
Abstract
Purpose
BAT-26 is one of the representative markers for microsatellite instability evaluation and presents different polymorphisms in different ethnic populations. The current knowledge of its comparative polymorphism between healthy individuals and cancer patients in the Chinese population is insufficient. This study aims to analyze germline polymorphic variations of BAT-26 between healthy individuals and cancer patients in Chinese from Jiangsu province and the associated cancer risk implications.
Methods
The various BAT-26 alleles and their percentages in cervical cells from 500 healthy women were assessed by direct sequencing. Twenty of these samples were also analyzed by fragment analysis. BAT-26 of blood DNA from 24 healthy individuals and 247 cancer patients was analyzed by fragment analysis.
Results
Compared with the sequencing results, 122.6-122.9 bp, 123.4-123.8 bp and 124.1-124.8 bp corresponded to the A25, A26 and A27 alleles, respectively. The 524 healthy individuals showed 4.58%, 92.18% and 3.24% of A25, A26 and A27, respectively. The variant alleles A18, A24, A28, A29 and A32 were only found in cancer patients, accounting for 0.81%, 0.40%, 0.40%, 0.40% and 0.40%, respectively; the A25, A26 and A27 alleles in cancer patients accounted for 6.48%, 77.33% and 13.77%.
Conclusions
Healthy individuals had a stable BAT-26 profile within the quasimonomorphic variation range (QMVR), but cancer patients harbored variant alleles outside QMVR and showed a trend from quasimonomorph to polymonomorph, suggesting that variant alleles of BAT-26 in germline cells may be regarded as a potential marker of higher cancer risk in the Chinese population from Jiangsu province.
Introduction
Lynch syndrome (LS) is an autosomal dominant inheritance syndrome characterized by a high incidence of early onset colorectal cancer (CRC) and extracolonic malignancies such as endometrial, ovarian, small bowel, urinary tract, hepatobiliary tract, gastric and brain cancers (1-2-3). LS is also referred to as hereditary nonpolyposis colorectal cancer (HNPCC) and accounts for 2% to 5% of all cases of CRC (3).
It has been shown that LS is the result of germline mutations in genes involved in DNA mismatch repair (MMR) including MSH2, MLH1, MSH6 and PMS2 (3). A defective MMR system usually shows microsatellite instability (MSI) (2). So MSI analysis is effective for the diagnosis of LS (4, 5). MSI is also considered a predictive biomarker of response to 5-fluorouracil, irinotecan and other chemotherapeutic agents (5-6-7-8-9). BAT-26 is one of the 5 markers of the MSI panel (BAT-25, BAT-26, D2S123, D5S346 and D17S250) recommended by the National Cancer Institute (NCI) because it has shown particularly high sensitivity and specificity in the detection of an MSI phenotype (4, 10). Zeinalian et al (11) found BAT-26 to be the most instable marker in selected CRC patients at risk of LS in central Iran.
BAT-26 is located downstream of exon 5 in the MSH2 gene and consists of poly-A nucleotide repeats (10). Its apparent, though not total, lack of polymorphism is remarkable (10, 12). For Chinese, it shows quasimonomorphism in germline cells and BAT-26-positive gastric cancers have distinct clinicopathological features (13). However, our knowledge of the comparative polymorphism of BAT-26 between healthy individuals and cancer patients is limited. In the present study we detected the polyadenine repeats of BAT-26 in healthy individuals and cancer patients from Jiangsu province, China, by sequencing and fragment analysis assay. We investigated the variant alleles and compared the basic polymorphism of this locus between these 2 groups.
Materials and methods
Samples
Cervical cells from 500 healthy women and blood from 24 healthy individuals (16 men and 8 women) as well as 247 patients (145 men and 102 women) with gastrointestinal or endometrial cancer from Jiangsu province were studied. All participants gave their informed consent for participation in the study and the outline of the study was approved by the institutional review board of the Affiliated Hospital of Nanjing University of Traditional Chinese Medicine. BAT-26 in cervical cells from 500 healthy women was analyzed by direct sequencing and 20 of the samples were also studied by fragment analysis. BAT-26 in blood from 24 healthy individuals and 247 patients with gastrointestinal or endometrial cancer was analyzed by fragment analysis (14).
Dna Isolation
DNA of cervical cells was extracted with an OMEGA tissue DNA kit (OMEGA bio-tek) and DNA of blood was extracted with an OMEGA blood DNA kit according to the manufacturers’ instructions, and then examined by agarose gel electrophoresis (14) for DNA extraction quality control.
PCR and Sequencing
The forward primer was 5’ ATC ACT GTC TGC GGT AAT CA 3’ and the reverse primer was 5’ AGG AGG GGA GAG AAA AAT AC 3’. PCR was performed (14) in a 20-μL reaction mixture of 20-100 ng DNA (1 μL), 10 × PCR buffer 2 μL (QIAGEN), HotStarTaq DNA polymerase 0.25 μL (QIAGEN), Q solution 4 μL (QIAGEN), 2 mM dNTPs 2 μL (Promega), forward primer (10 μM) 1 μL, reverse primer (10 μM) 1 μL, and water 8.75 μL. BAT-26 was amplified by an ABI 2700 (Applied Biosystems) thermocycler in the following thermal cycle profile: denaturation at 95°C for 15 minutes, 10 cycles of denaturation at 94°C for 50 seconds, annealing at 56°C-60°C (Touchdown PCR) for 1 minute, and extension at 72°C for 1 minute; 30 cycles of denaturation at 94°C for 50 seconds, annealing at 56°C for 1 minute, and extension at 72°C for 1 minute, followed by extension at 72°C for 10 minutes. PCR products were purified and sequenced on an ABI Prism 3100-Avant DNA analyzer following the reference (14). Some uncertain results were examined by forward/reverse sequencing.
Fluorescence PCR and Fragment Analysis
Forward primer: TGA CTA CTT TTG ACT TCA GCC-3’; the 5’ end was labeled with VIC fluorescent dye. Reverse primer: AAC CAT TCA ACA TTT TTA ACCC-3’. A tail consisting of the 7-base sequence GTTTCTT was added onto the 5’ end of the reverse primer.
Fluorescence PCR was performed (14) in a 20-μL reaction mixture including True Allele PCR Mix 15 μL (Applied Biosystems), Primer Mix 4 μL (Applied Biosystems) and 20-100 ng DNA (1 μL). The PCR thermal cycle profile was as follows: denaturation at 95°C for 15 minutes, 35 cycles of denaturation at 94°C for 50 seconds, annealing at 55°C for 1 minute and extension at 72°C for 1 minute, followed by extension at 72°C for 25 minutes. Fragment analysis of the PCR products was performed on an ABI Prism 3100-Avant DNA analyzer following the reference (14).
A blank, a negative control (A25) and a positive control (A26) were assayed in parallel with each series of samples for PCR, sequencing and fragment analysis quality control. The sequencing results were compared with standard sequence in NCBI nucleotide databases (GenBank accession number BD271286.1). Five samples with A25, 10 samples with A26, and 5 samples with A27 (total 20 samples of cervical cells) were analyzed by sequencing and fragment analysis to establish the relation between adenine repeats in BAT-26 and fragment length.
Results
BAT-26 of 771 samples was successfully amplified. Compared with the results of sequencing, the more frequent allele lengths were 122.6-122.9 bp, 123.4-123.8 bp and 124.1-124.8bp, respectively, consistent with the 25 poly(A) (A25), A26 and A27 alleles. The sequence of BAT-26 is shown in Figure 1. The typical relation between fragment length and adenine repeats at the BAT-26 locus is shown in Figure 2.
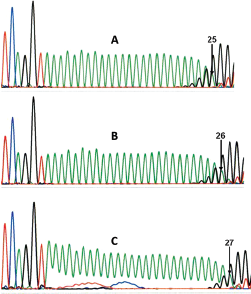
Electropherograms of the sequence at the BAT-26 locus. Allelic pattern of 25 (
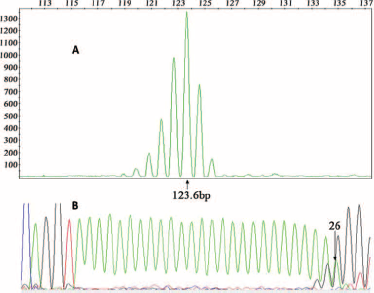
Relation between fragment length and adenine repeats at the BAT-26 locus. Fragment length (
The 524 healthy individuals and 247 cancer patients showed different alleles and percentages at the BAT-26 locus (Tab. I). Collating the variation range (8, 12), we found that the quasimonomorphic variation range (QMVR) of BAT-26 was A25, A26 and A27. BAT-26 of the 524 healthy individuals demonstrated a stable profile with a QMVR of A25-A27; no allele outside the range was found. For the 247 cancer patients, BAT-26 showed 97.58% inside the QMVR and 2.42% (3 women and 3 men) outside the QMVR.
Allele numbers and percentages of BAT-26
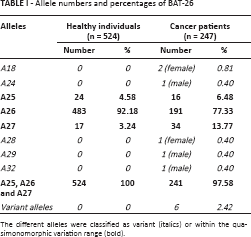
The different alleles were classified as variant (italics) or within the quasimonomorphic variation range (bold).
Discussion
MSI and its panel gene BAT-26 have been widely studied in HNPCC (15, 16), ordinary hereditary CRC (15), sporadic CRC (17), endometrial carcinoma (18) and gastric cancer (19). Vaniawala et al (20) explored whether all 5 markers proposed by the NCI (BAT-25, BAT-26, D2S123, D5S346 and D17S250) are suitable for CRC screening in the Indian population. They found that BAT-26 was the third most sensitive marker of the 5; D17S250 and BAT-25 were not informative enough and should be avoided for diagnosing LS in the Indian population. Zeinalian et al (11) studied the molecular and clinicopathological features of Iranian CRC patients at risk for LS by MSI testing and immunohistochemical staining. In their study BAT-26, MON0-27, NR-21 and NR-24 were analyzed to evaluate MSI status and the results showed that BAT-26 was the most instable quasimononucleotide marker.
The authors of the above research aimed to study MSI and patterns of variation in markers or molecular and clinicopathological features using the BAT-26 locus in cancer patients, especially HNPCC patients, but showed less interest in the polymorphism of BAT-26. Polymorphism of BAT-26 of populations worldwide including the Chinese population was reported by Campanella et al (8), Buhard et al (12), Lu et al (13), Pyatt et al (21), Berginc et al (22) and Cossio et al (23). However, less attention was paid to the difference in BAT-26 polymorphism between healthy individuals and cancer patients. In this study we investigated the polymorphism of BAT-26 in healthy individuals and cancer patients from Jiangsu province.
LS is an inherited disorder caused by germline mutations in the DNA mismatch repair genes and the disorder increases the risk of various cancer types, particularly CRC and endometrial cancer (24). So CRC and endometrial cancer patients were included and combined as one group in our study.
Usually white blood cells or lymphocytes are used as germline cells to study the polymorphism of genes (12), but also normal tissues are used (17); therefore, blood and cervical cells of healthy women were used in this research.
Fragment analysis and DNA sequencing (25) are standard techniques for MSI detection (14). Fragment analysis costs more than sequencing, but its operation procedure is easier and takes less time. Also, the results of fragment analysis are easier to read. We established the relation between fragment length and adenine repeats in BAT-26 in this study.
As mentioned above, the QMVR of BAT-26 is A25 to A27. We considered every allele less than A25 or greater than A27 as a variant. In the 524 healthy individuals in this study, BAT-26 was stable, with the quasimonomorphic alleles A25, A26 and A27 accounting for 4.58%, 92.18% and 3.24%, respectively. Conversely, the variant alleles A18, A24, A28, A29 and A32, besides the QMVR alleles A25, A26 and A27, were observed in the 247 cancer patients. The percentages of the variant alleles A18, A24, A28, A29 and A32 were 0.81%, 0.40%, 0.40%, 0.40% and 0.40%, respectively, while A25, A26 and A27 accounted for 6.48%, 77.33% and 13.77%, respectively. Obviously, in cancer patients the QMVR percentage (97.58%) decreased, especially that of A26, while the percentage of other alleles increased. It appears that in germline cells BAT-26 conserves its quasimonomorphic nature (12, 13) similar to BAT-25 (14) in healthy individuals, and shows a trend from quasimonomorph to polymonomorph in cancer patients, although variant alleles show a low incidence; this corresponded to the trend of BAT-25, whose variant alleles were more likely to be found in blood from cancer patients than healthy individuals (14). These results seem to suggest that variant alleles of BAT-26 in germline cells may be regarded as a potential marker of higher cancer risk in the Chinese population from Jiangsu province.
Among the 524 healthy individuals, 500 healthy women gave informed consent to use cervical cells and the other 24 healthy individuals gave informed consent to use blood for the study. In the 500 healthy women, A25, A26 and A27 accounted for 4.6% (23/500 × 100%), 92% (460/500 × 100%) and 3.4% (17/500 × 100%), respectively; the other 24 healthy individuals showed 4.17% (1/24 × 100%), 95.83% (23/24 × 100%) and 0% (0/24 × 100%) of A25, A26 and A27, respectively. Though it seems that there may be a difference in the frequency of A26 and A27 between the cervical cells from the 500 healthy women and blood from the other 24 healthy individuals, in all healthy controls BAT-26 showed a profile with a QMVR of A25-A27 and no variant allele was found. Also, the difference should be checked by collecting and testing more blood samples because the number of blood samples in the present study was relatively small.
Polymorphisms of BAT-26 in different ethnic groups were investigated by Campanella et al (8), Buhard et al (12), Lu et al (13), Pyatt et al (21), Berginc et al (22) and Cossio et al (23). These studies showed that different ethnic groups presented different frequencies of QMVR and variant alleles at the BAT-26 locus, though this locus conserved its quasimonomorphic nature. In a population from southeast Brazil, 3.23% of healthy individuals had variant alleles outside the QMVR range (8), whereas 6% of healthy individuals from Rio Grande do Sul in Brazil showed variant alleles at the BAT-26 locus (23). Buhard et al (12) found that the percentages of QMVR and variant alleles of BAT-26 from 55 different populations worldwide were 98.78% and 1.22%, respectively. Subsaharan Africans showed variant alleles above or approaching 10% for BAT-26, and none of the other geographic regions reached a frequency of 10% variant alleles (12). Biaka Pygmies from the Central African Republic, Bantu from South Africa, Yoruba from Nigeria, Bantu from Kenya, Pima from Mexico, Ashkenazim from Israel, Maya from Mexico, Balochis from Pakistan, and Palestinians from Israel showed variant alleles in 15.3%, 12.5%, 12.5%, 9.1%, 8.0%, 2.1%, 2.1%, 2.0%, and 1.0%, respectively (12). No variant alleles were identified in 423 genomic DNAs from blood of 389 healthy individuals and normal mucosa of 34 gastric cancer patients from Zhejiang province (13). Pyatt et al (21) identified allelic variations in the size of the poly(A) tract at BAT-26 in 12.6% of 103 healthy African-Americans. Berginc et al (22) reported that BAT-26 is quasimonomorphic in the Slovenian population, with a frequency of polymorphisms of 1.4%. Compared with the BAT-26 polymorphisms in these populations, our results showed that both healthy individuals and cancer patients in the Chinese population from Jiangsu province also conserved the quasimonomorphic nature at this locus, but the frequency of QMVR and variant alleles was different from those of Subsaharan Africans, Bantu, Pima, African-Americans (21) and Brazilians (8, 23), and closer to those of Ashkenazim, Maya, Balochis, Palestinians (21) and Slovenians (22). The healthy individuals from Jiangsu province showed no variant alleles and all BAT-26 within QMVR, which is consistent with those from Zhejiang province. But the frequencies of QMVR and variant alleles of cancer patients from Jiangsu province were 97.58% and 2.42%, which was different from those (no variant alleles) from Zhejiang province (13), even though these 2 populations were from neighboring provinces of China.
LS is caused by germline mutations in MMR genes including MLH1, MSH2, MSH6, PMS1 and PMS2, genes that normally ensure that all genetic information is copied correctly during DNA replication (2, 3, 25). Colon cancer arising in patients with a defective MMR system usually shows MSI, determined by the occurrence of frameshift mutations in simple sequence repeats (2). Large changes in microsatellite number in certain tumor tissue shows no normal function on DNA repair (26). MSI is a marked phenotypic characteristic of HNPCC, where it is found in 80%-90% of tumors, while it is present in up to 15% of sporadic cases (26).
MSI and MMR gene status are associated with clinical stage, disease outcome (27, 28) and response to chemotherapeutic agents (5-6-7-8-9, 27), but there are no reports on the relationship between BAT-26 polymorphisms, clinical stage and disease outcomes. Consistent data indicate that deficient DNA mismatch repair (dMMR)/MSI tumors have a better stage-adjusted survival than proficient MMR or microsatellite-stable (MSS) tumors, and may respond differently to 5-fluorouracil-based adjuvant chemotherapy (27). The results of the study by Szentirmay et al (28) showed that they could recognized MSS/MSI-low carcinomas, HNPCCs and sporadic MSI-high tumors with high probability on the basis of clinicopathological features like patient age, tumor localization, clinical stage and histological characteristics of CRCs, even if the genetic MSI test was not available. Our study was the first to compare the frequency of QMVR and variant alleles of BAT-26 between healthy individuals and cancer patients. Though the rare candidate variants make it difficult to examine whether these genetic variations are associated with clinical stage or outcome in cancer patients, the results help us understand more about the different polymorphisms of BAT-26 between healthy individuals and cancer patients and the cancer risk implications for the local Chinese, because BAT-25 also showed a similar trend from QMVR to polymorphic in our previous study (14).
It is controversial whether MSI is related to gender, and little has been written about the relationship between BAT-26 polymorphism and gender (13, 29, 30). Research by Umeto et al (29) showed that the overall frequencies of epithelial MSI in the left colon were significantly higher in men than women. Park et al (30) concluded that early stage gastric carcinomas with high MSI were only associated with old age and female sex. Lu et al (13) found that BAT-26 is an independent indicator of MSI-high gastric cancers with distinct clinicopathological features. In this study, variant alleles were found in 3 male and 3 female cancer patients. This seems to suggest that there may be no difference in the frequency of variant alleles between male and female patients, but these findings should be confirmed by testing more samples, which will also help to further confirm the trend from QMVR to polymorphic in cancer patients because the variant alleles are very low in number.
Footnotes
Abbreviations
Financial support: This work was supported by Project Funded by the Priority Academic Program Development of Jiangsu Higher Education Institution (PAPD, 012062003010).
Conflict of interest: The authors declare they have no conflict of interest.