
Abstract
Background
Given the major role of obesity and insulin resistance (IR) in colorectal cancer (CRC), we investigated whether genetic variants in ghrelin (GHRL), resistin (RETN) and insulin receptor substrate 1 (IRS1) were associated with CRC risk.
Methods
This study was conducted as a case-control study, and 750 subjects, including 438 controls and 312 patients with CRC, were enrolled and genotyped using the PCR-RFLP method.
Results
No significant differences were observed for GHRL (rs696217), RETN (rs3745367) and IRS1 (rs1801278, Gly972Arg or G972R) gene variants between the cases and controls. However, the IRS1 G972R R allele compared with the G allele and the G972R RR+GR genotype compared with the GG genotype appeared to be markers of decreased CRC susceptibility in the overweight/obese subjects (p = 0.024; odds ratio [OR] = 0.42, 95% confidence interval [95% CI], 0.20-0.91; and p = 0.048; OR = 0.42, 95% CI, 0.17-0.99, respectively). Furthermore, the R allele and RR+GR genotype were also associated with decreased risks for obesity in the patients with CRC (p = 0.007; OR = 0.35, 95% CI, 0.15-0.77; and p = 0.015; OR = 0.35, 95% CI, 0.15-0.72, respectively).
Conclusions
In accordance with previous studies, our findings suggest that the IRS1 G972R R allele and RR+GR genotype have protective effects for CRC in overweight/obese patients and for obesity in patients with CRC. Nevertheless, further studies are required to confirm these findings.
Introduction
Colorectal cancer (CRC), one of the leading causes of tumor-related death, is the second most commonly diagnosed cancer around the world (1). It has been shown that obesity, hyperinsulinemia and insulin resistance (IR) are involved in the etiology of CRC, and hyperinsulinemia has been proposed as a putative mechanism that links obesity with CRC (2-3-4-5-6). Previous epidemiological studies have also reported that individuals with type 2 diabetes mellitus, which is associated with IR and obesity, are at increased risk of CRC (7). Furthermore, there are negative associations between serum levels of ghrelin (product of the GHRL gene) and both obesity (8) and CRC (9), and positive associations between serum levels of resistin (product of the RETN gene) and both obesity (10) and CRC (11). Ghrelin and resistin are involved in body weight regulation. Ghrelin is a key regulator of food intake and energy balance (12) and plays a role in cell proliferation and apoptosis (13). Resistin also plays a pivotal role in energy balance and carcinogenesis (14). In addition, insulin receptor substrate 1 (product of the IRS1 gene) plays a key role in insulin action and cell proliferation (15). Insulin enhances proliferation and inhibits apoptosis in the target tissues (4, 7), and its serum level is positively associated with CRC (5). Finally, despite the biological plausibility, previous reports have been inconsistent about the association between GHRL (16, 17), RETN (17-18-19) and IRS1 (20-21-22-23) gene variants and CRC risk, and the roles of these 3 genes in the etiology of CRC are still equivocal.
Therefore, this study was designed to investigate the possible associations of GHRL (rs696217), RETN (rs3745367) and IRS1 (rs1801278) gene variants with CRC risk. These single nucleotide polymorphisms (SNPs) were chosen based on their common use in previous genetic epidemiology studies, degree of heterozygosity and functional importance.
Methods
Participants
A hospital-based case-control study with 438 controls (age range 17-88 years) and 312 patients with CRC (age range 19-82 years) was performed between July 2007 and January 2013 in Tehran, Iran. Both cases and controls were recruited from individuals who were undergoing colonoscopy for various gastrointestinal complaints such as change of bowel habits, unexplained weight loss, long-term pain in the abdomen, rectal bleeding, chronic diarrhea or constipation. However, the case group consisted of all eligible colonoscopy patients with positive pathological report for CRC, while only subjects whose colonoscopic results were negative for malignancy, as well as for adenomatous polyps or other polyps, were chosen as controls. All subjects were Iranian and genetically unrelated, and they were informed about the aims of the study. Information on demographic, anthropometric and clinical characteristics of the cases and controls was recorded using a self-administered questionnaire before diagnosis of CRC. Study protocol was approved by the Ethical Review Boards of the Institution, and it was in accordance with the principles of the Helsinki Declaration. Body mass index (BMI) was calculated by weight in kilograms divided by height in meters squared, and a total of 750 subjects, including 438 controls and 312 patients, were divided into subgroups based on the diagnosis of CRC and BMI values as follows: normal weight (BMI <25) controls (n = 211), overweight/obese (BMI ≥25) controls (n = 227), normal weight cases (n = 139) and overweight/obese cases (n = 173).
Genotype Analysis
Genomic DNA was extracted from 5 mL EDTA-anticoagulated whole blood using standard methods, and genotyping was done by the polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) method. Furthermore, the genotyping process was performed by investigators who were blinded to the subjects’ clinical data. Details of the studied gene variants and PCR and RFLP conditions are shown in Table I. All of the PCR products were digested overnight by corresponding restriction enzymes (Fermentas, Leon-Rot, Germany) and then electrophoresed on 2% to 3.5% agarose gels. The PCR and RFLP bands in gels were stained with ethidium bromide for visualization under UV light. GHRL, RETN and IRS1 genotypes for each subject were identified according to the digestion pattern and the presence or absence of the BseNI, BtgI and MvaI sites, respectively. To check for genotyping error rate, we repeated the genotyping analysis for approximately 20% of randomly selected samples, and all the results were concordant.
Information for the studied markers in ghrelin (GHRL), resistin (RETN) and insulin receptor substrate 1 (IRS1) genes
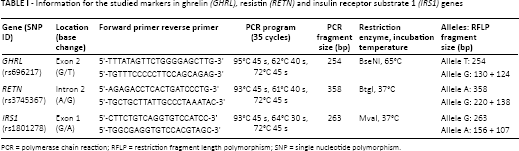
PCR = polymerase chain reaction; RFLP = restriction fragment length polymorphism; SNP = single nucleotide polymorphism.
Statistical Methods
We calculated differences in demographic or anthropometric factors using t-test or chi-square (χ2) test when appropriate. Consistency of genotype frequencies with the Hardy-Weinberg equilibrium (HWE) for each SNP among cases and controls was tested using the chi-square test. The chi-square test was also used to calculate the differences in the allele frequencies between the groups. Logistic regression was used to compare the distribution of the genotype frequencies between the different groups. To adjust confounding factors, including age, BMI, sex, smoking statues and family history of CRC, logistic regression analysis was also used. The odds ratios (ORs) were the measure of associations, and for all ORs, 95% confidence intervals (95% CI) were calculated. For statistical analyses, we used SPSS software, version 15.0 (SPSS Inc., Chicago, IL, USA). Significance was assumed for a p value of <0.05.
Results
Table II summarizes the major parameters of the patients with CRC and controls. There were no statistically significant differences between the 2 groups regarding their BMI, sex, smoking status and family history of CRC. However, the patients were older compared with controls.
Characteristics of patients with colorectal cancer and controls *
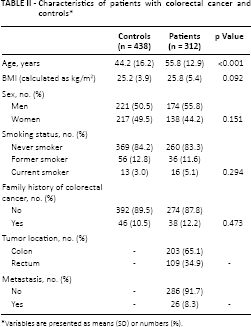
Variables are presented as means (SD) or numbers (%).
Table III shows the genotype and allele distributions for GHRL (rs696217), RETN (rs3745367) and IRS1 (rs1801278) gene variants in the patients with CRC and controls. No significant deviations from HWE were found for RETN and IRS1 genes in either patients or controls, suggesting that the alleles were in equilibrium (p>0.05). However, the genotype frequencies of the GHRL gene rs696217 variant were consist with HWE among the controls, but were out of HWE in the patients (p<0.05). We also observed no significant difference in genotype or allele frequencies between the patients and controls for all 3 genes either before or after adjustment for confounding factors including age, BMI, sex, smoking status and family history of CRC (Tab. III). However, the IRS1 rs1801278 A or G972R R allele compared with the rs1801278 G or G972R G allele and the rs1801278 AA+GA or G972R RR+GR genotype compared with the rs1801278 GG or G972R GG genotype appeared to be markers of decreased CRC susceptibility in the overweight/obese patients (p = 0.024; OR = 0.42, 95% CI, 0.20-0.91; and p = 0.048; OR = 0.42, 95% CI, 0.17-0.99, respectively).
Distribution of the genotypes and alleles of ghrelin (GHRL), resistin (RETN), and insulin receptor substrate 1 (IRS1) gene variants among colorectal cancer patients and controls
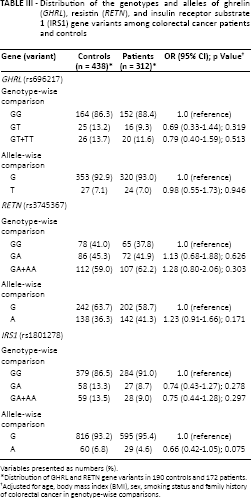
Variables presented as numbers (%).
Distribution of GHRL and RETN gene variants in 190 controls and 172 patients.
Adjusted for age, body mass index (BMI), sex, smoking status and family history of colorectal cancer in genotype-wise comparisons.
The possible role of the GHRL (rs696217), RETN (rs3745367) and IRS1 (rs1801278) gene variants in obesity was also examined in the present study. No significant difference in genotype and allele frequencies between the normal weight and overweight/obese patients with CRC, and between normal weight and overweight/obese controls for GHRL (rs696217) and RETN (rs3745367) gene variants was observed. However, the IRS1 G972R R allele and RR+GR genotype were associated with decreased risks for obesity in the patients (p = 0.007; OR = 0.35, 95% CI, 0.15-0.77; and p = 0.015; OR = 0.35, 95% CI, 0.15-0.72, respectively).
Discussion
Given the important role of obesity and IR in the pathogenesis of CRC, our case-control study was design to investigate whether there was an association between GHRL, RETN and IRS1 gene variants and susceptibility to CRC risk in an Iranian population. The results of our study indicated no significant differences in allele or genotype frequencies of GHRL, RETN and IRS1 gene variants between the patients with CRC and controls. However, when the subjects were subdivided by BMI, the IRS1 G972R R allele compared with the G allele and the RR+GR genotype compared with the GG genotype had protective effects for CRC in the overweight/obese subjects. Furthermore, the R allele and RR+GR genotype were also associated with decreased risks for obesity in patients with CRC.
To identify most of the genes involved in complex multifactorial diseases such as cancer may be difficult due to their relatively small individual effects and complex interactions (24). Previous studies, however, have suggested that the genes involved in obesity and IR are potential candidate genes for CRC because as mentioned before, CRC patients have an increased risk of obesity and IR. Recent studies have suggested that ghrelin and resistin may be involved in cancer development. The association between GHRL and RETN gene variants and CRC risk has been examined in several epidemiological studies, and the results were conflicting (16-17-18-19). Our findings are in line with those studies that showed no associations between CRC risk and GHRL (16, 17) and RETN (18, 19) gene variants. By contrast, significant associations have also been reported between GHRL (16) and RETN (17) gene variants and CRC risk. In this study, we found no significant association between the Leu72Met (rs696217) missense polymorphism of GHRL gene and CRC risk, which is in accordance with the study by Campa et al (16); nevertheless, Campa et al (16) also reported significant associations between other variants of GHRL gene (rs27647 and rs35683) and CRC risk. The RETN rs3745367 variant was the other gene polymorphism studied here. The rs3745367 is located in intron 2, and alterations in intronic sequences may influence protein expression and RNA splicing. Despite the biological plausibility, however, there are inconsistent results about the association between RETN gene variants and CRC risk, even between our previous study and the present study. Interestingly, in our previous study, the CC genotype of the RETN -420C>G (rs1862513) gene variant was a marker of decreased CRC susceptibility; while in this study, no significant association between the other variant (rs3745367) of the RETN gene and CRC risk was found. Unfortunately, there is no simple explanation for these discrepancies, which are common in genetic association studies (25). Conflicting results observed in the associations between GHRL and RETN gene variants and CRC risk may be attributable to differences in genotyped markers, statistical methods, disease definition, environmental factors, ethnic/racial differences in genetic makeup, small sample size and false positive results. Furthermore, the GHRL rs696217 and RETN rs3745367 variants may be in linkage disequilibrium with other unknown functional variants of the respective genes, which would explain the discrepancies observed.
Studies of the effects of the G972R variant, a glycine-to-arginine substitution at codon 972 in the IRS1 gene, on CRC risk have been inconclusive (20-21-22-23). This polymorphism has been used in many previous studies. Interestingly, in accordance with previous studies (20, 22), our findings suggest that the IRS1 G972R variant may be a genetic contributor to CRC risk; nevertheless, null associations have also been observed (21, 23). In our study, however, the IRS1 G972R R allele compared with the G allele and the RR+GR genotype compared with the ‘GG’ genotype appear to be markers of decreased CRC susceptibility in overweight/obese subjects. In other words, the R allele and RR+GR genotype have protective effects for CRC in overweight/obese subjects.
We also observed that the IRS1 G972R variant was associated with obesity, which is in line with previous studies (26-27-28). The IRS1 G972R R allele and RR+GR genotype were associated with a 65% decreased risk for obesity in the patients with CRC. The molecular mechanism through which the IRS1 G972R variant influences the risk of CRC and obesity remains speculative. However, previous studies have shown significant associations between the G972R variant and insulin secretion (29), IR (26), ovarian cancer (30), breast cancer (30) and prostate cancer (31). It has also been reported that obesity is involved in the etiology of CRC, and hyperinsulinemia has been proposed as a putative mechanism that links obesity with CRC (2-3-4-5-6). In fact, obesity can promote cancer through both IR and inflammation (32). Furthermore, the G972R variant is associated with obesity as well as IR in obese subjects, and there is a possible interaction between the gene variant and obesity to worsen insulin sensitivity (26-27-28).
Finally, the G972R variant may cause a change in the tertiary structure of the IRS1 protein and change the the function of the protein. In fact, the IRS1 G972R R allele compared with the wild-type allele (G) increases apoptosis and decreases proliferation (33, 34). Accordingly, our finding that the IRS1 G972R R allele appears to be a marker of decreased CRC susceptibility is consistent with the notions above. And a possible hypothesis is that the R allele is less stable and reduces IRS1 function (33) and may contribute to the decrease of CRC risk. Such a mechanism is speculative at present, but biologically plausible.
A number of limitations of the present study should be noted. First, the sample size of our study was relatively small, and the genotype differences may be attributable strictly to chance. Second, by testing only one variant in each gene, the coverage of the genes was incomplete. Third, our lack of information on serum levels of glucose, insulin, ghrelin and resistin as well as insulin resistance index (HOMA-IR) could have modified the effects observed here. Lastly, our study was a hospital-based study, and thus selection bias may have existed. However, the genotype frequencies of all 3 gene variants were consist with the HWE among the control group, and the controls came from the same region as the patients with CRC and were randomly sampled, which may reduce the effect of selection bias. Furthermore, our findings are in line with previous studies.
Nevertheless, in spite of these limitations, our study protocol was well designed and provides interesting information, and the possibility of true findings should not be excluded.
In summary, in accordance with previous studies, our findings indicated that the IRS1 G972R R allele and RR+GR genotype have protective effects for CRC in overweight/obese patients and for obesity in patients with CRC. Furthermore, the results of our study indicated no significant differences in allele or genotype frequencies of GHRL rs696217 and RETN rs3745367 gene variants between the patients with CRC and controls in the Iranian population. Nevertheless, further studies in other populations with increased numbers of CRC patients and controls are needed to validate our findings.
Footnotes
Financial support: This work was supported by a grant from the Gastroenterology and Liver Diseases Research Center, Shahid Beheshti University of Medical Sciences (Tehran).
Conflict of interest: The authors have no conflicts of interest with respect to this work.