
Abstract
Purpose:
Serum markers with increased sensitivity and specificity for endometrial cancer are required. To date, no good marker has met this standard. The aims of our study were to evaluate the utility of tumor markers HE4, CA125, CA724, and CA19-9 as potential markers in patients diagnosed with endometrial cancer.
Methods:
Blood samples from 105 patients with endometrial cancer and 87 healthy women were analyzed by Roche electrochemiluminescent immunoassay, and serum values were measured for the following biomarkers: HE4, CA125, CA724, and CA19-9.
Results:
Serum HE4, CA125, CA724, and CA19-9 concentrations were significantly higher in patients with endometrial cancer, compared with controls (P < .001). In the receiver operating characteristic analysis, the area under the curve value for combination of HE4, CA125, CA724, and CA19-9 was 82.1% (95% confidence interval: 75.3%-86.2%), the maximum area of the test groups. For all stages of patients with endometrial cancer, HE4 had higher sensitivity (58%), positive predictive value (60%), and negative predictive value (67%) than any other single tumor marker, and in the combination of HE4, CA125, CA724, and CA19-9, the sensitivity and positive predictive values reached 59.1% and 88%, respectively. Meanwhile, the receiver operating characteristic area under the curve of the combination of the 4 markers was significantly increased than any other group, either in stage I or in stage II to IV cases. HE4 and CA125 both correlate with advanced age; in addition, HE4 was related to pathology subtypes and positive adnexal involvement, CA125 was related to International Federation of Gynecology and Obstetrics stage, CA19-9 was related to International Federation of Gynecology and Obstetrics stage, and CA724 was correlated with positive lymph node.
Conclusion:
Combination of HE4, CA125, CA724, and CA19-9 has the highest value in diagnosing endometrial cancer, and they can be a useful tissue immune marker for patients with endometrial cancer.
Introduction
Endometrial cancer (EC) is the most common gynecological malignant tumor in Western countries, and its incidence has risen rapidly in Asia. 1,2 Most patients with EC exhibit symptoms such as postmenopausal bleeding and vaginal discharge uterine and have well-differentiated endometrioid in histology that leads to the diagnosis of the malignancy in the early stages of the disease (type I ECs). However, people at high risk, including women with systemic and advanced stage disease, may benefit from a serum marker for early detection. In addition, sensitive and specific serum markers could help to monitor the effect of treatment and screen recurrence or metastasis of EC. Unfortunately, to date, no serum marker is universally utilized for patients with EC. 3,4 In the present report, we have analyzed the serum level of HE4, CA125, CA724, and CA19-9 in single and combined, in order to evaluate their clinical value in EC.
Materials and Methods
Preoperative serum samples from 105 patients with EC were collected at First Affiliated Hospital of Zhengzhou University between February 2013 and March 2014. Moreover, serum samples of 87 controls (women without gynecological pathologies) were collected. The study was approved by the institutional review board, and all enrolled patients provided written informed consent. The International Federation of Gynecology and Obstetrics (FIGO) stage, histologic type, pathologic grade, myometrial invasion, and pelvic lymph nodes metastasis that were based on the criteria of the FIGO and the World Health Organization were established in all cases. 5 –8 A total of 105 cases with EC including 85 cases with endometrioid adenocarcinoma, 6 cases with serous papillary adenocarcinoma, 6 cases with clear cell carcinoma, and 8 cases with mixed adenocarcinoma were included. Of the 105 patients with EC, 74 (70%) were diagnosed with stage I disease, 10 (10%) with stage II disease, 16 (15%) with stage III disease, and 5 (5%) with stage IV disease. The average age of patients with EC is 54 years (range: 33-71 years). Eighty-seven healthy controls are selected from physical examination in our hospital by women staff members, whose average age is 53 years (range: 28-74 years). Patient population characteristics are shown in Table 1.
Patient Population Characteristics.

Abbreviation: FIGO, The International Federation of Gynecology and Obstetrics.
All blood samples were collected in the preoperative period, then centrifuged for 5 minutes with the serum withdrawn, and frozen at −80°C until analysis. Serum levels of HE4, CA125, CA724, and CA19-9 were detected by electrochemiluminescence. Reagents were provided by Roche Group. Serum samples were detected by Roche cobas e601 modules. The experiment was strictly operated according to the instruction and operation manual. Critical values of HE4, CA125, CA724, and CA19-9 separated were 140 pmol/L, 35 U/mL, 6.9 U/mL, and 37 U/mL, respectively.
Statistical Analysis
Data analysis was performed by SPSS 13.0 statistical analysis software. Median method (quartiles) was used to present quantitative data of skew distribution. Mann-Whitney test was used to assess difference between the 2 groups. Relationship between categorical variables was assessed using χ2 test. Logistic regression models were estimated for each marker separately and for all combination of markers to differentiate between patients with EC and healthy controls. Receiver operating characteristic (ROC) curves were constructed, and the areas under the curve (AUCs) with binomial exact 95% confidence intervals (95% CIs) were calculated. 9 The diagnostic performance of tumor markers was also performed by sensitivity, positive predictive values (PPVs), and negative predictive values (NPVs). A level of P < .05 was accepted as statistically significant for all comparisons.
Results
The serum marker levels of HE4, CA125, CA724, and CA19-9 were evaluated in the 2 groups (Table 2). There was a significant difference between EC and healthy control. Serum levels of HE4 and CA125 were significantly elevated between EC and healthy control.
Serum Markers in 2 Groups.

We used ROC analysis to evaluate diagnostic performance of the markers in distinguishing malignant from normal conditions. The areas under the ROC (ROC-AUCs) curves for a single marker and combinations of biomarkers for all stages of EC are presented in the first column in Table 3. In the single detection, HE4 has a greater ROC-AUC (76.3%) than the other markers. Combination of HE4, CA125, CA724, and CA19-9 has the highest ROC-AUCs (82.1%) in all groups.
AUC, Sensitivity, PPV, and NPV of Controls Versus Malignant for Individual and Combined Tumor Markers for All Stages of Endometrial Cancers.

Abbreviations: AUC, under the curve; NPV, negative predictive value; PPV, positive predictive value; ROC-AUC, areas under the receiver operating characteristic curves.
Sensitivity, PPV, and NPV for the detection of single and combined tumor markers for all stages of EC are shown in Table 3. Sensitivity of combined CA19-9, CA125, and CA724 (40.6%) is lower than HE4 alone (58%) but has higher PPV (0.65 vs 0.6) and NPV (0.8 vs 0.67). Combined HE4, CA125, CA724, and CA19-9 has higher sensitivity, PPV, and NPV than combined HE4, CA125, and CA724, but this difference was not statistically significant (P > .05).
The ROC-AUCs for single markers and marker combination assays for stage I and stage II to IV cases are presented in Table 4. Detection of the ROC-AUCs for single tumor marker revealed that HE4 had a significantly higher ROC-AUC when compared with CA125, CA724, or CA19-9, both in stage I and stage II to IV patients (74.9% and 84.4%, respectively). The combination of HE4, CA125, CA724, and CA19-9 had the largest ROC-AUC for any triplet combination of markers, no matter in stage I or stage II to IV group (76.8% and 89.9%, respectively).
ROC-AUCs Curves for Individual and Combined Tumor Marker Assays for Stage I and Stage II to IV Endometrial Cancers.

Abbreviation: ROC-AUC, areas under the receiver operating characteristic curves.
The relationship between positive rate of tumor markers and the clinicopathological features is shown in Table 5. Positive rate of HE4 was significantly associated with advanced age at diagnosis, higher pathology grade, and positive adnexal involvement group and was irrelevant to FIGO stage, pathology subtypes, and histologic type. Positive rate of CA125 was obviously associated with advanced age and higher FIGO stage but also not related to pathology subtypes and histologic type. Positive rate of CA19-9 was associated with higher FIGO stage and positive lymph nodes, and CA724 was associated with positive lymph nodes.
Clinical and Pathological Characteristics of Patients With Endometrial Cancer and Association With Tumor Marker Levels.a
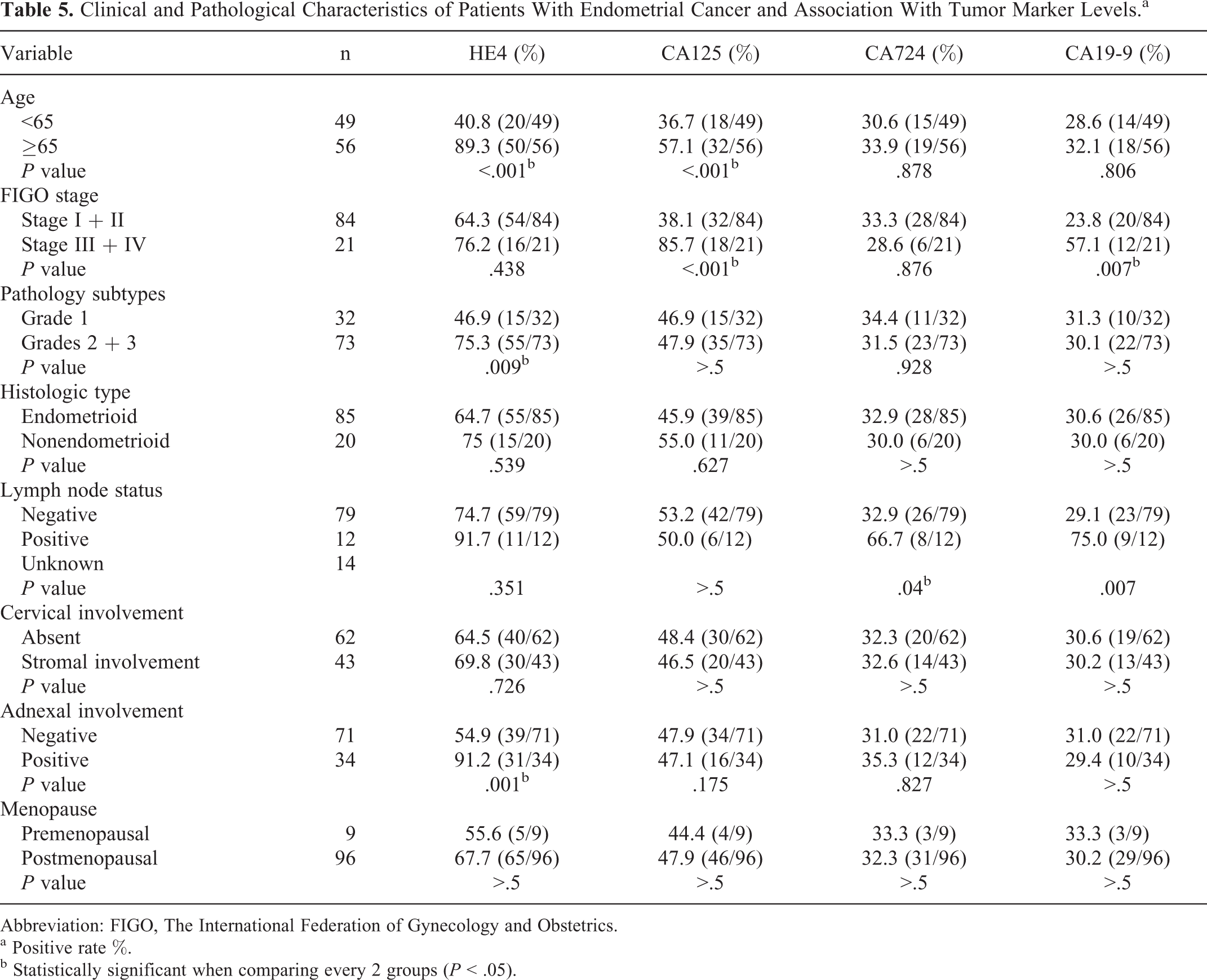
Abbreviation: FIGO, The International Federation of Gynecology and Obstetrics.
a Positive rate %.
b Statistically significant when comparing every 2 groups (P < .05).
Discussion
Endometrial carcinoma is one of the most common female malignant tumors; its incidence is the third in malignant tumor of female reproductive organs. Patients with EC could be seen with abnormal postmenopausal bleeding or vaginal discharge in the early stage; however, a large number of patients still be diagnosed in its latest stages. So a panel of specific serum markers for early detection and prognostic assessment would be useful for improving the survival rate of patient with EC. The serum CA125 was considered to be the most effective tumor marker for EC but have poor diagnostic sensitivity. 10 –12 Besides CA125, EC also could be diagnosed by elevated levels of HE4, CA724, and CA19-9, each with their own unique advantages. 13 –15
In our test, we detected serum level of HE4, CA125, CA724, and CA19-9 in 105 patients with EC; the results showed that the level of tumor markers was obviously higher in the EC group than that in the healthy controls. Sensitivity of HE4 in patients with EC was 58%, much higher than sensitivity of CA125, CA724, and CA19-9 (35.4%, 11.3%, and 16.3%, respectively). Our data showed that combined detection of the 4 tumor markers had the highest sensitivity (59.1%) but had little difference with combined detection of HE4, CA125, and CA724 (58.6%).
By comparing the AUCs, we found that combined detection of HE4, CA125, CA724, and CA19-9 showed a statistical significance when compared with any combination of 3 or single tumor marker(s). The ROC-AUC of HE4 was significantly higher than any single tumor marker. This suggests HE4 have significance for EC screening and have higher accuracy in detection than CA125, CA724, or CA19-9 (Tables 3 and 4).
According to 2011 NCCN (National Comprehensive Cancer Network) guidelines for revision of EC clinical stage, age status, pathology subtypes, FIGO stage, histologic type, lymph node status, and cervical stroma invasion, adnexal involvement and menopause are important factors for EC prognosis. In our research, we found that HE4 and CA125 were both related to advanced age; furthermore, HE4 was also associated with pathology subtypes and positive adnexal involvement; CA125 was related to FIGO stage but not relevant with pathology subtypes. The serum CA19-9 was related to FIGO stage, and CA724 was associated with positive lymph node. Besides this, the worse histologic classes, the later clinical stage, and the metastatic lymph node were associated with the higher rate of HE4, CA125, CA19-9, and CA724. So combined detection could help clinicians for prognosis evaluation and rational treatment exploration.
In conclusion, HE4, CA125, CA19-9, and CA724 all have good early diagnostic value. For patients with all stages of EC, combined detection of HE4, CA125, CA19-9, and CA724 has the equal sensitivity but higher PPV and NPV compared with combined HE4, CA19-9, and CA724. As a single marker, HE4 performed the best effective feature in both stage I and stage II to IV cases. The ROC-AUC of the combination of HE4, CA125, CA724, and CA19-9 was obviously higher compared to any other group, especially in stage II to IV group. According to relationship between the 4 markers and EC-related prognostic factors, patients can be classified and appropriately treated. Combined detection of the 4 markers should be promoted for EC biochemical properties, diagnosis, and treatment. Moreover, the 4 markers have different relationships with EC clinical and pathological characteristics, and combined detection has more advantages than single detection in improving the prognosis of patients with EC.
Footnotes
Abbreviations
Acknowledgments
The authors thank Xuna Wang, Weitao Zhu, and Peiguo Zheng (Department of Tumor Immunity, The First Affiliated Hospital of Zhengzhou University) for technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Medical science and technology research projects, Henan, People’s Republic of China (No. 201303075, 201403035) and Scientific research key project fund of Henan province education department, Henan, People’s Republic of China (project No.13A310622).