
Abstract
Chromosomal translocation resulting in the fusion between the echinoderm microtubule-associated protein-like 4 (EML4) gene and the anaplastic lymphoma kinase (ALK) gene was recently identified as a novel genetic alteration in a subset of non-small cell lung cancer (NSCLC). EML4–ALK translocations are rare events associated with specific clinicopathological features, such as never or light smoking history, young age and adenocarcinoma with signet ring or acinar histology. Reports suggest ALK gene arrangements are mutually exclusive with EGFR and KRAS mutations. To the best of to our knowledge, this is the first case report of a patient with concurrent KRAS mutation and ALK translocation. This patient had an excellent response to crizotinib, suggesting that the ALK translocation was the oncogenic driver.
Introduction
Anaplastic lymphoma kinase (ALK) gene translocations have been described in a subgroup of 4%-6% non-small cell lung cancers (NSCLC) (1). The echinoderm microtubule-associated protein-like 4 (EML4)-ALK fusion oncogene arises from an inversion on the short arm of chromosome 2 that links exons 1-13 of EML4 to exons 20-29 of ALK, leading to a fusion protein with constitutive activation of the ALK intracellular kinase domain (2). EML4-ALK fusion genes possess a strong oncogenic activity both in vitro and in vivo, and 11 different ALK-fusion variants are presently known (3, 4). Other clinically relevant molecular alterations in NSCLC include epidermal growth factor receptor (EGFR) kinase domain and KRAS mutations. Previous reports have suggested that ALK rearrangement and KRAS and EGFR mutations were mutually exclusive (5–7), although there are some cases reported with EML4-ALK rearrangement and EGFR mutation (8). We report a case of a patient with a coexisting KRAS mutation and ALK translocation.
Case Report
A 55-year-old, nonsmoking woman presented with a history of lower extremity swelling after a airplane flight. A chest computed tomography (CT) scan to rule out a pulmonary embolism was negative; however, a 4.2-cm mass was found in the lower left lobe associated with a small left pleural effusion (Fig. 1A, B). On further workup, positron emission tomography (PET) and magnetic resonance imaging (MRI) of the brain did not show evidence of extrathoracic disease. Pleural fluid was drained and found to have a negative malignant cytology. The patient underwent a left thoracotomy, during which multiple pleural-based nodules were noted, involving the lower lobe, mediastinum, pericardium and posterior pleura. The planned definitive surgical procedure was suspended, and multiple biopsies were taken. Pathological examination was consistent with adenocarcinoma with mucinous and signet ring cell features. Immunohistochemistry showed neoplastic cells to be positive for CK7, TTF1, Napsin A, CA-125 and CA 19.9, while negative for CK20, CDX2 and the estrogen receptor.
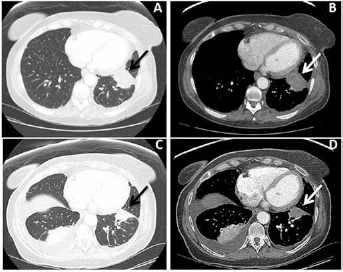
Computerized tomography scan of thorax before initiating crizotinib treatment (A, B) and with response to crizotinib (C, D). A, B) A 4.2-cm mass was found in the lower left lobe associated with a small left pleural effusion (arrows). C, D) Partial response without new lesions (arrows).
Fluorescence in-situ hybridization (FISH) assessment was performed and reported positive for ALK gene rearrangement and deletion of the 5 prime ALK gene as well as positive for subpopulations with extra copies of the ALK gene consistent with an aneuploid cell population (Fig. 2C). Mutation screening panel indicated that the tissue was also positive for a KRAS exon 4 A146V and an exon 2 E168D MET mutations (Fig. 2A, B).
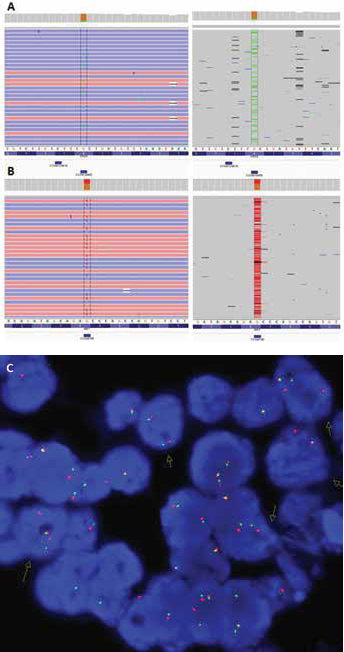
A) KRAS gene polymorphism in exon 4 (c.437 C>T pA146V) B) MET mutation in codon 168 in exon 2 leading to an amino acid change from glutamate to aspartate (c.504 G>T pE168D). C) Fluorescence in situ hybridization (FISH), positive result for presence of a clone with an ALK gene rearrangement, and deletion of the 5 prime ALK gene (arrows).
Based on molecular findings, treatment was initiated with crizotinib. After 2 months of therapy, the patient achieved a partial response (Fig. 1C, D). Tumor continued reducing in size for an additional 3 months, followed by 9 months of stable disease, after which crizotinib was discontinued due to tumor progression.
Discussion
Lung cancer in never-smokers (LCINS) is currently considered a distinct entity with its own unique epidemiological, clinicopathological and molecular features (9, 10). Mutations in EGFR, KRAS and ALK rearrangements are the 3 major oncogenic alterations associated with LCINS. Some studies suggest that ALK rearrangement and EGFR or KRAS mutations appear to be mutually exclusive (2, 6, 7).
EML4-ALK translocated NSCLCs share distinct clinical and pathological characteristics. They tend to occur in never-smokers and younger patients, with adenocarcinoma histology and advanced clinical stage (11, 12). Signet ring cells are more frequently found in gastrointestinal cancers and rarely seen in adenocarcinomas from other organs like lung. Adenocarcinomas with an ALK translocation are more likely to present signet ring cells than those with EGFR mutations (13).
KRAS mutations are present in approximately 20% to 30% of lung adenocarcinomas and are usually associated with smoking history (14). The presence of a KRAS mutation may confer a poorer prognosis (15), although this has not been uniformly observed in all studies (16). Recent studies suggest that KRAS mutations in LCINS are more likely to be transition mutations – different from those in smokers, which are most commonly transversion mutations (17).
This case presented with clinicopathological features characteristic of EML4-ALK rearranged NSCLCs, such as relatively young age, absence of smoking history, adenocarcinoma (signet ring cell) histology and advanced disease presentation. However, a KRAS mutation and a MET mutation were additionally noted. Although the A146V mutation in the exon 4 of the KRAS gene has been reported to confer resistance to EGFR tyrosine kinase inhibitors (EGFR TKIs), it also exhibits mitogen-activated protein/extracellular (MAPK) preference signaling and a more favorable clinical course than the common alterations at codons 12 and 13, explaining the excellent clinical response to crizotinib therapy in this patient (18).
The MET gene codifies for the hepatocyte growth factor receptor, a transmembrane tyrosine kinase receptor that, after autophosphorylation, initiates downstream signaling via the PI3K pathway (19). MET amplification has been associated with resistance to EGFR TKIs (20), but MET mutations are rare, and their oncogenic potential has not been determined. The E168D missense mutation is located in the ligand-binding (Sema) domain of c-MET. This mutation has previously been detected in some (21, 22) but not all (23) cohorts of small cell and non-small cell adenocarcinomas of the lung. Being a rare event, its functionality has not been determined. Nevertheless, homozygous deletions of 3p.21.3, where genes for Sema 3B and Sema 3F are located, have been implicated in small cell lung cancer progression (24–26), suggesting that the clinical implication of mutations in the Sema domain of c-Met, including the missense E168D, may worth determining.
This patient experienced an excellent disease control with crizotinib for 11 months, but ultimately progressed. In this scenario, different subsequent therapies could be implemented. First, ceritinib, a second-generation ALK inhibitor has been shown to induce response in ALK + NSCLC patients previously treated with crizotinib (27). Second, as the KRAS A146V variant, also present in the tumor, preferentially signals through MAPK, the use of MEK inhibitors could be considered. Finally, standard chemotherapy with carboplatin and pemetrexed could also be offered (18).
To the best of to our knowledge, this is the first case report of a patient with these coexisting molecular aberrations, EML4-ALK rearrangement and KRAS mutation. Oncogenic driving events are mutually exclusive in the vast majority of cases. However, in up to 3% of cases, 2 or more oncogenic drivers can be found in a single patient, as seen in this case report. Are these 2 different cell clones, with each carrying 1 molecular aberration, or is this a single clone carrying both? These questions will need to be answered in more detailed molecular studies (28). Nevertheless, scenarios like this support the use of panels testing for multiple molecular markers, simultaneously allowing for the identification of sentinel alterations, a deeper study of which could increase our understanding of the molecular biology in general and enable us to craft better personalized treatment strategies in particular.
Conclusion
In conclusion, the present report describes the coexistence of EML4-ALK translocation and KRAS mutation in a lung adenocarcinoma case responsive to crizotinib therapy. The good response to crizotinib suggests that the ALK translocation was the molecular driving event.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has any financial interest related to this study to disclose.