
Abstract
Objectives
Methods
Results
Conclusions
Introduction
Lung cancer is one of the main causes of death in the world (1), and is projected to be responsible for up to 30% cancer-related deaths in the coming years (2). The high incidence of lung cancer is due to increased environmental pollution and use of carcinogens; moreover, in the Indian setting, the main causative factors are smoking, oral use of tobacco, and alcohol consumption. Approximately 63,000 new cases of lung cancer are reported in India each year, and this type of cancer is considered as a disease of smokers (3, 4). Between the 2 types of lung cancer, namely non-small cell lung cancer (NSCLC) and small cell lung carcinoma, NSCLC accounts for 80% of all lung cancer-related deaths. In patients with NSCLC, the survival rate is less than 5% despite surgical interventions at initial stages (5). The treatment of NSCLC is complicated due to different responsiveness to targeted therapeutics; these differences are associated with specific mutations, deficiency in apoptotic control, DNA repairing capacity, and regulation at cell cycle checkpoints (6-7-8). NSCLC is also characterized by genetic and epigenetic changes, and hence is considered as a heterogeneous group of diseases requiring routine mutational profiling. NSCLC detected in smokers or never-smokers is respectively characterized by the activation of the signaling molecules Kirsten rat sarcoma viral oncogene (KRAS) and epidermal growth factor receptor (EGFR) (9). Though multiple risk factors such as gender, geographical distribution, as well as environmental, genetic, and viral factors are all associated with the incidence of NSCLC, no specific etiologic factors are associated with NSCLC, especially in never-smokers.
A widely accepted screening tool for the detection of lung cancer is not yet available, though routine chest X-ray analyses and low dose computer tomography are both used. Biomarker-based approaches, among which comet assay, micronucleus test (MNT), PCR, immunohistochemistry, and florescence in situ hybridization (FISH) are also employed. The comet assay is widely accepted as a genotoxicity test for the assessment of genetic damage, as it enables the easy detection of various forms of DNA damage (10, 11). The assay is characterized by the formation of a distinct head and a tail resembling a “comet”, of which the tail length is directly proportional to the amount of DNA damage (12, 13). The association between DNA damage and cancer risk (14-15-16-17-18-19), including lung cancer, has been reported (7, 20, 21). The comet assay has been widely used to detect (22, 23) lung cancer, as well as to assess the influence of cell-cycle checkpoints in developing lung cancer (7). In peripheral lymphocytes of NSCLC patients the detection of DNA adducts (24, 25), DNA damage, and apoptosis (26) have also been reported using the comet assay. Chromosomal abnormalities have been linked to the etiology of cancer pathogenesis (27) and can be detected by cytokinesis-blocked micronucleus (CBMN) assay or MNT (27) in peripheral lymphocytes of NSCLC patients (28, 29).
The use of peripheral blood lymphocytes for the detection of cancer is possible, is minimally invasive, and prominently reflects the amount of genetic damage in the precursor cells that led to the carcinogenic process in the target tissues (30). As an example, excision repair proteins in lymphocytes serve as a marker of susceptibility to squamous cell carcinomas of the head and neck (23). Despite the significant improvements in imaging techniques, treatment strategies, and novel anti-cancer drugs, there has been no increase in the survival rate of NSCLC patients in the last 3 decades (31, 32). Physicians believe that any cancer, including NSCLC, can be cured when detected in its smallest and earliest stages. This underscores the need to detect NSCLC at early stages for proper diagnosis and treatment, especially in the Indian population, in which smoking, tobacco chewing, and alcohol consumption are widespread. It is also important, in the Indian setting, to generate epidemiological data that can corroborate the findings worldwide about the risk factors associated with NSCLC. Considering the multiracial, geographic, and lifestyle characteristics of the Indian population, it is rather difficult to correlate the risk factors associated with NSCLC throughout the country. Hence, specific epidemiological studies that can address the risk factors associated with NSCLC in the South Indian population are important. By analyzing peripheral lymphocytes of lung cancer patients from the Andhra Pradesh region of South India, we here evaluated the possible confounding factors that might play a role in causing NSCLC.
Materials and Methods
Study Population
A total of 246 NSCLC patients were included in the study conducted at the Indo-American cancer Hospital, in Hyderabad, India, during the period June 2006 - January 2010. Patients were classified using the revised lung cancer staging system (33). A total of 250 age and gender-matched healthy controls (apparently healthy and without a history of cancer or any other chronic disease) were recruited among the general population of the same geographic region. The study was approved by the ethics committee of the Indo-American Cancer Hospital, Banjara Hills, Hyderabad. Informed and educated consent was collected from all lung cancer patients and controls. Sociodemographic characteristics such as age, gender, lifestyle (alcohol, diet, etc.), occupational exposure (working hours/day, years of exposure, use of protective measures, etc.), history of smoking, number of cigarettes per day, and duration of smoking were collected using a standard questionnaire. Smokers were considered as current smokers at the time of diagnosis. Ex-smokers were defined as subjects who had smoked at least 100 cigarettes during their life. The smoking status of the subjects was calculated as the average tobacco consumption expressed in pack-years. The pack-years were computed as the number of cigarettes smoked per day multiplied by the duration of smoking in years.
Micronucleus Test
The MNT was performed as already described (34, 35). Whole blood cultures were incubated with cytochalasin-B (5 mg/mL) at 37ºC for 72 hours in duplicates. The cultures were harvested by centrifugation and lymphocytes were subjected to mild hypotonic treatment with 0.075 M KCl for 5 minutes, and then fixed using a solution of methanol and acetic acid (3:1). The cell suspension was smeared on pre-cooled microscopic slides, air dried, and stained with 10% Giemsa for 10 minutes. A total of 2x103 binucleated lymphocytes (103 cells per culture) were scored at a 400X magnification and the frequency per 1,000 cells was calculated.
Comet Assay
The comet assay was performed as described earlier (36). Frozen microscopic slides were pre-coated with 100 µL 1% molten agarose prepared in PBS, covered with cover slips, and allowed to gel at 4°C for 10 minutes. A 10-µL lymphocyte suspension (separated by density gradient centrifugation), was mixed with 110 μL of low melting agarose prepared in PBS, and coated onto microscopic slides, then covered with a cover slip and placed on ice to allow agarose to form a second layer. A third layer of 110 μL of low melting agarose was coated onto the slides and allowed to gel at 4°C for 10 minutes. Slides were incubated overnight in ice cold lysing solution (2.5 M NaCl, 100 mM EDTA, 10 mM Tris-HCl, and 1% Triton X-100) and then in denaturation solution (0.3 M NaOH, 10 mM EDTA pH 13.1). After electrophoresis the slides were drained, washed twice in distilled water, incubated in neutralizing solution (0.4 M Tris-HCl, pH 7.5), dehydrated in absolute methanol for 10 minutes, and air-dried. Silver staining was performed (37) to score the comets, and a total of 100 individual cells per subject were screened. The tail length was measured using an ocular meter fitted in the eyepiece of the transition microscope and calculated as: comet tail length (µm) = maximum total length - head diameter.
Statistical Analysis
The results are expressed as mean ± standard deviation. Statistically significant differences were analyzed using the Student's t test. ANOVA (analysis of variance) was used for comparisons among 3 or more groups. Multiple linear regression analysis was performed to assess the association of DNA damage and micronuclei with the independent variables. The results were considered to be significant at p values less than 0.05. All calculations were performed using the SPSS statistical software. To avoid complexity, only the significance levels <0.05 are shown.
Results
The demographic features of NSCLC patients and healthy controls are presented in Table I. The percentage of never-smokers was significantly higher among healthy controls than lung cancer patients (69.08% vs 39.84%). By contrast, the percentages of ex-smokers and current smokers were significantly higher among lung cancer patients than among healthy controls (respectively 17.07% vs 4.35% and 43.08% vs 26.57%; p<0.001). Surprisingly, an approximately equal number of non-smokers (39.84%) and smokers (43.08%) were affected by lung cancer. Among the current smokers, the number of pack-years did not seem to influence the incidence of cancer initiation. It is also worthwhile to note that 15.45% of the NSCLC patients were passive smokers.
GENERAL CHARACTERISTICS OF THE STUDY GROUP
Indicates a p<0.05 when compared to controls.
The majority of healthy controls and lung cancer patients did not consume alcohol, with a significantly higher percentage among healthy controls (89.6% vs 61.38%; p<0.01). However, the percentage of alcohol-consumers was significantly higher among lung cancer patients than among healthy controls (38.62% vs 10.4%; p<0.01). Surprisingly, among lung cancer patients, those who did not consume alcohol were more than those who did (61.38% vs 38.62%; p<0.01).
Histopathological evaluation revealed that while 48.65% of lung cancer patients had adenocarcinoma, 43.24% had squamous cell carcinoma. At diagnosis, most patients presented with advanced cancer stages, i.e. stage IV (58.11%) followed by stage III (34.23%). However, none of the patients was diagnosed with stage I cancer.
The comet assay performed on peripheral lymphocytes revealed that the tail length was significantly higher in lung cancer patients than healthy controls (6.07±0.09 vs 2.05±0.04) (Fig. 1A). The mean comet tail length in peripheral lymphocytes of male and female NSCLC patients (respectively 6.28±0.11 and 5.51±0.14) was significantly higher than their respective healthy controls (2.14±0.05 and 1.81±0.05) (Fig. 1A). In all the categories of smokers the mean comet tail length was significantly higher among NSCLC patients than their respective controls (Fig. 1B). Among NSCLC patients the mean comet length was significantly higher in smokers (6.79±0.10) than ex-smokers (5.59±0.23) and non-smokers (3.47±0.16). When compared to healthy controls, a significant increase in comet tail length was observed among all NSCLC patients, and this increase seemed to correlate with the stage of the disease (stage II to stage IV) (Fig. 1C). When considering the samples obtained at different cancer stages, the mean comet tail length was significantly higher in stage IV (6.84±0.11) compared with stage III (5.42±0.10) and stage II (4.16±0.24), as well as in stage III compared with stage II (Fig. 1C). Based on histology findings, the samples from NSCLC patients were divided into squamous carcinoma, adenocarcinoma, and large cell lung carcinoma. A significantly increased comet tail length was observed in all histological subtypes when compared to the controls (Fig. 1D). Furthermore, among the histological subtypes, a significantly higher mean comet length was observed in both squamous cell carcinoma (6.41±0.13) and adenocarcinoma (6.08±0.12) samples when compared to large cell carcinoma samples (5.18±0.33) (Fig. 1D).
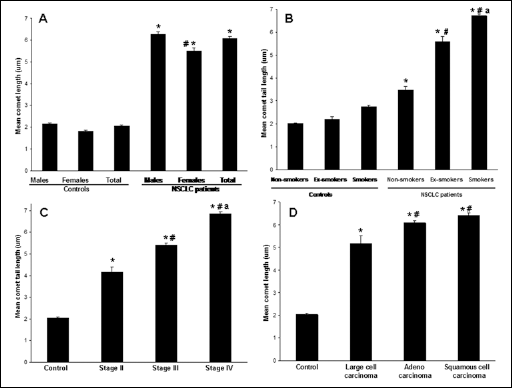
Factors that influence the genomic damage in peripheral lymphocytes of healthy controls and NSCLC patients. Peripheral lymphocytes isolated from healthy controls and NSCLC patients were subjected to comet assay, and the mean comet length for each subject was scored in 100 cells and calculated as comet tail length (µm) = maximum total length - head diameter. Values shown are mean ± SD.
Chromosomal damage in peripheral lymphocytes, as assessed by the MNT, was also significantly increased in lung cancer patients compared to the controls (5.60±0.12 vs 2.32±0.05) (Fig. 2A). The micronuclei frequency in the peripheral lymphocytes of male and female NSCLC patients (respectively 5.57±0.11 and 5.22±0.17) was significantly higher when compared to their respective healthy controls (2.74±0.04 and 2.48±0.05) (Fig. 2A). Although we observed a significant difference in the mean comet tail length (Fig. 1A) between male and female NSCLC patients, such difference was not found in the occurrence of micronuclei (5.57±0.11; 5.22±0.17) (Fig. 2A). The smoking status had a profound effect on the occurrence of micronuclei in NSCLC patients (Fig. 2B). Within the NSCLC patients' group, the frequency of micronuclei formation was significantly increased in smokers (5.98±0.15) compared to either ex-smokers (4.84±0.09) or non-smokers (4.45±0.04). Conversely, in healthy controls the smoking status did not have any effect (Fig. 2B). Micronuclei formation in the peripheral lymphocytes obtained from patients presented at different stages of NSCLC was higher than their healthy counterparts (Fig. 2C). Within the NSCLC patients' group the increase in micronuclei formation was found to be stage-dependent. Similarly to the observations made with the comet assay, we found a significant difference in the frequency of micronuclei formation between stage II and stage III cancers (4.92±0.09 vs 5.63±0.16) and between stage III and stage IV cancers (5.63±0.16 vs 6.12±0.14) (Fig. 2C). We then classified NSCLC patients on basis of their histopathological characteristics and analyzed the frequency of micronuclei formed in each of the groups. There was no significant difference among the number of micronuclei formed in the adenocarcinoma, squamous carcinoma, and large cell carcinoma groups (Fig. 2D).
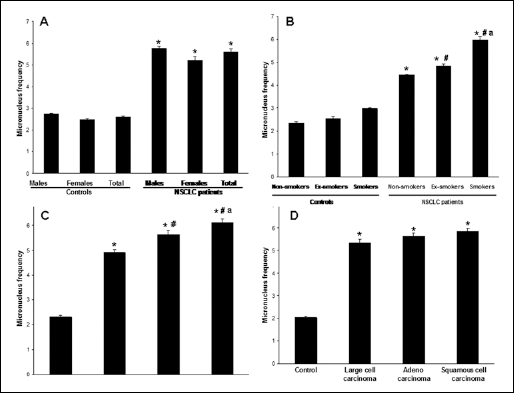
Factors that influence micronuclei formation in peripheral lymphocytes of healthy controls and NSCLC patients. Lymphocytes from peripheral blood were isolated and the occurrence of micronuclei was assessed. A total of 2x103 binucleated lymphocytes (103 cells per culture) were scored at a 400X magnification and the frequency per 1,000 cells was calculated. The values shown are mean ± SD.
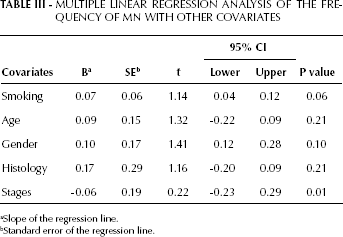
Multiple regression analysis considering DNA damage and chromosomal damage together with other measured parameters showed that age, gender, and histology of NSCLC were non-significant predicting factors (Tabs. II and III). Smoking status and lung cancer stage were the strongest predictors, as evidenced by the increased tail length (respectively p=0.02 and p=0.03) and micronuclei frequency (respectively p=0.06, a borderline significance, and p=0.01).
MULTIPLE LINEAR REGRESSION ANALYSIS OF COMET TAIL LENGTH WITH OTHER COVARIATES
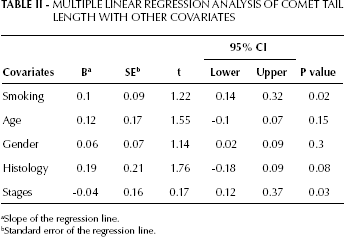
Slope of the regression line.
Standard error of the regression line.
MULTIPLE LINEAR REGRESSION ANALYSIS OF THE FREQUENCY OF MN WITH OTHER COVARIATES
Slope of the regression line.
Standard error of the regression line.
Discussion
Among the strengths of our study is the fact that it specifically includes patients from a South Indian population, from whom we obtained information using a standardized questionnaire and interviews performed by experienced professionals. The results here obtained are valuable to assess the prevalence of NSCLC in the South Indian population of Andhra Pradesh, which hitherto had not been reported. The weakness of this study lies in the fact that the samples were collected at a tertiary hospital, which is generally referred by district-level medical centers. Since many of the people referred to tertiary care centers may not be able to travel due to logistic, social, and ethical issues, it would have been more appropriate to select patients from primary or secondary health care centers.
We observed that the majority of healthy controls were non-smokers, whereas among the NSCLC patients smoking was prevalent, thus suggesting a positive correlation between smoking and incidence of NSCLC. Previous studies also demonstrated that NSCLC is associated with smoking (38, 39). With regard to smoking, we also observed the lack of a significant difference among NSCLC patients based on the number of pack-years. It has been reported that the number of cigarette pack-years can be a prognostic factor for the development of NSCLC (40). Furthermore, it was also demonstrated that the total smoking exposure, or smoking duration, and not the intensity (per pack-year) is a major contributing factor for the development of lung cancer (41). Since none of the patients in this study were diagnosed at stage I, it becomes more complicated to assess the correlation between the number of pack-years and the actual initiation of lung cancer.
An interesting observation in our study is that the incidence of NSCLC was comparable between non-smokers and smokers, which is in contrast with the standard belief that the incidence of NSCLC is associated with smoking. Our observation is supported by previous studies (42-43-44). The occurrence of lung cancer among non-smokers indicates that, besides smoking, other factors, such as lifestyle, are also among the determining factors. This is also evident from the results of this study, in that alcoholism was more prevalent among NSCLC patients than their healthy counterparts; in addition, among NSCLC patients the majority were alcohol-abusers. In the Indian context, the odds ratio between alcohol consumption and occurrence of lung cancer was found to range from 1.13 to 7.8 (4, 45-46-47). Interestingly, in the present study, we found that among NSCLC patients there were more non-alcohol abusers than alcohol-abusers, thus indicating that besides smoking and alcoholism, other lifestyle or environmental factors could also contribute to the onset of lung cancer. The lower number of alcohol-abusers in the population sampled in our study (considering healthy controls and patients together) could be due to their diverse demographic, ethnic, educational, and social backgrounds. Further studies are needed to generate more evidence that can determine the relationship between the levels of alcohol consumption and NSCLC-related deaths, so that effective community measures can be implemented.
We found that adenocarcinoma occurred in 48.65% of the patients, followed by squamous cell carcinoma. It is believed that squamous cell carcinoma was the predominant form of NSCLC until the 1970's, and that there has been a shift in the pathological features of NSCLC, with adenocarcinoma becoming the more frequent pathological subtype (48). Furthermore, until 2004, in the Indian context the incidence of squamous cell carcinoma seemed to be predominant (49, 50). Based on the results obtained in this study, it is possible that the pathological shift could be now happening in the Andhra Pradesh population. None of the patients in this study was diagnosed at stage I. This could be due to current clinical diagnosis patterns, by which a non-smoker presenting with a lung-related problem is not subjected to cancer screening as part of the differential diagnosis, thereby delaying the detection of NSCLC, which was found to occur at around 143 days after onset (51). Adding to this is the misdiagnosis of non-smokers with tuberculosis. This underlines the need to change the diagnosis patterns among clinicians as well as to generate lung cancer awareness in the general population about the need for a routine health checkup.
Since the mechanisms inducing chromosomal and DNA damage are similar in different tissues, the evaluation of these same mechanisms in peripheral lymphocytes truly reflects the extent of damage in cancer-prone tissues and the risk of cancer (52, 53). The comet assay and the MNT are recommended as standard biomarker assays for a variety of cancers, including NSCLC (27, 54, 55). The sensitivity of lung cancer to radiotherapy and chemotherapy, as well as the microenvironment of the tumors with specific reference to hypoxic conditions can be predicted with the comet assay and MNT (54). Using the comet assay, the extent of DNA damage in the peripheral lymphocytes of bladder cancer patients (56) and IR-induced lung cancer patients was reported (7, 21, 30). Furthermore, micronuclei formation is a manifestation of chromosomal instability often observed in cancer; measurement of these events in peripheral lymphocytes allows accurate diagnosis and provides a closer insight into the molecular mechanisms of genome damage (27). We observed that the mean tail length in NSCLC patients was significantly higher than in healthy controls. Specifically, in NSCLC patients the mean comet tail length was the highest in current smokers compared to ex-smokers and non-smokers. However, the same observation was not true for healthy controls. Furthermore, among NSCLC patients, the DNA damage seemed to be higher in males than females. Earlier studies reported similar findings as significantly higher levels of DNA damage were observed in males when compared to females in an Indian population (57). In the Indian context, this could be due to the predominant smoking habit in males. Furthermore, the different number of males and females included in the current study might have affected our results. Surprisingly, we observed that the micronuclei frequency in the present study was not different between genders. Similar observations were reported earlier (58) in patients with mesothelioma.
Cigarette smoking is a serious risk factor for lung cancer (18), and in the Indian population it is related to both tobacco chewing and smoking (45). Besides cigarettes, smoking of Bidi (made of crude particles of dried tobacco leaves wrapped in a tendu or temburni leaf, rich in tar and nicotine) (59) is predominant in the South Indian population, especially in rural areas and among low-income groups. The association between smoking and DNA damage reflected in peripheral lymphocytes has already been reported (30). We observed an increased mean comet tail length frequency among smokers of the NSCLC group. These results further strengthen the concept that the risk of cancer increases with smoking and alcohol consumption. From our data is not clear whether the compounding factor is either the cigarette or bidi consumption, thus requiring further specific studies on this issue.
A significant correlation between DNA damage, stage of the disease, and histopathological status of NSCLC patients was observed in this study. The increased DNA damage could be due to oxidative stress as the disease progresses. Measuring DNA damage using the comet assay and MNT could be of potential diagnostic value to assess the cancer's stage and histopathological features. Using the comet assay it was demonstrated that NSCLC patients have a higher risk of developing secondary malignancies (60). Since we found a positive correlation between the mean tail length, the frequency of micronuclei formation, and the cancer stage, the results of our study may provide valuable information to predict the actual cancer stage using the comet assay and MNT. We also observed that among the histopathological subtypes of NSCLC there was no substantial difference in the mean comet tail length or frequency of micronuclei formation. This suggests a limitation on the use of the comet assay and MNT in diagnosing NSCLC patients.
In conclusion, we found a strong association between smoking, alcohol consumption, and the incidence of NSCLC in the South Indian population of Andhra Pradesh. At the same time, it was surprising to observe the high occurrence of NSCLC in non-smokers and non-alcohol abusers, suggestive of the increasing changes in the lifestyle patterns polarizing towards the risk of developing lung cancer. The comet assay and MNT could be potential diagnostic tools to assess the cancer stage, thereby representing a valuable aid in providing better treatment strategies.
Footnotes
Acknowledgements
The authors thank all the study subjects who voluntarily participated in the study. The authors also thank the Director of the Institute of Genetics, Osmania University, for providing the necessary infrastructure needed to perform the study.