
Abstract
Objective
The aim of this study was to estimate the diagnostic accuracy of serum marker CA 19-9 levels in the triage of adnexal masses.
Methods
This retrospective cohort study was carried out in patients referred to the Gynecology Department at Carmel Medical Center due to adnexal masses. All patients underwent preoperative measurements of serum CA 125 and CA 19-9 and surgery with histopathologically confirmed diagnosis.
Results
Between January 2005 and December 2012, 503 patients with adnexal masses were evaluated with serum tumor markers. Combination of CA 19-9 with CA 125, compared with CA 125 levels alone, suggested a nonsignificant effect on sensitivity (86.9% vs. 88.9%, respectively, p = 0.54) or specificity (79.5% vs. 73.5%, p = 0.1) in differentiating malignant from benign adnexal masses. CA 19-9 was not helpful in detecting mucinous histological types or borderline tumors. Mean CA 19-9 levels were higher in metastatic cases compared with primary ovarian malignancy (488.7 ± 1,457 vs. 46.3 ± 149.8 U/mL, respectively, p = 0.001). In mature cystic teratomas, mean CA 19-9 levels were higher and CA 125 levels were lower than in ovarian carcinoma (p = 0.049 and p = 0.0012, respectively).
Conclusions
The combination of the tumor markers CA 19-9 and CA 125 did not contribute significantly to the detection of malignant adnexal masses compared with CA 125 alone. As our results suggest that higher CA 19-9 levels could be helpful in differentiating metastatic tumors from primary ovarian malignancy; this issue should be investigated in large well-designed prospective cohort trials.
Introduction
Adnexal mass is a common gynecological finding, demonstrated in up to 7.8% of premenopausal and 2.5% of postmenopausal women (1, 2), and there is a 5% 10% lifetime risk for women to undergo surgical evaluation for an adnexal mass (3). The main concern of the managing physician is to exclude malignancy. Definitive diagnosis of ovarian cancer requires a histological sample, which is usually obtained by an invasive procedure. However, this approach often results in performance of surgical procedures in women with benign masses. While in postmenopausal women, 30% of complex adnexal masses are malignant (3), in premenopausal women, ovarian cancer is rare. Thus, accurate preoperative assessment of adnexal masses is important for patient counseling, choosing the optimal surgical procedure and avoiding unnecessary invasive procedure.
At present, combination characteristics are used to assess the risk of malignancy in patients presenting with adnexal masses. These include patient's age, menopausal status, gynecological examination, imaging modalities (mainly ultrasonography) and tumor markers. Tumor marker CA 125, a high-molecular-weight mucin protein (MUC16) that is recognized by the OC125 monoclonal antibody, has been the focus of most investigations and is the most extensively used, alone and in combination with other markers. Initial studies showed that serum levels of this antigen were elevated in approximately 80% of women with epithelial ovarian cancer (4). However, subsequent research has demonstrated both lower sensitivity and lower specificity for early-stage cancer detection (5, 6). A meta-analysis of 49 cohort studies and 2 case-control studies found that, at a threshold of 35 U/mL, CA 125 measurements had an overall sensitivity of 78.7% and a specificity of 77.9% (7). Elevated serum CA 125 levels are also associated with a variety of common benign gynecological conditions, including uterine leiomyomas, pelvic inflammatory disease, endometriosis, pregnancy and even menstruation and ovulation, which explains the low specificity, especially in premenopausal women.
Given the suboptimal accuracy of CA 125 alone in evaluation of adnexal mass, other serum tumor markers have been suggested alone and in combination with CA 125 by different investigators (8). Combining CA 125 with other markers has been shown to increase sensitivity by 5%-10%; however, specificity was reduced (8).
CA 19-9 is a monosialoganglioside, with an assay that was been demonstrated to yield high specificity and sensitivity for diagnosis of gastrointestinal adenocarcinomas, especially those of the pancreas (9). Since elevated levels of this biomarker have been reported in ovarian cancer patients, especially in mucinous histological types (10), measurement of CA 19-9 has been proposed to be of some clinical value in combination with CA 125 as a marker for serological monitoring of ovarian cancer (11). Accordingly, in some institutions, CA 19-9 has been incorporated as a tumor marker for evaluation of patients with adnexal masses. However, later studies have shown that CA 19-9 levels were not helpful in differentiating benign from malignant adnexal masses (12-14). Moreover, its levels were shown to be high in several benign ovarian findings, especially mature cystic teratomas (15) and endometriomas (16), and even in nongynecological conditions such as rheumatoid arthritis (17).
None of the national guidelines, including those of the American College of Obstetricians and Gynecologists (ACOG), the Society of Gynecologic Oncologists (SGO) and National Institute for Health and Clinical Excellence (NICE), have included CA 19-9 measurement as an adjunct in the triage of patients with adnexal masses (18, 19). Nevertheless, in many institutions, CA 19-9 is still sparingly used as a preoperative tumor marker in the investigation of a patient with an ovarian mass.
Thus, the objective of this study was to assess the added value of CA 19-9 measurement as a preoperative tumor marker in the evaluation of patients with ovarian masses.
Materials and Methods
Data from all cases referred to the Gynecology Department at Carmel Medical Center with a diagnosis of adnexal mass, between January 2005 and December 2012, were retrospectively obtained from the computerized database of the hospital charts and the pathological registry. All patients underwent a tertiary transvaginal or transabdominal sonography, and only cases with preoperative measurement of serum CA 125 and CA 19-9 levels (drawn as part of regular clinical practice) were included in the study. Oophorectomy, cystectomy or hysterectomy with unilateral or bilateral salpingo-oophorectomy were performed as treatment modality according to age and menopausal status, fertility considerations, physical examination and sonographic findings. Cases were excluded from the study if the final histological type of the adnexal finding was not documented. The reports were reviewed, and the retrieved parameters included patient's age and histological type. The latter was then divided into 6 categories: benign, borderline, primary ovarian malignancy, tumor metastatic to the ovary, granulosa or germ cell tumor.
All serum marker measurements were performed in the Clinical Biochemistry Laboratory of Carmel Medical Center, by electrochemiluminescence immunoassay on a Roche Cobas e analyzer (Roche Diagnostics, Mannheim, Germany). Serum CA 125 of <35 U/mL and CA 19-9 of <37 U/mL were taken as within the normal range. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), and odds ratio were calculated for each tumor marker and for their combination in evaluation of benign vs. malignant adnexal masses. A separate examination of CA 19-9 and CA 125 values was made in borderline tumors, mature cystic teratomas with or without malignant transformation, endometriomas and mucinous findings.
The study was approved by the local institutional review board committee for human subjects. Since data acquisition was performed retrospectively, informed consent from the patients whose samples were used in the study was not obtained.
Statistical Analysis
Data were analyzed using SPSS software (SPSS Inc., Chicago, IL, USA). Continuous variables were presented as means ± SD and were tested by Student's t-test. Categorical data were expressed as numbers and compared using Fisher's exact test and Z-test calculator for 2-population proportions, when appropriate. A p value <0.05 was considered statistically significant for all comparisons.
Results
Five hundred and three women aged 18-88 years, referred to our institution due to adnexal masses, were identified and included in the study. Benign pathology was diagnosed in 268 of the cases (53.3%), 182 of the histology reports (36.2%) were malignant and 17 (3.4%) metastatic, including 13 cases of gastrointestinal origin (none of which were of pancreatic source), 3 cases of metastatic breast carcinoma and 1 case of sarcoma of unknown origin. The remaining cases included 28 (5.6%) borderline tumors, 7 (1.4%) granulosa cell tumors and 1 case of germ cell tumor.
Mean preoperative serum CA 125 and CA 19-9 levels were 306.4 ± 869 U/mL and 55.5 ± 313.5 U/mL, respectively. CA 19-9 levels were elevated above 37 U/mL in 77 cases (15.3%). Using the Spearman rank correlation test, no correlation was found between the 2 markers (data not shown). Table I presents mean tumor marker levels by each pathology outcome.
CA 125 and CA 19-9 levels according to the pathology outcome
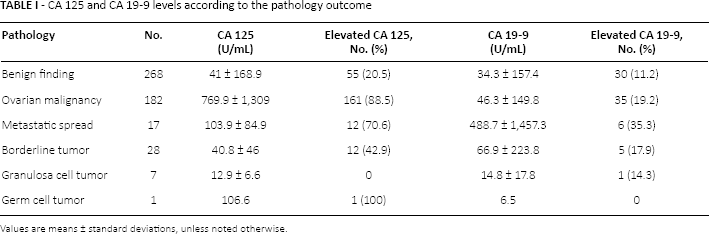
Values are means ± standard deviations, unless noted otherwise.
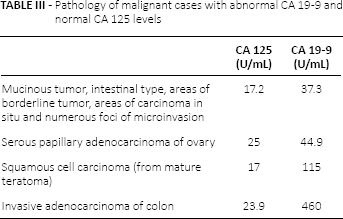
Since only 7 cases of granulosa cell tumor and 1 case of germ cell tumor were reported, these cases were omitted from the statistical analysis. In addition, the borderline tumor group was analyzed separately because of its unique nature. In the remaining 467 cases, 268 benign and 199 malignant (primary ovarian and metastatic) cases were demonstrated (Tab. II). Mean CA 125 levels in the malignant group were 730.3 ± 1282.8 U/mL, higher than in the benign group (p<0.0001), while mean CA 19-9 levels did not significantly differ between the malignant (84.4 ± 454.4 U/mL) and benign groups (p = 0.09). Combination of both markers did not exhibit any significant effect on malignancy diagnosis, compared with CA 125 alone. Of note, in the 239 cases with normal CA 125 level, which included 26 malignancies, elevated CA 19-9 was found in 20 cases. Of these, 16 cases were benign and 4 malignant (15.4% sensitivity and 20% PPV for malignancy), with varying pathology (Tab. III). Mean CA 19-9 levels did not differ significantly between the 26 malignant (33.97 ± 89.9 U/mL) and 213 benign (19.95 ± 54.2 U/mL) cases with normal CA 125 levels (p = 0.25).
Analysis of CA 125 and CA 19-9 levels in malignant vs. benign cases
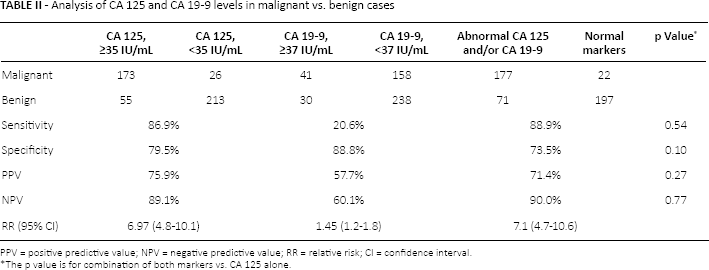
PPV = positive predictive value; NPV = negative predictive value; RR = relative risk; CI = confidence interval.
The p value is for combination of both markers vs. CA 125 alone.
Pathology of malignant cases with abnormal CA 19-9 and normal CA 125 levels
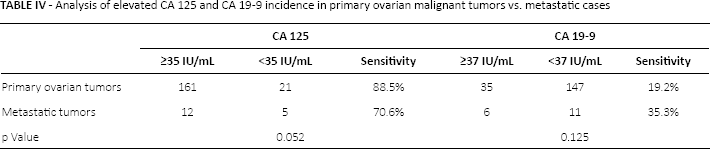
Out of 199 malignant cases, 182 primary ovarian malignant tumors were found and 17 cases of metastatic spread to the ovary (Tab. IV). Significantly higher mean CA 125 and lower mean CA 19-9 levels (Tab. I) were observed in primary ovarian malignant tumors compared with the metastatic group (p = 0.038 and p = 0.001, respectively).
Analysis of elevated CA 125 and CA 19-9 incidence in primary ovarian malignant tumors vs. metastatic cases
Combined analysis of the 28 borderline tumors with benign cases is presented in Table V. Mean CA 125 and CA 19-9 levels (Tab. I) did not differ between borderline and benign groups (p = 0.99 and p = 0.32, respectively). In the 16 serous and 12 mucinous borderline tumors, elevated CA 19-9 was observed in 3 serous and 2 mucinous histotypes (p = 0.64). No significant differences were found between mean CA 19-9 levels in serous (30.9 ± 60.6 U/mL) vs. mucinous (113.5 ± 337.5 U/mL) borderline tumors (p = 0.34).
Analysis of elevated CA 125 and CA 19-9 incidence in borderline tumors vs. benign cases
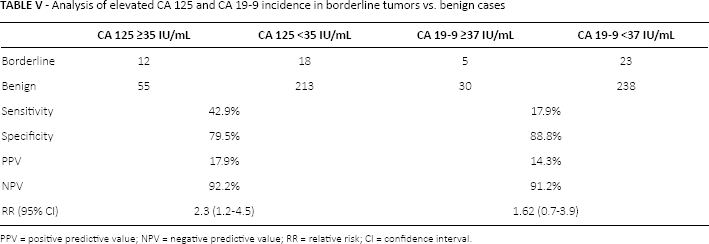
PPV = positive predictive value; NPV = negative predictive value; RR = relative risk; CI = confidence interval.
Fifty mucinous histotype cases were found overall, including 30 benign mucinous cystadenomas/cystadenofibromas, 12 borderline tumors, 5 cases of primary ovarian mucinous adenocarcinomas and 3 adenocarcinomas of colon. CA 19-9 was elevated in 10 of these cases (20%): 4 benign, 2 borderline tumors, 2 ovarian and 2 metastatic tumors. This proportion was not statistically significant compared with the rest of the cases. Mean CA 19-9 levels in the mucinous group (100.2 ± 273.9 U/mL) did not differ from the rest of the cases (p = 0.33). Also, CA 19-9 levels in the 8 mucinous malignant histotypes (373.26 ± 466.98 U/mL) were not significantly different from the rest of the malignant cases (p = 0.08).
Thirty-three cases of mature cystic teratomas (MCTs) were noted, 9 of which (27.3%) demonstrated elevated CA 19-9 levels – not significant compared with the study group (p = 0.055). Mean MCT CA 19-9 levels (127.8 ± 415.8 U/mL) did not differ from the rest of the study group (p = 0.21), but were significantly higher than in primary ovarian malignant tumors (p = 0.049). Mean CA 125 levels (19.7 ± 26.8 U/mL) in MCT cases were found to be significantly lower than in primary ovarian malignant tumors (p = 0.0012).
The pathological report noted 3 cases of malignant transformation of MCT, with mean CA 19-9 level of 93.3 ± 77.9 U/mL, which was not different from benign MCT CA 19-9 levels (p = 0.89).
In addition, CA 19-9 levels were high in 8 of 23 endometrioma cases (34.7%) – a statistically significant proportion compared with the rest of the cases (p = 0.013). However, mean CA 19-9 levels in this group (47.3 ± 54.5 U/mL) did not differ from the rest of the study group (p = 0.9), or from ovarian malignancy in particular (p = 0.97). Mean CA 125 levels (106.1 ± 124.2 U/mL) in endometriosis were found to be significantly lower than in primary ovarian malignant tumors (p = 0.0012), but higher than in MCTs (p = 0.003).
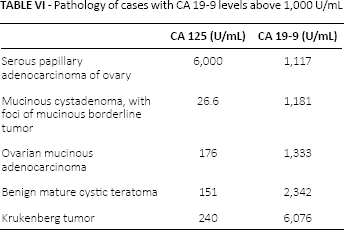
Finally, 5 cases of extremely high CA 19-9 levels (above 1,000 U/mL) were demonstrated (Tab. VI), with varying pathology. Four of these cases also exhibited increased CA 125 levels, except 1 case of borderline mucinous tumor.
Pathology of cases with CA 19-9 levels above 1,000 U/mL
Discussion and Review of the Literature
CA 19-9 and Malignancy
CA 19-9, a monoclonal antibody reacting with sialylated lacto-N-fucopentaose 11 (20), was originally raised against a human colon carcinoma cell line SW 116 (21). Initial studies showed that at serum concentrations above 37 U/mL, CA 19-9 levels had high specificity (98.5%) and high sensitivity (up to 79%) for patients with gastrointestinal adenocarcinomas, especially those originating from the pancreas (9). When examined immunohistochemically, CA 19-9 has been shown to occur in association with ovarian adenocarcinomas, with mucinous histological types reacting much more frequently than serous (22). In 1983, elevated CA 19-9 was demonstrated in the serum of ovarian cancer patients, and thus was proposed to be of some clinical value in combination with CA 125 as a marker for serological monitoring of ovarian cancer (11). Previous reports have found elevated CA 19-9 levels in 41.7%-48.8% of ovarian cancer patients (10, 23). Gadducci et al evaluated 90 patients with epithelial ovarian cancer and 254 patients with benign ovarian pathology, and showed that combination of serum CA 125 and CA 19-9 had a significantly higher sensitivity (93.2% vs. 81.1%; p = 0.03) and a slightly lowered specificity (78.9% vs. 86.0%; p = 0.46) than CA 125 assay alone in the differential diagnosis of ovarian masses in patients above 50 years of age (24). However, more recent studies have shown that CA 19-9 levels were not statistically significant in the differentiation of benign and malignant of adnexal masses (12-14). A study that evaluated preoperative CA 19-9 in 186 patients who were subsequently surgically treated for adnexal masses, demonstrated sensitivity of 18.4% and specificity of 93% (14). Similar estimations were suggested in our study (sensitivity of 20.6% and specificity of 88.8%).
The usefulness of CA 125 for predicting malignancy of adnexal mass in our study (sensitivity of 86.9%, specificity of 79.5%, PPV of 75.9% and NPV of 89.1%) also approximated the findings reported by other larger studies. Combination of both markers did not exhibit a significant effect on the performance of CA 125 alone. Therefore, in our opinion, and consistent with several previous studies, preoperative CA 19-9 levels have no meaningful value in predicting whether a suspected adnexal finding is benign or malignant.
CA 19-9 and metastases
An interesting finding demonstrated in our analysis was significantly higher mean CA 19-9 levels in metastatic cases compared with the primary ovarian malignancy group. While a few studies have noted increased CA 19-9 levels in nongynecological malignancies metastasizing to the ovaries (25, 26), surprisingly very scarce data are to be found in the professional literature regarding the ability of serum CA 19-9 levels to differentiate between primary and metastatic ovarian tumors. Several studies, using immunohistochemistry, showed that CA 19-9 is not a useful discriminatory parameter in differentiating between primary and metastatic ovarian carcinomas (22, 27, 28). As our results suggest that CA 19-9 serum levels can be helpful in differentiating metastatic from primary ovarian malignancy, this matter should be investigated in larger, prospective studies.
CA 19-9 and borderline ovarian tumors
Borderline ovarian tumors (BOTs) account for 10%-20% of ovarian epithelial tumors (29). BOTs differ from benign findings by an increased mitotic index and the presence of nuclear atypia, but unlike malignant forms, BOTs lack stromal invasion (30). These tumors have a favorable prognosis, with a 10-year survival rate higher than 95% (31). Limited studies have evaluated CA 19-9 levels in BOTs. In 1996, a retrospective study of 101 BOT patients suggested that CA 19-9 has clinical value in screening for BOTs, since its levels were found to be positive in 51.5% of serous tumor cases and 44.7% of mucinous tumors (32). Additional studies reported on elevated CA 19-9 rates in 8%-27% of serous and 30.4%-65% of mucinous BOTs (33, 34). When retrospectively comparing 50 women a BOT and 50 individuals with benign adnexal mass, the sensitivity of CA 19-9 was shown to be 40%, specificity 66%, PPV 54%, NPV 52%, while the risk of malignancy index (35) was more accurate in discriminating between BOTs and benign adnexal masses (36).
Regarding tumor histology, it has been suggested that CA 19-9 levels are higher in mucinous tumors compared with serous (37, 38). In addition, it has been shown that endocervical-like mucinous BOTs exhibit higher CA 19-9 levels vs. intestinal-type tumors (39). In another 50 BOT patients, a significant relation was found between elevated CA 19-9 and cytology positivity, and in serous BOTs between abnormal CA 19-9 and recurrence (40). In addition, since abnormal levels of CA 19-9 were found more frequently in stages IB-IIIC than in stage IA, a prognostic role for this marker has been suggested (41). Finally, as the marker levels tended to normalize after surgical tumor excision, a role of CA 19-9 in the follow-up of patients with a borderline mucinous histology has been proposed (38).
In our study, low sensitivity and PPV of CA 19-9 were demonstrated in differentiating BOTs from benign adnexal masses (17.9% and 14.3%, respectively), with relatively high specificity and NPV (88.8% and 91.2%, respectively). Likewise, no significant differences were found between mean CA 125 and CA 19-9 levels in borderline and benign groups. Finally, CA 19-9 was not found useful in distinguishing between serous and mucinous borderline tumors.
CA 19-9 and mucinous histotypes
Several studies have demonstrated elevated serum CA 19-9 levels in epithelial neoplasms of mucinous type and in benign mucinous ovarian findings (42-44). However, in our study this marker was not found to be useful in distinguishing between mucinous and nonmucinous malignancies, or between overall mucinous histotypes and the rest of the cases. These findings are supported by other studies (13).
CA 19-9 and benign findings
Increased CA 19-9 levels may be misleading in the context of diagnostics. For example, a CA 19-9 level of 2,880 U/mL was reported in 60-year-old woman presenting with ascites, eventually diagnosed with benign ruptured ovarian cyst (45). Significant increases in serum CA 19-9 were reported following torsion of ovarian adenofibroma (46), in benign mucinous ovarian cystadenoma (3,170 U/mL) (44) and in a case of appendiceal mucocele mimicking an adnexal complex mass (47).
In our study we found 5 cases with CA 19-9 levels above 1,000 U/mL, including 1 MCT, 1 borderline tumor, 1 metastatic tumor and 2 ovarian adenocarcinoma cases – serous and mucinous. Highest values were demonstrated in Krukenberg tumor (6,076 U/mL), and in MCT (2,342 U/mL), implying that even extremely high CA 19-9 levels are not enough to rule out a benign diagnosis.
CA 19-9 and MCTs
MCTs are common benign neoplasms, accounting for 10%-20% of all ovarian tumors (48). CA 19-9 has been immunohistochemically demonstrated in the bronchial mucosa and glands of MCT, and was shown to be secreted into the cystic cavity of the lesion (49). Several studies have noted that serum CA 19-9 levels have the highest positivity rate in ovarian MCTs, compared with other tumor markers including CA 125, CA 15-3, carcinoembryogenic antigen, alpha-fetoprotein and sialyl Tn antigen (15, 50-52). Several studies found increased CA 19-9 levels in 37.4%-39.6% of MCT cases (15, 50, 51, 53), with up to 78% in 1 prospective trial (54). CA 19-9 levels showed significant correlations with tumor size (50-52, 55), presence of adhesions (55) or fat component (56) and were significantly higher in cases of bilaterally occurring MCTs (15, 52). A recent retrospective study of 322 women by Cho et al aimed to determine whether CA 19-9 is a useful marker in discrimination of MCT from ovarian carcinomas (56). They showed that the incidence of CA 19-9 elevation was not different between the 2 groups, but the mean value of CA 19-9 was higher in those with ovarian malignancy. Futagami et al examined whether CA 19-9 can predict malignant transformation in MCTs (57). This retrospective analysis of 2 cases of MCT with malignant transformation and 76 cases of benign MCT showed that CA 19-9 can be elevated in both malignant and benign cases, while serum squamous cell carcinoma level may serve as indicator of malignancy.
In our study we found increased levels of CA 19-9 in 27.3% of MCT cases, with mean levels not differing from the rest of the cases or from the 3 cases of MCTs with malignant transformation. When comparing marker measurements in MCTs vs. primary ovarian malignant cases, the former yielded significantly higher levels of CA 19-9 and lower levels of CA 125. Hence, as was already suggested in the study by Cho et al (56), when an adnexal mass is demonstrated by ultrasound, and serum CA 19-9 is elevated, lower CA 125 levels can support a diagnosis of an MCT.
CA 19-9 and endometriosis
Several cases of endometriosis with extremely elevated CA 19-9 levels were reported (up to 7,604 IU/mL) (34, 35). One study even proposed CA 19-9 as a useful marker for determining the severity of endometriosis (36). Comparing 101 women with endometriosis and 22 without endometriosis, this retrospective work showed that mean serum CA 19-9 levels in patients at all stages of endometriosis were significantly higher than those in patients without endometriosis – elevated in 38.9% of cases – and that serum CA 19-9 levels significantly correlated with the Revised American Fertility Society classification scores.
In the 23 cases of endometriomas found in our study, the incidence of elevated CA 19-9 was 34.7%, comparable with previous reports. This percentage was significantly higher compared with the rest of the cases (p = 0.013), but the mean levels of this marker did not differ either from the rest of the cases in general or from the primary ovarian tumor group in particular. The finding that CA 19-9 can be significantly elevated in benign ovarian findings, such as endometriomas and MCTs, further supports the fact that elevated CA 19-9 has limited value in pointing out malignant tumors.
In summary, the combination of CA 19-9 with CA 125 did not exhibit clinical significance in distinguishing between benign and malignant adnexal masses compared to CA 125 alone. Likewise, CA 19-9 measurement was not useful in distinguishing mucinous findings or borderline tumors, or in distinguishing between MCTs and teratomas with malignant transformation. As our results imply that CA 19-9 levels could be helpful in differentiating metastatic tumors from primary ovarian malignancy, this subject should be further investigated in large well-designed prospective cohort trials.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors have any conflicts of interest to declare.