
Abstract
The dilution effect of high plasma volume contributes to a lower level of specific tumor marker such as prostate-specific antigen. To date, few studies have focused on this effect of other tumor marker levels. Therefore, we evaluated the dilution effects of a higher plasma volume on lowering the serum concentration of various tumor markers such as CA125 and CA19-9. Data from patients (age ≥40 years) visiting our public health center between March 2007 and March 2013 were gathered. A total of 19,439 male and 11,655 female native Koreans were eligible to have a serum CA125 and CA19-9 screening for ovarian and pancreatic cancer, respectively. CA125 levels in 11,234 women were analyzed. There was a statistically significant trend toward a lower likelihood of having a serum CA125 level >35 U/mL with increased body mass index (BMI), with obese men having a 53.1% lower likelihood than those with a normal BMI. After CA19-9 analysis in 29,978 participants, there was also a significant trend toward a lower likelihood of having a serum CA19-9 level >35 U/mL with increased BMI, with obese men having a 27.0% and obese women having a 32.7% lower likelihood than those with a normal BMI. These results might affect tumor screening efficiency for ovarian and pancreatic cancer using serum CA125 and CA19-9, respectively. Further studies are needed to better define these results in clinical practice.
Introduction
Tumor markers are substances produced by a tumor or secreted by tissue in response to a tumor. They may be used in the screening, diagnosis and classification of tumors, as well as in the prognostic assessment and monitoring of recurrence and metastasis in cancer cases (1). Men offered screening for prostate-specific antigen (PSA) (2) had a significant reduction in the rate of death from prostate cancer (3). Recently, a growing body of evidence suggests that obese men may have lower serum PSA (4–5–6–7–8). A proposed mechanism for the relationship between obesity and lower PSA is hemodilution. Banez et al (4) reported that PSA significantly decreased with increasing body mass index (BMI) due to dilution of a fixed amount of PSA in the greater plasma volume in larger-bodied patients. An inverse association could result in fewer screen-detected cancers, causing a decrease in the observed incidence of prostate cancer in obese men (9).
Our previous study showed that there was a statistically significant trend toward a lower likelihood of having a serum total PSA level ≥2.5 ng/mL with increased BMI, with obese men having an 18% lower likelihood than those with normal BMI (10). When this threshold was considered, there was an observable trend of decreasing PSA level with increased BMI, with significant point estimates of risk of an “abnormal” PSA among BMI groups (9).
CA125 is a well-known tumor marker for ovarian cancer, together with ultrasonography. In the last decade, much effort has focused on the performance of CA125 to improve its sensitivity (11). CA19-9 is a potential marker in the early detection of pancreatic cancer when used in the appropriate clinical setting (12).
Current tumor markers including PSA, CA125, CA19-9 and carcinoembryonic antigen (CEA) have common limitations that these markers are not cancer specific but rather disease specific, resulting in low specificity. Nevertheless, to date, there are no substitutable tumor makers for them. In this study, we hypothesized that if the dilution effect of high plasma volume contributes to a lower PSA, this effect may lower other tumor marker levels. Therefore, we evaluated the dilution effects of a higher plasma volume on various tumor markers including CA125 and CA19-9.
Materials and Methods
Data collection and study design
Male and female data (age ≥40 years) from the public health center attached to Soonchunhyang University Seoul Hospital was gathered between March 2007 and March 2013. A total of 19,439 male and 11,655 female native Koreans were eligible to have serum tumor marker tests, including CA125, CA19-9, CEA and α-fetoprotein (AFP) screening for ovarian, pancreatic, colorectal cancer and hepatoma, respectively. CA125 and CA19-9 were estimated using Architect i2000 (Abbott Diagnostic Laboratories, Abbott Park, IL, USA), CEA using Advia Centaur (Siemens Medical Solution, Erlangen, Germany) and AFP using Hitachi 7600-110 (Hitachi Ltd., Tokyo, Japan). The standard diagnostic cutoff values were CA125 (>35 U/mL), CA 19-9 (>35 U/mL), CEA (>5 ng/mL) and AFP (>20 ng/mL). All anthropometric measurements were made by trained observers using standardized techniques. BMI was defined as weight (kg) divided by the square of height (m2). Subjects were then classified as nonobese (BMI <25) or obese (BMI ≥25) according to the Asia-Pacific criteria of obesity (13). This study was approved by our institutional review board.
Statistical analysis
Mean and standard deviation (SD) were used to describe statistical data. All variables were nonparametric variables as determined by the Kolmogorov-Smirnov normality test. A logarithmic transformation of all variables was performed to ensure a more normal distribution and back-transformed for interpretation. A p value was calculated by using the independent t-test for continuous variables and the Pearson chi-square test for categorical variables. Thresholds of tumor markers were used to categorize each value as normal or abnormal for analyses. To describe the association between obesity and the likelihood of a certain serum CA125 or CA19-9 level, logistic regression analyses were used after dichotomizing men as having a CA125 or CA19-9 level >35 U/mL. The odds of having an abnormal CA125 or CA19-9 level for each threshold were then calculated, using men with a normal BMI as the reference group. SPSS 14.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analyses, and p values <0.05 were considered statistically significant.
Results
CA125
Table I gives the demographics of the CA125 study population. Mean age was 50.9 years (range 40-86), which was significantly younger in the nonobese group than in the obese group. Data from 11,234 of 11,388 total women (98.6%) were analyzed. One hundred four were excluded because of data loss. Among the 11,234 women, 277 (2.47%) had an abnormally high CA125 level (>35 U/mL). Mean CA125 was significantly lower in the obese group than in the nonobese group. Univariate analyses revealed that the likelihood of having a CA125 level >35 U/mL in the nonobese group (2.78%) was significantly higher than in the obese group (1.32%) (p<0.001) (Tab. I). After controlling for age, there was a statistically significant trend toward a lower likelihood of having a serum CA125 level >35 U/mL with increased BMI, with obese men having a 53.1% lower likelihood than those with a normal BMI (Tab. II).
Demographics Of Study Population For Ca125
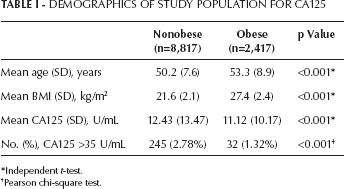
Independent t-test.
Pearson chi-square test.
Odds of Having a Serum CA125 >35 U/mL, According to Obesity
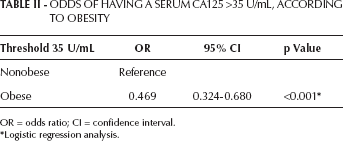
OR = odds ratio; CI = confidence interval.
Logistic regression analysis.
CA19-9
Mean age for this study group was 50.8 years (range 40-90). Of the 30,132 total study subjects for CA19-9, 154 were excluded due to insufficient data, for a total of 29,978 participants analyzed (male to female ratio 62.6%/37.4%). Among them, 856 (2.86%) had an abnormally high CA19-9 level (>35 U/mL). The positive rate in women (5.35%) was much higher than that in men (1.37%) (p<0.001). Univariate analyses revealed that the likelihood of having a CA19-9 of >35 U/mL in the nonobese group was significantly higher than in the obese group in both men (p=0.019) and women (p<0.001) (Tab. III). After controlling for age, there was a statistically significant trend toward a lower likelihood of having a serum CA19-9 level >35 U/mL with increased BMI, with obese men having a 27.0% (p=0.018) and obese women having a 32.7% (p<0.001) lower likelihood than those with a normal BMI (Tab. IV).
Demographics Of Study Population For Ca19-9
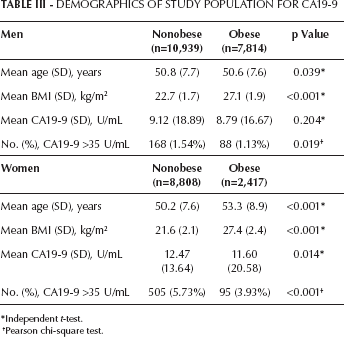
Independent t-test.
Pearson chi-square test.
Odds of Having a Serum CA19-9 >35 U/mL, According to Obesity
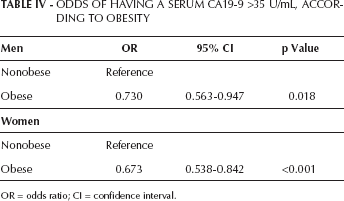
OR = odds ratio; CI = confidence interval.
CEA and AFP
Among 30,738 participants, 285 (0.93%) had a CEA level >5 ng/mL. The chi-square test revealed that there was no difference according to obesity (nonobese 0.95%, obese 0.88%, p=0.570) in the likelihood of having an abnormal CEA. AFP showed a very low positive rate (41/30,631 participants, 0.13%) over cutoff value, which was statistically insignificant.
Discussion
Obese men are known to have a significantly higher rate of prostate cancer deaths but lower serum PSA concentrations compared with nonobese men (14, 15). It has been suggested that obese men experience a prostate cancer detection bias due to hemodilution of PSA that can result in delayed prostate cancer diagnosis and subsequent delay in treatment (4). Yang showed that there was a statistically significant trend toward a lower likelihood of having a serum PSA level ≥2.5 ng/mL with increasing BMI and that obese men had an 18% lower likelihood compared with men with a normal BMI (10). If obesity leads to a clinically significant decrease in PSA, this would suggest that the PSA thresholds used in clinical practice should be adjusted based on BMI. Likewise, the current study revealed that there was a significantly lower likelihood of having “abnormal” serum CA125 or CA19-9 levels with increased BMI, than in those with a normal BMI.
CA125 is a tumor antigen that is elevated in the majority of ovarian cancers and has shown increases in some women with early stage disease (16). Few data have been published concerning the association of CA125 concentration and obesity. CA125 has been reported to be inversely correlated with the presence of metabolic syndrome and the numbers of metabolic syndrome components such as obesity (16, 17). The possible mechanism is assumed to be that subjects with a greater BMI have larger plasma volumes, which could lead to hemodilution of soluble tumor markers, a similar phenomenon with PSA (17). Johnson et al attempted to elucidate the usual pattern of CA125 levels among populations of women without ovarian cancer (16). Among women 55 to 74 years of age not diagnosed previously with ovarian cancer, the odds ratio (OR) of obese patients having an elevated CA125 level was significantly decreased (OR=0.53, 95% confidence interval [95% CI], 0.39-0.71) compared with the normal weight group, similar to the results from our current study (OR=0.469, 95% CI, 0.324-0.680) (16). In the same study, the mean CA125 level was 11.9 U/mL, with a very low percentage of women (1.6%) having values greater than the standard clinical threshold of 35 U/mL, while the current study demonstrated a higher mean CA125 (12.15 U/mL) and higher positive rate (2.47%) over cutoff. The reason for these differences is not clear. Besides obesity, CA125 level is influenced by a number of factors, including race/ethnicity, age, hysterectomy, smoking, etc. Therefore, we believe that the different age distribution and/or different ethnicity between the 2 study groups may have affected the results.
So far, CA19-9 is the standard tumor marker for pancreatic cancer. CA19-9 has proven to be useful in differentiating benign and malignant pancreatic disease (12). Among our study population, 2.86% had an abnormally high CA19-9 level (>35 U/mL), and the positive rate in women (5.35%) was significantly higher than that in men (1.37%). However, regardless of sex, there was a significantly lower likelihood of having an abnormal CA19-9 value with increased BMI, with obese men having a 27.0% and obese women having a 32.7% lower likelihood than those with a normal BMI. Chang et al revealed that a higher BMI was significantly associated with lower CA19-9 levels in a screened Korean male population (18).
In our current study, the positive rates of CEA and AFP were very low (0.93% and 0.13%, respectively); therefore, it was difficult to assess the relation between obesity and these markers due to the weak statistical power. Colon cancer and hepatoma are the second and fourth most prevalent cancer in Korean men (19). We believe that these tumor markers were inappropriate to use for screening the normal population.
In this study, there were several limitations. First, as we have documented before, these tumor markers are not cancer specific but rather disease or organ specific. Hence, benign conditions which cause the elevation of those tumor markers should be considered. However, in our study we did not consider those confounding factors, because we wanted to investigate only the casualty of dilutional effect of obesity in those tumor markers. PSA can be affected by benign conditions such as prostatitis, and CA125 can be affected by menstruation and endometriosis or greatly by pregnancy (20, 21). CA19-9 is affected by pancreatitis, too (20, 22). Second, this study was not considered for cancer status, which is the fundamental part of a tumor-screening study. However, this study is based on the data by screening population, and real cancer status could not be discerned if a serial workup for the national cancer network was not done. Moreover, the results are taken from an electronic medical recording system and no data are available about the analytical variations of the employed methods during the course of the study. Lastly, the International Association for the Study of Obesity has proposed a criterion for obesity as a BMI ≥30 based on data from a white population. In contrast, for people from the Asia-Oceania region, for whom the main form of energy intake is carbohydrates, obesity has been defined as a BMI ≥25 (13). This difference in BMI cutoff is quite large and could have had an effect on the study results. If we had used the Western criteria for obesity in the CA19-9 study population, only 3.0% (890 of 29,978) of the participants would have been classified as obese. Therefore, we believe our results might not be applicable to populations in other countries. The current study was not community-based, and we had no additional evidence as to whether these men were perfectly healthy. These points highlight limitations of our study.
Conclusions
In our study, obese women had a 53.1% lower likelihood of having a CA125 level >35 U/mL compared with nonobese women in a screened Korean population. Also, there was a significant trend toward a lower likelihood of having a serum CA19-9 level >35 U/mL with increased BMI, with obese men having a 27.0% and obese women having a 32.7% lower likelihood than those with a normal BMI.