
Abstract
Background
Salivary and serum levels of interleukin-6 (IL-6) and interleukin-8 (IL-8) have previously been studied in oral cancer with conflicting results.
Methods
We designed a controlled study to assess the correlation between pretreatment salivary and serum levels of IL-6 and IL-8, and all-cause survival and cancer recurrence in oral cancer patients.
Results
Fifty-two oral cancer patients and 52 healthy control cases were selected. In univariate analysis, salivary IL-6 and IL-8 seemed to be more expressed in cases (p<0.001 and p = 0.010, respectively). Multivariate analysis showed that higher pretreatment saliva IL-6 levels were significantly associated with better survival (hazard ratio [HR] = 8.62; 95% confidence interval [95% CI], 1.21-62.50; p = 0.031).
Conclusions
To date, this is the largest prospective controlled study that has analyzed the pretreatment salivary and serum levels of IL-6 and IL-8 in oral cancer patients, suggesting salivary IL-6 as a possible prognostic biomarker. But further validation in a larger sample is still necessary.
Introduction
Oral squamous cell carcinoma (OSCC) is the most frequent oral cancer, accounting for more than 90% of cases worldwide. Despite substantial improvements in diagnosis and therapy, OSCC still has a low estimated 5-year overall survival rate: 50% even in the United States and Western Europe (1, 2). Knowledge of specific prognostic and predictive factors could therefore be crucial in determining appropriate therapy.
Many different biological and molecular factors have been proposed as prognostic factors in OSCC, but they are far removed from having a real impact on routine clinical care (3). Cytokines play an important role in the initiation and maintenance of inflammatory and immune responses as well as intercellular cross-talking (4). Interleukin-6 (IL-6) is a multifunctional cytokine synthesized in response to defined stimuli by a variety of different cells (5). Interleukin-8 (IL-8) belongs to a super family of chemokines that has chemotactic activity for neutrophils, eosinophils, basophils, monocytes, mast cells, dendritic cells, natural killer (NK) cells and lymphocytes (6). Salivary and serum levels of IL-6 and IL-8 have been studied in head and neck cancer but with conflicting results, inadequate follow-up and in different types of tumors (7–10).
Therefore, we designed a study to assess the correlation between pretreatment salivary and serum levels of IL-6 and IL-8, and all-cause survival and cancer recurrence in OSCC patients.
Methods
This was a prospective cohort study: the primary explanatory variable was pretreatment salivary and serum IL-6 and IL-8 levels; control variables were age, sex, smoking, tumor site and stage, and different treatment modalities. The secondary outcome variables were tumor recurrence and all-cause survival.
Patient Selection and Control Variables
Consecutive white patients, attending the Oral Medicine Section of the Department of Surgical Sciences, University of Turin, between January and September 2008, were enrolled. Local ethical committee approval was obtained before the trial started, and all participants gave their written informed consent. Newly diagnosed patients with biopsy-proven OSCC were approached for participation in this study.
Excluded were those who (i) were age <18 years, (ii) were pregnant or breastfeeding, (iii) had mental health issues, (iv) had had a diagnosis of oral lichen planus, (v) or had had a clinical diagnosis of periodontitis. A group of control subjects, unrelated to the cases, were recruited from the population attending the University Hospital of Turin. All controls presented with no oral lesions.
Demographic information, smoking, alcohol consumption, tumor site, T classification and neck nodes involvement, treatment, outcome and survival rate (at 31 December 2012) were recorded. Tumor grade (well, moderately or poorly differentiated) (11), was evaluated by 2 different pathologists. C-reactive protein was also assessed.
Saliva and Serum Collection
Participants were asked to refrain from eating, drinking or oral hygiene for at least 1 hour prior to unstimulated whole saliva collection; they rinsed out their mouths with tap water and then waited at least 5 minutes before expectorating into a 50-mL Falcon tube. The tube was centrifuged at 3,500 rpm (2,600 g) for 15 minutes at 4°C (Hermle bench centrifuge Z300; Labnet International, Woodbridge, NJ, USA). The supernatant obtained was immediately transferred to a new tube and frozen at −80°C. Serum samples were collected at the same time, by centrifuging whole venous blood at 3,000 rpm (1,000 g) for 10 minutes at 15°C (Hermle bench centrifuge Z300; Labnet International, Woodbridge, NJ, USA). The aliquots were stored at -80°C.
Interleukins
Samples were tested using ELISA kits for recombinant human IL-6 and IL-8 (ThermoScientific/Pierce Biothechnology, Rockford, IL, USA). Cytokine protein levels were determined by solid phase quantitative sandwich immunoassay technique. The minimum detectable doses were 1.0 pg/mL for IL-6 and 2.0 pg/mL for IL-8. All testing was performed in duplicate per manufacturer instructions, and means were used for data reporting.
Statistical Analysis
A study with 52 case patients and 52 control subjects was planned in order to detect at least a true difference in the mean response of experimental and control subjects of ±0.52 standard deviation with an 80% power. The Type I error probability associated with this test of the null hypothesis that the population means of the experimental and control groups are equal is 0.05. If we suppose a Bonferroni setting, the detection of true difference in the mean response is ±1.71 standard deviations.
Means and frequency distributions were examined for all variables. Describing general information, data were reported as means and standard deviation (±SD). Associations between salivary and serum interleukins and control variables were assessed using analysis of variance. For univariate and multivariate analyses, interleukins were treated as a continuous variable after log transformation [ln(IL + 2)]. Univariate and multivariate Cox proportional hazards models were used to study the relation between salivary and serum IL-6 and IL-8, control variables and time to recurrence and death. Time to recurrence and death was measured from the pretreatment blood draw date. Crude and adjusted odds ratios (ORs) were computed using logistic regression analyses to assess the independent effects of control and pretreatment case variables. Statistical analyses were performed using the IBM-SPSS statistics software version 20.
Results
Cases and controls were comparable with regards to age, sex and risk factors. Fifty-two patients with OSCC were selected, of whom 32 were male and 20 female (mean age 66.19 ± 14.97 years). The follow-up period ranged from 12 to 60 months (median 39.4 months). During the period considered, 10 patients (19.2%) died because of the original OSCC. There was no recurrence in 29 patients(55.8%), while 13 (25%) developed a recurrence. No second primary tumors were detected.
Control Variables and Association with Pretreatment Levels of Interleukins
Table I shows the differences between cases and controls for interleukin expression. In univariate analysis, salivary IL-6 and IL-8 seemed to be more expressed in cases (p<0.001 and p = 0.010, respectively) than in controls; similar results were also present in the multivariate analysis, also adding a statistically significant higher expression of serum IL-8 (p = 0.006) for pretreatment cases.
Univariate and multivariate analyses of control and pretreatment case variables
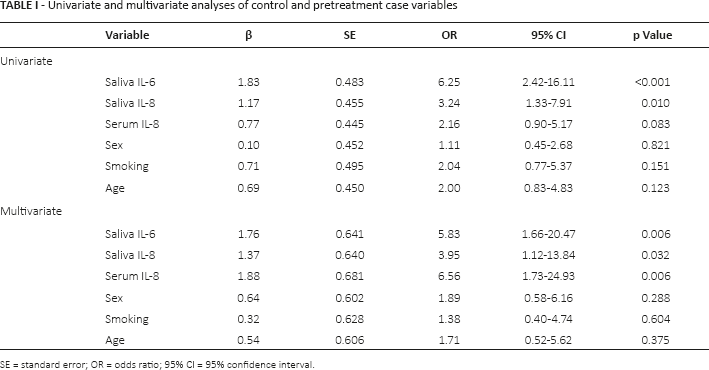
SE = standard error; OR = odds ratio; 95% CI = 95% confidence interval.
Older persons had higher salivary and serum IL-6 levels than did younger persons, which was the converse of salivary and serum IL-8 expression, but neither data had statistical significance. Smokers were more likely to have higher salivary IL-6 levels than nonsmokers. Those with larger cancers had higher levels of salivary IL-6 (p = 0.011). There was no association between salivary and serum interleukins and sex, cancer site, node association, serological inflammation data grading or treatment type; there was only a larger expression of salivary IL-6 and salivary IL-8 and lymph node involvement, but again without statistical significance.
IL-6, IL-8 and Control Variables as Independent Predictors of Recurrence and Survival
The results of the univariate and multivariate Cox proportional hazards regression models for recurrence and survival are detailed in Table II. Serum IL-6 was not included in the final model, because the levels were too low to perform the analysis.
Univariate and multivariate ratios of IL-6 and IL-8 from cox proportional hazard regression models for recurrence and death events
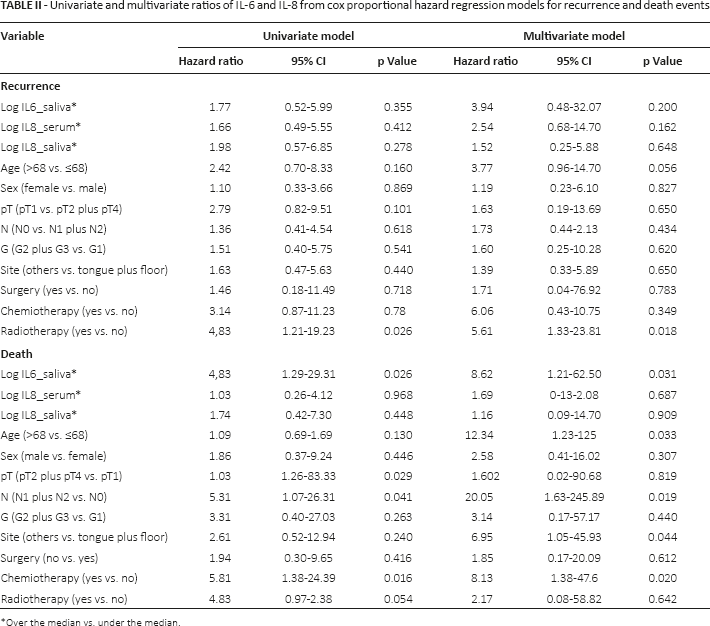
Over the median vs. under the median.
Univariate and multivariate analyses did not show that higher pretreatment salivary or serum levels of interleukins were associated with recurrence. Analyses showed that patients who underwent radiotherapy remained significantly more susceptible to recurrence, even after controlling for the other variables.
Univariate analysis showed that larger cancers, nodal involvement and chemotherapy were significantly negatively associated with survival. Both analyses showed that higher pretreatment saliva IL-6 levels were significantly associated with survival (p<0.05). Older age, nodal involvement, cancer site and having chemotherapy were also independently associated with poorer survival in the multivariate analysis, whereas sex of participant was not associated with survival.
Discussion
OSCC is one of the most complex malignancies to control, and only a small improvement has been seen in the survival rate over the last decades. The problems of metastasis, recurrences and difficulties in reconstruction comprise the main obstacles in treatment; therefore, early detection would be a powerful assistance in improving quality of life and outcomes and survival rates (12).
The use of saliva as a diagnostic biofluid has long been recognized, and it has many advantages over other specimens such as blood, exfoliated cells and urine (13). To date, some studies based on salivary and serum cytokine expression profiles have endeavored to provide information relevant to survival rate and recurrence of OSCC, but several critical issues still need to be addressed before these findings can be fully utilized in patient care. One of the biggest problems is that samples have included not only oral cancer but also oropharyngeal carcinomas, which generally have a different etiopathogenesis (human papillomavirus) and a better prognosis.
In the present study, we set out to identify whether IL-6 and IL-8 could potentially be useful as biomarkers for oral cancers. Interleukin 6 was detected at higher concentrations in the saliva of OSCC cases compared with controls, and IL-8 was detected at higher concentrations both in the saliva and in the serum of patients with OSCC. Moreover, salivary IL-6 levels have been demonstrated to be useful also as independent prognostic factors for OSCC survival rate.
Data confirmed the hypothesis that saliva should be preferred to blood in this type of research, its collection having the potential to serve as noninvasive, widely accessible screening tools that do not rely on the localization of a lesion for diagnosis. Collection is also inexpensive and can be performed in any setting. If it became routine, saliva as a diagnostic tool for OSCC would also be a suitable instrument for population screening, monitoring of patients at high risk of recurrences, and subsequently for improving survival rates (12).
Serum measurements of cytokines may reflect the systemic response to tumor development and progression, and may not be simply indicative of local biochemical events at the tumor site. Moreover, several studies have outlined the importance of autocrine IL-6 signaling in different types of carcinoma, such as lung, breast, skin, and in head and neck squamous cell carcinoma cell lines, where findings indicate that endogenous IL-6 could play an important role in the growth of tumor and exert its action by an autocrine growth mechanism. Therefore, it seems that variations of salivary levels of IL-6 and IL-8 could represent disease markers that could possibly reflect accurately tumor status (13–15).
Higher levels of the salivary cytokines (above all IL-6) may have significant usefulness as surrogate biomarkers to improve the efficiency of chemoprevention therapy (7). Although, the present data were from a relatively small sample size (even if the biggest in oral cancer ever reported), the results were significant enough to merit further investigation.
Determination of the exact mechanisms leading to increased IL-6 and IL-8 secretion in recurrent and advanced disease might also lead to new therapeutic interventions or approaches to monitoring.
To the best of our knowledge, this is the largest prospective control study that analyzed the pretreatment salivary and serum levels of IL-6 and IL-8 in OSCC patients, confirming earlier results (16), which have suggested salivary IL-6 and IL-8 as diagnostic biomarkers for OSCC, but further validation in a larger sample in a multicenter population study is still necessary.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: The authors declare that they have no conflict of interest.