examined the relationship between mtDNA copy number and clinicopathological features by Spearman's rank test. The mtDNA ratio of tumor/benign tissues was used as the cutoff and the 162 patients were divided into 2 groups: a high mtDNA group with more mtDNA in tumor tissues and a low mtDNA group with less mtDNA in tumor tissues. As shown in Table I, a higher mtDNA copy number in tumor tissues was positively associated with tumor diameter (r = 0.315, p = 0.032), higher serum CEA level (r = 0.467, p = 0.003), advanced TNM stage (r = 0.592, p = 0.002), vascular embolus (r = 0.634, p = 0.015), and liver metastases (r = 0.422, p = 0.015). However, there was no significant relationship of mtDNA copy number to other clinicopathological features including age (r = 0.162, p = 0.080), gender (r = 0.054, p = 0.124), smoking (r = 0.072, p = 0.115), comorbidities (r = 0.057, p = 0.168), and serum CA199 level r = 0.172, p = 0.071).
Association between mtDNA Copy Number in Tumor Tissues and Survival of Colon Cancer Patients after Surgery
To figure out whether mtDNA content was associated with prognosis after surgery in colon cancer patients, we collected follow-up information from 124 of the 162 patients (76.5%). The range of follow-up duration was 12 to 60 months, with a median of 42 months. The 124 colon cancer patients were classified into a high mtDNA group (n = 105) and a low mtDNA group (n = 19). The high mtDNA group included patients with higher mtDNA content in tumor tissues, whereas the low mtDNA group contained patients with a lower mtDNA copy number in tumor tissues compared to adjacent colon tissues. As shown in Figure 3A, although there was no significant difference in overall survival time between both groups (HR = 1.933; 95% CI 0.933-4.006; p = 0.076), there was a tendency for patients of the high mtDNA group to have a worse postsurgical outcome than patients from the low mtDNA group. In addition, the median survival time of patients in the high mtDNA group was 54 months versus 60 months in the low mtDNA group. In the right colon cancer group, patients with higher mtDNA content in tumor tissues had a worse prognosis after surgery compared with those having lower mtDNA in their tumor tissues (HR = 2.177; 95% CI 1.055-4.495; p = 0.035; Fig. 3B). A similar tendency was found in the left colon cancer group, even though the difference was not significant (HR = 2.366; 95% CI 0.653-8.575; p = 0.167; Fig. 3C). Based on the TNM stage, we categorized the 124 colon cancer cases with follow-up information into 2 groups: the early stage group (TNM I+II, n = 45) and the advanced stage group (TNM III+IV, n = 79). In the advanced stage group, there were 72 cases with higher mtDNA copy numbers in tumor tissues, which we referred to as the high mtDNA group, while the low mtDNA group was constituted by the remaining 7 cases with lower mtDNA content in tumor tissues. Comparison of the Kaplan-Meier survival curves showed that patients in the high mtDNA group had a worse prognosis than those in the low mtDNA group (HR = 2.526; 95% CI 1.043-6.116; p = 0.040; Fig. 3D). In the early stage group, the mtDNA copy number in tumor tissues was increased in 33 cases and decreased in the other 12 patients. No differences in outcome after surgery between the high mtDNA group and low mtDNA group were found after analysis of the Kaplan-Meier survival curves by the log-rank test (HR = 1.492; 95% CI 0.4753-4.683; p = 0.493; Fig. 3E). No significant difference in postsurgical complications was found in the comparison mentioned above.
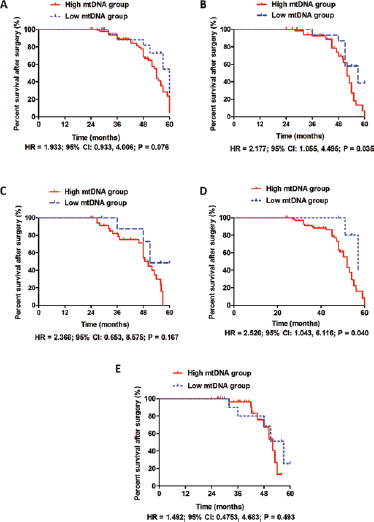
Patients in the high mtDNA group tended to have a worse postsurgical outcome than patients in the low mtDNA group, but there was no significant difference in overall survival time between the 2 groups (
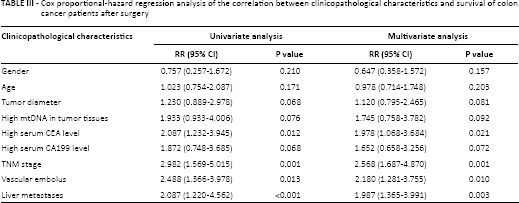
Furthermore, we used Kaplan-Meier survival curves to explore the impact of clinicopathological characteristics on the postsurgical prognosis of colon patients. As presented in Table III, univariate analysis showed that age, gender, tumor diameter and serum CA199 level did not affect the survival time after operation. High mtDNA content, high serum CEA level, advanced TNM stage, vascular embolus and liver metastases were identified as poor prognostic factors. Moreover, multivariate analysis showed that advanced TNM stage, vascular embolus and liver metastases were independent postsurgical prognostic factors for colon cancer patients.
Cox proportional-hazard regression analysis of the correlation between clinicopathological characteristics and survival of colon cancer patients after surgery
Discussion
Mitochondria are important cell organelles that regulate numerous biological processes including cell energy production (ATP/ROS), iron and calcium homeostasis, cell cycle, and apoptosis. Evidence has shown that dysfunction of mitochondria resulted in cardiovascular disease (11), kidney disease (12), and various cancers (12, 13). Human mtDNA includes the genes coding for 13 polypeptides of the respiratory chain, 2 rRNAs and 22 tRNAs, which contain the critical genetic information of mitochondria. Recent studies found frequent mutations in the D-loop of mtDNA modulating the replication and transcription of mtDNA in a variety of cancers, which was considered to result from the lack of introns, binding histone protein, exact DNA replication, and effective DNA repair system (14, 15). It has been demonstrated that dysfunction of mitochondria driven by mtDNA mutation promotes cancer development and progression via the massive production of ROS (16, 17). Altered mtDNA content is a characteristic of mtDNA mutation. However, different relationships between mtDNA copy number and tumor progression have been found in different cancers. Dang and colleagues examined the mtDNA copy number in 204 cases of laryngeal cancer and found that a low copy number of mtDNA was associated with worse survival in early stage disease (8). In addition, downregulation of mtDNA content was found in hepatocellular carcinoma (19), gastric cancer (20), breast cancer (9), and prostate cancer. By contrast, the mtDNA copy number was increased in esophageal squamous cell carcinoma (14), lung cancer with a smoking history, and head and neck cancer. Intriguingly, although the mtDNA content was found to be decreased in gastric cancer compared with normal gastric tissues, there was a strong association between increased mtDNA content and worse prognosis in patients at advanced stages of the disease.
There have been a few reports about mtDNA in colon cancer, reaching different conclusions. Most of them tried to elucidate the mechanism of aberrant mtDNA copy content in colon cancer (15-16-17), genetic changes in mtDNA (18), and the relevant single nucleotide polymorphism (19). Thyagarajan's group tested the mtDNA copy content in peripheral blood of colorectal cancer patients and controls free of colorectal cancer, and found a U-shaped correlation between the relative mtDNA copy number and the colorectal cancer risk (20). In the present investigation, mtDNA content was assessed in tumor samples and matched colon tissues from 162 patients with colon cancer using qRT-PCR. A higher mtDNA copy number was found in tumor tissues than matched adjacent colon tissues in 135 patients. Moreover, the mean mtDNA content was significantly higher in tumor tissues than adjacent colon tissues. These data suggested that the mtDNA copy number was aberrantly increased in colon cancer, a phenomenon that could be involved in colon carcinogenesis. This finding was different from those of the Van Osch group, probably due to the higher proportion of patients with KRAS-mutated tumors in that study (15). After analyzing the clinical features of 162 patients with colon cancer, we did not find a significant association of mtDNA content with gender and age. Although no relationship between serum level of CA199 and mtDNA content was found, there was a remarkable correlation between mtDNA copy number and more malignant characteristics including larger tumor size, advanced TNM stage, higher serum CEA level, vascular embolus, and liver metastases. The aforementioned results implied that increased mtDNA content could play an important part in colon cancer progression.
To figure out the impact of mtDNA copy number on postsurgical survival of colon cancer patients, we performed follow-up interviews and obtained relevant information from 124 of 162 cases. Comparison of Kaplan-Meier survival curves revealed a tendency for colon cancer patients with higher mtDNA content in tumor tissues to have a poor prognosis after surgery, though no significant difference was found. Furthermore, in patients at TNM stages III and IV, the higher mtDNA copy number in tumor tissues was associated with worse survival after surgery. Additionally, univariate analysis identified high mtDNA content, high serum CEA level, advanced TNM stage, vascular embolus and liver metastases as predictive factors for poor prognosis. Advanced TNM stage, vascular embolus and liver metastases were established as independent poor prognostic factors.
In summary, we examined the mtDNA copy numbers in a large cohort of patients with colon cancer and showed that mtDNA content was aberrantly increased in colon cancer tissues. High mtDNA copy number was associated with larger tumor size, advanced TNM stage, higher serum CEA level, vascular embolus, and liver metastases. Furthermore, a higher mtDNA copy number in tumor tissues predicted worse survival after surgery for patients at TNM stage III and IV. These findings indicated that a higher mtDNA copy number in colon cancer tissue compared with the adjacent colon tissue predicted poor outcome and a higher risk of metastases after surgery. Hence, mtDNA copy examination could become an important factor in the system of colon cancer staging.
Footnotes
Financial support: This investigation was supported by grants from the International Cooperation Program of Shaanxi Province (No. S2014kw428 to Shuixiang He), Key Science and Technology Program of Shaanxi Province (No. 2013JC2-21 to Xingmei Zhu), the National Natural Science Foundation of China (No. 81402186 to Xingmei Zhu), and a special grant from the Education Department of Shaanxi Province (No. 14JK1633 to Xingmei Zhu).
Conflict of interest: None of the authors has any conflict of interest related to this study to disclose.