
Abstract
Background
A high neutrophil to lymphocyte ratio (NLR) is a strong predictor of poor survival in patients with colorectal, breast, pancreatic and lung cancers, while the prognostic value of NLR in gastric cancer is still controversial. The aim of our study was to determine the prognostic value of pretreatment NLR in a Chinese population of patients with gastric adenocarcinoma.
Methods
Our retrospective study used an unselected cohort of gastric adenocarcinoma patients treated in the Cancer Center of Sun Yat-sen University between January 2001 and December 2008. We used the data from 341 healthy individuals as controls to understand the difference of NLR between the gastric cancer patients and normal individuals. A total of 706 patients had a complete blood count (CBC) record prior to treatment. Cox regression analysis was used to evaluate the prognostic value of NLR.
Results
Gastric adenocarcinoma patients had a significantly higher NLR as well as neutrophilic granulocyte and lower lymphocyte counts compared with healthy individuals. By combining the nearby groups of NLR whose survival had no significant difference, we got a cutoff value for NLR of 3. Patients with a high NLR had a significantly lower survival rate than patients with a low NLR. On multivariate analysis, after adjusting for tumor stage and other clinicopathologic factors, high NLR turned out to be an independent risk factor for poor survival (p=0.016).
Conclusions
Gastric cancer patients had a significantly higher incidence rate of high NLR compared with healthy individuals. High pretreatment NLR in gastric cancer was an independent prognostic factor.
Keywords
Introduction
Approximately 1 million people are diagnosed each year with gastric cancer, making it the second most common cancer and the third leading cause of cancer-related death in China (1). The incidence of gastric adenocarcinoma varies widely according to geographic region and is particularly common in Asia (2). The prognosis for gastric adenocarcinoma patients remains poor (3, 4), and until now the most effective prognostic factor has been tumor-node-metastasis (TNM) stage. A few serum biomarkers were also found to be associated with poor prognosis in gastric adenocarcinoma patients (5, 6). The host inflammatory response to cancer cells is reported to be associated with tumor progression (7, 8). A large number of studies have focused on the search for surrogate biomarkers which are immunologically relevant and can serve as prognostic factors (9, 10). Increased numbers of neutrophils and/or decreased numbers of lymphocytes may suppress lymphokine-activated killer cells, thereby increasing the propensity to metastasis (11). The preoperative neutrophil to lymphocyte ratio (NLR) has frequently been reported to be related to patients’ inflammation status, clinical stage and survival in colon cancer, lung cancer and liver cancer as well as gastric cancer (12–13–14–15). However, limited information on the prognostic value of lymphopenia, neutrophilic leukocytosis (NL) and NLR in gastric adenocarcinoma patients in China has been reported. This study aimed to compare the prognostic significance of pretreatment lymphopenia, NL and high NLR in gastric adenocarcinoma patients.
Materials and Methods
Ethics statement
All patients provided written informed consent for their information to be stored and used in the hospital database. Study approval was obtained from independent ethics committee. At the Cancer Center of Sun Yat-Sen University. The study was undertaken in accordance with the ethical standards of the World Medical Association Declaration of Helsinki.
Patients and Methods
Patients
Between January 2001 and January 2008, the medical records of patients with pathology-proven gastric carcinoma who were diagnosed and received treatment in the Cancer Center of Sun Yat-Sen University were retrospectively analyzed. A total of 850 patients were enrolled in the study. We excluded 59 patients (8.2%) because of missing baseline characteristics, 75 patients (3.2%) with incomplete follow-up and 10 patients (0.6%) with secondary malignancy. None of the patients received neoadjuvant treatment. The final study involved 706 patients. Moreover, we enlisted 341 healthy individuals as controls. None of these healthy individuals had any history of malignant diseases. None of the patients or healthy individuals had any clinical evidence of active infection, presence of hematologic disorders, acute or chronic inflammatory or autoimmune diseases or prior steroid therapy. The healthy individuals underwent a physical checkup each year, and data for complete blood count were collected in 2012 when they underwent a routine examination.
The clinical features collected for subsequent analysis included sex (male or female), age at diagnosis (<59 or ≥59 years; median age was 59), tumor size (≤5 cm or >5 cm; median diameter was 5 cm), anemia (yes or no), thrombocytosis (yes or no), location of primary tumor (proximal or distal or total), histology subtypes (well + moderate differentiated adenocarcinoma or poor + signet ring cell differentiated adenocarcinoma), total number of lymph nodes retrieved (<15 or ≥15) and TNM stage (American Joint Committee on Cancer [AJCC], 7th edition of the staging manual) (16) (Tab. I).
Overall Survival Rates For Gastric Cancer Patients According To The Classification Of Neutrophilic Granulocyte, Lymphocyte And Nlr Intervals
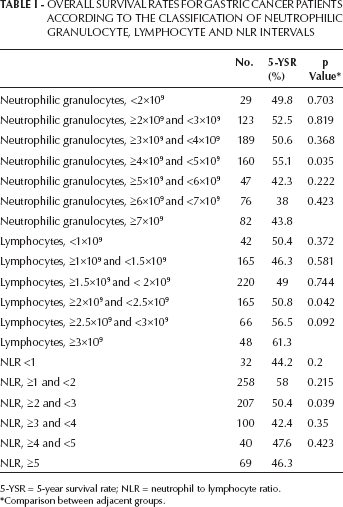
5-YSR = 5-year survival rate; NLR = neutrophil to lymphocyte ratio.
Comparison between adjacent groups.
During the study period, we did not have a standardized protocol for postoperative chemotherapy and (or) radiotherapy. Adjuvant therapy was considered in patients with T3-T4 classification and/or positive lymph node involvement. In the present study, only 451 patients (66.1%) completed the adjuvant chemotherapy (2-6 cycles). Agents using for chemotherapy included oxaliplatin, 5-fluorouracil, capecitabine, S-1, irinotecan, docetaxel and paclitaxel. The median number of cycles was 4. No patients received adjuvant radiotherapy. Until 1 January 2013, 374 patients had died from the disease.
Statistical analysis
All statistical analysis was performed with SPSS 16.0 software (SPSS Inc, Chicago, IL, USA). A p value <0.05 was considered to be statistically significant (2-tail). Disease-specific survival (DSS) was calculated by the method of Kaplan-Meier. For patients who remained alive, data were censored at the date of the last contact. Kaplan-Meier analysis with log-rank testing was used for univariate analysis. Variables showing a trend for association with survival (p<0.05) and variables that were known to have prognostic value were selected in the final multivariate Cox proportional hazards model (forward conditional model), while variables that were highly associated with others were excluded from the final multivariate Cox proportional hazards model. We compared the -2log likelihood (which was the parameter in the Cox regression) of the different multivariate models: the smaller the value of this statistic, the better the model. The chi-square test was used to compare the clinicopathologic data. Distributions of leukocyte parameters were presented as means and standard deviations (SD). The comparison of leukocyte parameters between healthy individuals and gastric adenocarcinoma patients was evaluated using the Kruskal-Wallis test.
Results
The gastric adenocarcinoma patients had a significantly higher neutrophil count (mean ± SD: 4.52×109 ± 2.34×109 vs. 1.50×109 ± 0.22×109, p<0.001), lower mean lymphocyte count (1.85×109 ± 0.66×109 vs. 2.4×109 ± 0.4×109, p<0.001) and higher mean NLR (2.98 ± 3.10 vs. 0.65 ± 0.2, p<0.001) compared with healthy individuals (Fig. 1A-C). The range of NLR for gastric adenocarcinoma patients was from 0.21 to 23.00, while for healthy individuals, it was from 0.46 to 4.8.

Comparison between gastric adenocarcinoma patients and healthy individuals. A) neutrophil to lymphocyte ratio B) neutrophil count C). lymphocyte count. Horizontal lines within boxes represent median values, and boxes denote values between the 25th and 75th percentiles. The p values were determined using the Mann-Whitney U-test.
Cutoff for neutrophilic leukocytosis, lymphopenia and high NLR intervals
Table I lists patient numbers and 5-year survival rates of different groups according to the number of their neutrophilic granulocytes (range 0.5×109 to 21.7×109, with an interval of 1.0×109), lymphocytes (range 0.3×109 to 4.3×109, with an interval of 0.5×109) and NLRs (range 0.21 to 23.0, with an interval of 1.0). By combining patients with similar prognosis, we found the cutoff values for neutrophilic granulocytes (cutoff value = 5×109), lymphocytes (cutoff value = 2.5×109) and NLR (cutoff value = 3).
Patient demographics
The median age of the 706 patients was 59 years (range 24-83 years). Among them, 481 were men and 225 were women. The overall 5-year survival for the whole group of patients was 50.1%. The median follow-up for the entire cohort was 48.0 months (range 3.0-175.0 months). The characteristics of the 706 gastric adenocarcinoma patients and the effects of clinical features on survival are summarized in Table II.
Demographics And Univariate Survival Analysis Results For Gastric Carcinoma Patients (N=706)

AJCC = American Joint Committee on Cancer; NLR = neutrophil to lymphocyte ratio; OS = overall survival; TNM = tumor-node-metastasis.
Tumor characteristics
Only 652 patients underwent a resection, so the T and N stages for the remaining 54 patients were unknown due to the distant metastasis. There were 52 T1 tumors (8.0%), 99 T2 tumors (15.2%), 29 T3 tumors (4.4%) and 472 T4 patients (72.4%). Median tumor size was 5 cm. There were 412 proximal tumors (gastroesophageal junction and proximal third of stomach) and 275 distal tumors. Their relationship with high NLR is shown in Table II. Patients with a high NLR tended to be older, have a larger tumor, higher incidence of thrombocytosis and higher incidence of metastasis (Tab. II).
Univariate and multivariate analyses of overall survival
Both univariate and multivariate analyses were used to evaluate factors relating to overall survival. The items of tumor size, degree of differentiation, T stage, N stage, M stage and TNM stage (AJCC, 7th edition), status of NL, lymphopenia and NLR were significantly related to overall survival (Tab. II).
For the multivariate regression analysis, we first set up a model including age, sex, size of tumor and degree of differentiation, T stage, N stage, M stage and status of NL. It showed that tumor size, T stage, N stage and M stage (AJCC, 7th edition) were independent factors for overall survival. The -2log likelihood was 1656.2. Then we set up a second model which is identical to the first except that the status of NL was replaced by the status of lymphopenia. It turned out that tumor size, T stage, N stage and M stage (AJCC, 7th edition) as well as the status of lymphopenia were independent factors for overall survival. The -2log likelihood was 1551.1. Finally we set up another model which is identical to the second except that the status of lymphopenia was replaced by the status of NLR. It turned out that tumor size, T stage, N stage and M stage (AJCC, 7th edition) as well as the status of NLR were independent factors for overall survival (Tab. III). The -2log likelihood was 1479.3. The 5-year survival for patients whose NLR <3 or ≥3 was 53.9% and 44.6%, respectively (p=0.018) (Fig. 2).
Three-Step Multivariate Analysis Of Overall Survival In Gastric Carcinoma

CI = confidence interval; LN = lymph node; AJCC = American Joint Committee on Cancer; T = tumor; N = node; M = metastasis; NLR = neutrophil to lymphocyte ratio.

Survival curves for patients with gastric adenocarcinoma stratified by pretreatment neutrophil to lymphocyte ratio (NLR) <3 and ≥3 (p=0.018); p values were determined using the log-rank test.
Discussion
Although several studies have suggested that NLR is a good indicator for the evaluation of the condition of host tumor status, the prognostic value of NLR in gastric cancer is still controversial (17–18–19). We once reported that leukocytosis was an independent prognostic factor in patients with cervical cancer, but not in patients with gastric cancer (20). Several studies in a variety of advanced cancers have shown that a high preoperative NLR was an independent prognostic factor for shorter survival (12–13–14–15). In our present study, the prognosis of patients with a high pretreatment NLR was significantly worse than that of patients with a low NLR. Multivariate analysis also confirmed that high pretreatment NLR was an independent prognostic factor.
Though in the univariate analysis, high NLR, NL and lymphopenia were all correlated with a shorter survival, in the multivariate analysis; NL was not an independent prognostic factor. Even though both high NLR and lymphopenia were independent prognostic factors in the multivariate analysis, the -2log likelihood was lower in the NLR model, which indicated that high NLR was a better prognostic factor than lymphopenia.
One possible explanation for this phenomenon is that the infiltration by lymphocytes has been reported to indicate the generation of an effective antitumor cellular immune response (21), and increased lymphocytic infiltration correlates with a better prognosis (7, 8). On the other hand, tumor-infiltrating granulocytes can promote tumor progression (22). Therefore a high NLR may reflect an enhanced neutrophil response and a weak lymphocyte response. The combination of these 2 effects finally leads to the promotion of tumor growth.
The cutoff value used in our study differed from those in previous reports (2.0, 2.5, 4.0 or 5.0) (17–18–19–20). In this study, we analyzed the overall survival according to the value of NLR, from the minimum level to the highest level, and combined the groups whose survival curve had no significant difference. Finally, we got the best cutoff value, 3.0, to distinguish patients with a poor prognosis from those with a good prognosis.
As for the relationship between the high NLR and clinical features of gastric cancer, we found that patients with high NLR tended to be older, have a larger tumor, higher incidence of thrombocytosis and metastasis. All of these factors were reported to be correlated with poor survival (3, 4, 10). The most important information was the relationship between the high NLR and higher incidence of metastasis. Though both of these 2 factors were independent prognostic factors in the multivariate analysis, this does not exclude the possibility that increasing metastasis is the mechanism of high NLR–related poor survival.
Furthermore, in our study, we compared the differences in NLR between gastric cancer patients and healthy individuals. It turned out that patients with gastric cancer had a significantly higher pretreatment NLR than healthy individuals. This indicated that high NLR may play a role in the tumorigenesis of gastric cancer.
The limitation of current study is in its retrospective analysis setting. Since peripheral blood cell count is a quick and easy assay to perform, measurement of the NLR may be useful as a clinical biological marker, not only to estimate tumor burden but also to predict prognosis in patients with gastric cancer.
In conclusion, this retrospective study demonstrated that high pretreatment NLR in gastric cancer was an independent prognostic factor. This study also revealed that gastric cancer patients had a significantly higher incidence rate of high NLR compared with healthy individuals.
Footnotes
list of Abbreviations
Acknowledgements
We thank Prof. Liu Qing in the Epidemiology Department for his assistance with the statistical analysis.