
Abstract
Purpose
An imbalance between matrix metalloproteinases (MMPs) and tissue inhibitors of MMPs (TIMPs) appears critical for tumor progression and metastasis. This study aimed to determine whether gene expression of MMP1, MMP2, MMP9, TIMP1 and TIMP3 and the MMP/TIMP expression ratio in peripheral blood leukocytes (PBLs) and the MMP1 and TIMP1 contents or MMP1/TIMP1 ratio in plasma were associated with clinicopathological characteristics in invasive ductal carcinoma (IDC) of the breast.
Materials and methods
Blood samples were collected from women newly diagnosed with IDC who had not received prior treatment (n = 102). Gene expression in PBLs was analyzed by quantitative real-time polymerase chain reaction. Concentrations of MMP1 and TIMP1 in plasma were measured using ELISA.
Results
In univariate analysis the expression levels of MMP2 and TIMP1 mRNA were significantly higher in premenopausal compared to postmenopausal patients (p<0.001 and p = 0.014, respectively). MMP2 mRNA expression negatively correlated with age (p<0.001, r = -0.43). We found that the MMP2/TIMP3 expression ratio was significantly higher in women after menopause (p = 0.007). The MMP2/TIMP1 expression ratio was higher in human epidermal growth factor receptor 2 (HER2)-positive patients (p = 0.022). Low-grade tumors had significantly lower MMP1/TIMP1 and MMP2/TIMP1 expression ratios (p = 0.047 and p = 0.048, respectively). TIMP1 plasma concentration was significantly higher in small tumors compared with T2-T3 tumors (p = 0.013).
Conclusions
These findings reveal an important association between tumor characteristics and expression ratios of MMP1/TIMP1 and MMP2/TIMP1 in PBLs and TIMP1 concentration in plasma. Menopausal status may influence the mRNA expression levels of MMP2 and TIMP1 as well as the MMP2/TIMP3 expression ratio in IDC of the breast.
Introduction
Matrix metalloproteinases (MMPs) are able to cause proteolytic cleavage of a number of extracellular matrix (ECM) components (1). Overstimulation of MMP activity is required in tumor progression and metastasis (2). Since MMP activity is mainly regulated by specific tissue inhibitors of MMPs (TIMPs) (3), an imbalance between MMPs and TIMPs has been thought to play an important role in carcinogenesis. Numerous studies have found a correlation between the expression or activity of MMPs and TIMPs and a variety of clinicopathological features in tumor tissue, plasma or serum (4-5-6). Although MMPs and TIMPs are expressed also in many different blood cell types, relatively little is known about the role of MMP and TIMP mRNA expression in peripheral blood leukocytes (PBLs) of cancer patients.
Breast is the leading cancer site in women, accounting for 23% of the total cancer cases and 14% of the total cancer-related deaths (7). The most common type of invasive breast cancer (BC) is invasive ductal carcinoma (IDC), accounting for 72% of cases, followed by invasive lobular carcinoma (8).
Various MMPs are overexpressed in BC, causing cell migration and matrix degradation, thereby playing several roles in tumor invasion and metastasis (9). Because MMPs and TIMPs are expressed in many different blood cell types, their measurement in blood cells, specifically PBLs, may reflect cellular changes and may help to diagnose BC. Gene expression of MMPs and TIMPs in PBLs from patients with newly diagnosed IDC of the breast and its correlation with clinicopathological parameters such as age, body mass index (BMI), menopausal status, hormone receptor status, tumor stage, grade and lymph node metastasis (LNM) were not identified. Hence we carried out quantitative real-time polymerase chain reaction (qRT-PCR) measurements of MMP1, MMP2, MMP9, TIMP1 and TIMP3 mRNA expression levels as well as MMP/TIMP ratios. Additionally, we investigated the relationship between plasma concentrations of MMP1 and TIMP1 as well as the MMP1/TIMP1 ratio and clinicopathological features.
Materials and methods
Patients and Clinical Sample Collection
Polish Caucasian women with IDC of the breast were recruited between 2011 and 2013 from the Copernicus Memorial Hospital (Lodz, Poland). All blood samples (n = 102) were collected immediately before patients underwent surgery. The patients were enrolled into the study only if they had had no chemotherapy treatment. None of the patients showed evidence of any other malignancies at the time of diagnosis. The study design was approved by the ethics committee of the Nofer Institute of Occupational Medicine (Lodz, Poland) and informed consent was obtained from all patients.
Data regarding tumor characteristics at diagnosis were obtained from the Copernicus Memorial Hospital pathology reports. Histological grade was determined according to the TNM classification and grading system. For tumor grade, analysis was performed comparing well-differentiated tumors (G1) versus moderately and poorly differentiated tumors (G2-G3). Similarly, we divided other clinical-pathological features of the tumors into groups: tumor stage (T1 vs. T2-T3) and LNM (N0 vs. N1-N3).
The characteristics of the BC patients (age, BMI, smoking status, menopausal status and receptor status including estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) were extracted from Copernicus Memorial Hospital data and questionnaires. All personal identifiers were removed from the data.
The study included postmenopausal women who had undergone natural menopause and had their last menstrual bleeding at least 1 year previously, and premenopausal women who had regular periods over the preceding 12 months. For the smoking-stratified analyses, nonsmokers were defined as women who were not currently smoking and had not smoked in the last 5 years, and smokers were defined as those who were currently smoking. The information about hormone use concerned current users of exogenous hormones such as oral contraceptives or menopausal hormone therapy.
RNA Extraction and cDNA Synthesis
All blood samples were collected into EDTA tubes and transported to the lab at 4°C 2 to 6 hours after venipuncture. Leukocyte lysate was collected in a sterile microtube and stored at -70°C until RNA isolation. Total RNA was isolated using a RNeasy Mini Kit (Qiagen) according to the manufacturer's instructions. RNA was eluted in 30 µL RNase-free water and stored at -70°C until use. cDNA was synthesized from 250 ng of total RNA using the QuantiTect cDNA synthesis kit (Qiagen). Total RNA was reverse transcribed according to the manufacturer's protocol; the final volume of the reaction was 20 µL. Prepared cDNA was stored at -20°C for further expression analysis.
qRT-PCR Analysis
Expression analysis of the MMP1, MMP2, MMP9, TIMP1 and TIMP3 genes was performed using primers synthesized by Metabion international AG as well as the primers for glyceraldehyde 3-phosphate dehydrogenase (GAPDH) housekeeping gene. Real-time reactions were subjected to PCR amplification using primer sets for MMP1: 5’-CTG CTG CTG CTG CTG TTC-3’ and 5’-ACT TGC CTC CCA TCA TTC TTC-3’; MMP2: 5’-GGA GAT ACA ATG AGG TGA AGA AG-3’ and 5’-GAC GGC ATC CAG GTT ATC G-3’; MMP9: 5’-AAC CAA TCT CAC CGA CAG G-3’ and 5’-CGA CTC TCC ACG CAT CTC-3’; TIMP1: 5’-GGG CTT CAC CAA GAC CTA CA-3’ and 5’-TGC AGG GGA TGG ATA AAC A-3’; TIMP3: 5’-TGC AAC TCC GAC ATC GTG-3’ and 5’-AAG GGC CCC TCC TTT ACC-3’; and GAPDH: 5’-AGC CAC ATC GCT CAG ACA C-3’ and 5’-GCC CAA TAC GAC CAA ATC C-3’. Aliquots of 0.5 μL of cDNA were mixed with 5 μL of 2x FastStart SYBR Green Master (Roche Applied Science), 0.5 μL of each primer, and molecular-grade water in a final volume of 10 μL. All samples were amplified in duplicate. Amplification reactions were performed on a LightCycler 96 Real-Time PCR System using fast 96-well plates (Roche Diagnostics) as follows: initial denaturation at 95°C for 10 minutes, followed by 40 cycles at 95°C for 15 seconds, annealing at 60°C for 45 seconds, and extension at 72°C for 45 seconds. Melting-curve analyses were run immediately after cycling to verify the specificity of the reactions. The efficiency calibration curves were obtained using 5 randomly selected and pooled samples. Relative quantification of the target genes with endogenous GAPDH controls and efficiency correction were done according to the Pfaffl-based method with the Q-Gene application (10).
Enzyme-Linked Immunosorbent Assays (ELISA)
The concentrations of MMP1 and TIMP1 were analyzed in heparinized plasma. Plasma was obtained by centrifugation at 4000 rpm for 10 minutes and stored at -25°C until use. The concentrations of MMP1 and TIMP1 were measured by ELISA according to the protocol provided by the manufacturer (Boster Immunoleader). Samples were diluted 2-fold for MMP1 analysis and 25-fold for TIMP1 analysis. All sample analyses were performed in duplicate. A standard curve was prepared on each plate in duplicate.
Statistical Analysis
Expression data were log-transformed to achieve normal distribution. Nominal variables were specified as numbers with appropriate percentages, whereas continuous variables were presented as means with standard deviations. Chi-square tests were used to test associations between categorical variables. For pairwise comparisons of continuous variables, Student's t-test was used. Multivariate analyses were performed using linear regression models in order to adjust for covariates (ER, PR and HER2 status, smoking status, hormone use, tumor stage, tumor grade and LNM). A p value lower than 0.05 was considered statistically significant. Data were analyzed using the Statistica 12.0 software.
Results
Subject Characteristics
In Table I we show the clinicopathological characteristics of the patients with IDC of the breast. A total of 102 patients (59.4 ± 10.5 years of age) were enrolled in the study; 71.6% were nonsmokers (n = 73) and 18.6% were smokers (n = 19). Age was found to be positively correlated with BMI (27.6 ± 4.6) (p = 0.014, r = 0.26). Thirty-nine patients used hormones (38.2%) and 54 did not (52.9%). Most IDC patients were classified as ER positive (77.4%; n = 79) while a negative ER status was present in 21.6% (n = 22). Sixty-three (61.8%) patients were classified as PR positive while 36 (35.3%) were negative. Seventy-seven (75.5%) patients were HER2 negative while the HER2 positivity rate was 9.8% (10 patients).
Comparison of clinical and tumor characteristics of patients with IDC of the breast
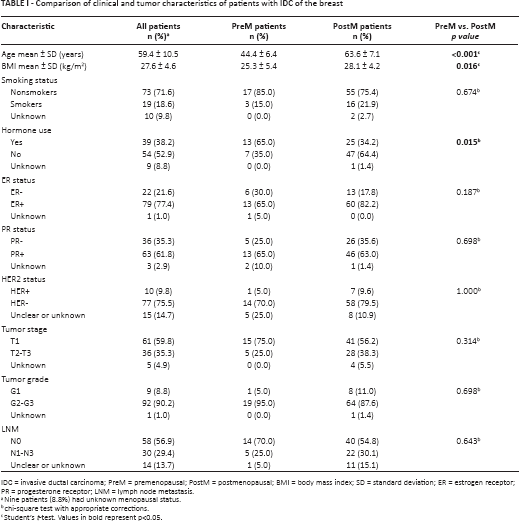
IDC = invasive ductal carcinoma; PreM = premenopausal; PostM = postmenopausal; BMI = body mass index; SD = standard deviation; ER = estrogen receptor; PR = progesterone receptor; LNM = lymph node metastasis.
Nine patients (8.8%) had unknown menopausal status.
chi-square test with appropriate corrections.
Student's t-test. Values in bold represent p<0.05.
Tumor stage was classified for most IDC patients as T1 (59.8%; n = 61); the remaining patients had T2-T3 tumors (35.3%; n = 36). G1 tumors were present in 9 patients (8.8%) and G2-G3 tumors in 92 patients (90.2%). Fifty-eight patients (56.9%) were classified as N0 and 30 patients (29.4%) as N1-N3.
Ninety-three patients (91.2% of all patients) were divided into 2 groups according to their menopausal status: the first group consisted of 73 postmenopausal patients (63.6 ± 7.1 years of age) and the second group of 20 premenopausal patients (44.4 ± 6.4 years), while 9 patients (8.8%) had an unknown menopausal status. There were statistically significant differences between postmenopausal and premenopausal patients in age distribution and hormone use (p<0.001 and p = 0.015, respectively). Comparison of BMI indicated that postmenopausal patients were more obese than premenopausal patients (p = 0.016). There were no differences in smoking status between premenopausal and postmenopausal patients (p = 0.469). Premenopausal and postmenopausal patients showed no differences in ER, PR and HER2 status (p = 0.187, p = 0.698, p = 1.000, respectively) or in tumor stage, tumor grade and LNM (p = 0.314, p = 0.698, p = 0.643, respectively).
Association between MMP and TIMP mRNA Expression, MMP/TIMP Expression Ratio and Clinicopathological Features
We performed analyses to evaluate the association of mRNA expression of MMP1, MMP2, MMP9, TIMP1, TIMP3 and the MMP/TIMP expression ratio with clinicopathological characteristics such as menopausal status, smoking status, hormone use, receptor status, tumor stage, tumor grade and LNM.
Univariate analysis showed an association between mRNA expression of MMP2 and TIMP1 and menopausal status. MMP2 and TIMP1 mRNA expression was higher in premenopausal patients than postmenopausal patients (p<0.001 and p = 0.014, respectively). The analysis showed that age was negatively correlated with MMP2 mRNA expression (p<0.001, r = -0.43). A similar but less strong tendency was observed for TIMP1 expression (p = 0.061, r = -0.21). However, multivariate analysis adjusted for ER, PR and HER2 status, smoking status, hormone use, tumor stage, tumor grade and LNM showed no significant association between mRNA expression of MMP or TIMP and menopausal status (Tab. II).
Association between expression of MMP and TIMP mRNA and menopausal status in patients with IDC of the breast
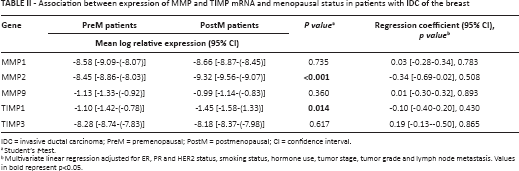
IDC = invasive ductal carcinoma; PreM = premenopausal; PostM = postmenopausal; CI = confidence interval.
Student's t-test.
multivariate linear regression adjusted for ER, PR and HER2 status, smoking status, hormone use, tumor stage, tumor grade and lymph node metastasis. Values in bold represent p<0.05.
No associations were found between mRNA expression of MMP1, MMP2, MMP9, TIMP1 or TIMP3 and clinical features (smoking status, hormone use, receptor status) and tumor characteristics (tumor stage, grade and LNM) (data not shown). Multivariate analysis of different clinicopathological features showed no significant association with mRNA expression of MMP1, MMP2, MMP9, TIMP1 and TIMP3.
Additionally, we demonstrated that the MMP2/TIMP3 ratio was significantly lower in premenopausal patients than postmenopausal patients (p = 0.007). Multivariate analysis showed no significant association between MMP/TIMP ratio and menopausal status (Tab. III). Univariate analysis showed that low-grade (G1) tumors had significantly lower MMP1/TIMP1 and MMP2/TIMP1 ratios (p = 0.047 and p = 0.048, respectively) than G2-G3 tumors (Fig. 1). Additionally, the MMP2/TIMP1 ratio was higher in patients with positive HER2 status (p = 0.022). No association was found for MMP/TIMP expression ratio and smoking status, hormone use, ER status, PR status, tumor stage and LNM (data not shown). Multivariate analysis of different clinicopathological features show no significant association with MMP1/TIMP1, MMP1/TIMP3, MMP2/TIMP1, MMP2/TIMP3, MMP9/TIMP1 and MMP9/TIMP3 expression ratios.
Association between MMP/TIMP expression ratios and menopausal status in patients with IDC of the breast
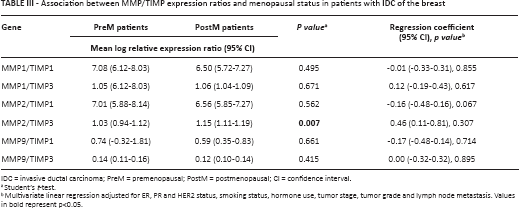
IDC = invasive ductal carcinoma; PreM = premenopausal; PostM = postmenopausal; CI = confidence interval.
Student's t-test.
multivariate linear regression adjusted for ER, PR and HER2 status, smoking status, hormone use, tumor stage, tumor grade and lymph node metastasis. Values in bold represent p<0.05.
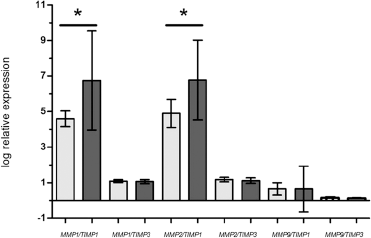
Association between mRNA expression ratio and tumor grade (MMP1/TIMP1 p = 0.047; MMP2/TIMP1 p = 0.048). The bars and whiskers represent mean log relative expression ± SD. Light gray bars indicate G1 and dark gray bars indicate G2-G3.
Association between Plasma MMP1 and TIMP1 Concentrations, MMP1/TIMP1 Concentration Ratio and Clinicopathological Features
Univariate and multivariate analyses were done to evaluate the association of the MMP1 and TIMP1 concentrations in plasma and MMP1/TIMP1 ratio with clinicopathological characteristics such as menopausal status, smoking status, hormone use, receptor status, tumor stage, tumor grade and LNM.
No associations were found between plasma MMP1 and TIMP1 concentrations, the plasma MMP1/TIMP1 concentration ratio and menopausal status. However, the mean MMP1 levels were higher in premenopausal patients (0.51 ± 0.23 ng/mL) than postmenopausal patients (0.45 ± 0.16 ng/mL) (p = 0.281). The mean plasma concentration of TIMP1 in premenopausal patients was 57.0 ± 25.9 ng/mL compared to 59.6 ± 27.7 ng/mL in postmenopausal patients. Multivariate analysis adjusted for ER, PR and HER2 status, smoking status, hormone use, tumor stage, tumor grade and LNM showed no significant differences when the 2 groups of women, postmenopausal and premenopausal, were compared for MMP1 and TIMP1 concentrations and MMP1/TIMP1 concentration ratio in plasma (data not shown).
The concentration of TIMP1 was found to be higher in small tumors (T1) than in T2-T3 tumors (64.4 ± 27.0 ng/mL vs. 48.3 ± 24.8 ng/mL, p = 0.013) (Fig. 2). No associations were found between the concentrations of MMP1 and TIMP1 and smoking status, hormone use, receptor status and LNM (data not shown). Multivariate analysis of different clinicopathological features revealed no significant association with MMP1 and TIMP1 concentrations or with the MMP1/TIMP1 concentration ratio.
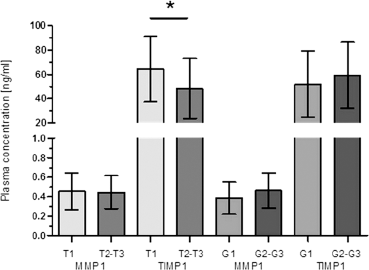
Association between plasma concentrations of MMP1 and TIMP1 versus tumor stage (TIMP1 p = 0.013) and tumor grade. The bars and whiskers represent mean plasma concentrations ± SD.
Discussion
Numerous studies have shown the relationship between the levels of MMPs and TIMPs in tissue, serum or plasma and cancer progression (11-12-13-14-15). The upregulation of MMP and TIMP mRNA expression in BC tissue and body fluids of BC patients results in the induction of tumor invasion and metastasis (16-17-18-19-20). However, no studies are available on the association between mRNA expression of MMPs and TIMPs and clinicopathological characteristics in PBLs from patients with IDC of the breast. In our opinion, differences in the formation of gene products that may reflect changes in interactions at different stages of cancer should be taken into consideration. It is known that the analysis of overexpressed genes in cancer may open a new possibility to improve diagnosis, predict clinical outcome, and provide a potential target for therapeutic intervention in tumor growth. Therefore, mRNA studies have gained the interest of researchers.
To test the potential clinical value of MMP and TIMP mRNA expression in PBLs of patients with IDC, we investigated the association between MMP1, MMP2, MMP9, TIMP1 and TIMP3 mRNA expression and clinicopathological features such as age, BMI, smoking status, hormone use, menopausal status, receptor status, tumor stage, tumor grade and LNM. Moreover, we examined the relationship between the concentration of MMP1 and TIMP1 in plasma and clinicopathological features.
The expression of MMPs is regulated by tumor cells to degrade ECMs and release ECM-bound growth factors, thereby allowing them to cross multiple tissue boundaries (21). It should not be forgotten, however, that MMPs and TIMPs are expressed in many different blood cell types and can be easily determined in blood (22). Moreover, measurement of the mRNA expression level compared to the protein concentration may provide a more accurate measure.
Some studies have shown that alterations of MMP expression in blood cells may provide important information about cell behavior. Vijayalakshmi et al (23) found a relationship between the activity of MMPs and the activity of mononuclear blood cells in inflammation. Bar-Or et al (24) have conducted comprehensive profiling of MMPs and TIMPs in leukocytes, and suggest that high expression of MMPs and TIMPs plays a role in high migratory capacity of monocytes.
A few studies have indicated that elevated levels of mRNA of MMPs in BC tissue are associated with poor outcome (16, 17). McGowan and Duffy showed an association between mRNA expression of certain MMPs and adverse outcome in patients with BC (25). Our results have demonstrated that moderately and poorly differentiated tumors are associated with high mRNA expression of MMP1/TIMP1 ratio and MMP2/TIMP1 ratio in PBLs from IDC patients. Moreover, tumor stage may modulate the concentration of TIMP1 in plasma. On the other hand, we have shown in this study that gene expression of MMP1, MMP2, MMP9, TIMP1 and TIMP3 and the MMP/TIMP ratio are not related to tumor stage or LNM.
Some authors (26, 27) observed increased expression and activity of MMPs during senescence and cancer development. Epidemiological studies have shown that risk factors for BC such as age and endocrine factors are altered in different menopausal statuses (28). The results of our and other authors’ studies show that postmenopausal and premenopausal groups differ in age and BMI. Postmenopausal women were older and had a higher BMI, but the women did not differ in their tumor characteristics. To find out if age-related menopausal changes may bring about changes in mRNA expression, we investigated the effect of menopausal status on the expression of MMP and TIMP and the MMP/TIMP ratio by comparing premenopausal versus postmenopausal women. The results obtained in our study showed significantly higher gene expression of MMP2 and TIMP1 in PBLs of premenopausal compared to postmenopausal patients. Because changes in menopausal status are age related, it is clear that in our analyses mRNA expression of MMP2 correlated also with age. A similar pattern was reported by Laird et al in endometrial adenocarcinoma (29). In another study Shynlova et al (30) observed that the expression levels of MMP2 and TIMP1 were increased in premenopausal compared with postmenopausal healthy women. Moreover, the expression of MMP2 and MMP9 in endometrial polyps was significantly higher in premenopausal patients than in postmenopausal patients (31). In our study, hormone use differed between premenopausal and postmenopausal patients, but we did not observe any association between mRNA expression and hormone use.
It is considered that maintaining a balance between MMP and TIMP controls the efficiency of proteolytic ECM degradation. Recent studies have demonstrated the usefulness of 2-gene expression ratio for the prediction of clinical outcome in BC patients (32, 33). Moreover, the MMP/TIMP ratio has been implicated in diseases like asthma, endometriosis and BC (11, 34, 35). MMP/TIMP imbalance also through abnormalities of the expression of these genes may lead to loss of homeostasis in the production and degradation of ECMs. This may suggest the potential impact of the MMP/TIMP expression ratio on cancer progression. Consequently, our next goal was to compare the MMP/TIMP expression ratio and clinicopathological parameters. We hypothesized that a disordered MMP/TIMP ratio might represent aggressiveness of BC. In this paper we demonstrate that the MMP1/TIMP1 and MMP2/TIMP1 mRNA expression ratios were significantly related to tumor grade. Additionally, our study showed that the MMP2/TIMP3 expression ratio was significantly associated with menopausal status. A reduced MMP2/TIMP3 expression ratio has been observed in premenopausal patients, due to the importance of the balance between these 2 proteins.
Conclusion
Taken together, the results of the present study support a role of MMP and TIMP mRNA expression in PBLs of patients with IDC of the breast. These findings reveal an important association between MMP1/TIMP1 and MMP2/TIMP1 expression ratios in PBLs and the concentration of TIMP1 in plasma and tumor characteristics. Moreover, the mRNA expression levels of MMP2 and TIMP1 and the MMP2/TIMP3 expression ratio may be regulated by menopausal status.
Footnotes
Acknowledgment
We would like to thank Stefan Markiewicz for the English editing of the manuscript.
Abbreviations
Financial support: This work was supported by the Nofer Institute of Occupational Medicine (internal grants No. 1.7/2011, No. 1.2/2012-2014 and No. 1.7/2012-2014).
Conflict of interest: The authors declare they have no conflict of interests related to this work.