
Abstract
Purpose
The use of ten clinical “warning signs” has been suggested as a screening tool to identify patients that may have primary immunodeficiency (PID) conditions in adulthood. This study aimed to evaluate the presence of these “warning signs” among a cohort of patients with periprosthetic joint infections (PJI), in order to detect those cases that may have had a PID contributing to development of infection.
Methods
A descriptive study using our institutional PJI database was conducted. 185 patients with more than 15 medical consultations in our healthcare network before the diagnosis of PJI were considered eligible for the study. The presence of the “warning signs” was retrospectively evaluated using medical records.
Results
Twenty-seven patients (14.5%) presented with one or more “warning signs” of PID; however, 24 of the individuals had another immunocompromising condition and were thought to suffer secondary immunodeficiency. Among the remaining 3 patients, PID was confirmed in 1 individual who was found to have hypogammaglobulinemia.
Conclusions
It appears that some patients who develop PJI could suffer from a primary immunodeficiency status that may be detected using “warning signs” questionnaire. The administration of these questions to patients with multiple infections may lead to identification of a primary immunodeficiency status which may in turn influence the outcome of elective arthroplasty or PJI, when develops.
Introduction
Periprosthetic joint infection (PJI) is a devastating complication after hip and knee arthroplasty. For that reason, clinical and basic researchers have invested efforts in developing strategies for primary, secondary and tertiary prevention. Among the most important advances in primary prevention is the identification of risk factors predisposing to PJI. Various studies have reported risk factors for PJI, such as diabetes, obesity, previous surgery, and so on (1-3). More recently, some scores have been proposed to calculate the risk of future PJI based on the individual characteristics and comorbidities (4, 5).
Despite the advances, to our knowledge, no studies have explored the role of the immunologic status as a potential contributor during the pathophysiological process of PJI. In recent years, the concept of “primary immunodeficiency (PID) in adults” has been used to describe patients with no predisposing factors for infection who consequently develop a variety of infections (6). It is estimated that 1 in 1200 people in the United States may be afflicted with PID that may manifest in adulthood (7).
Around 180 disorders have been described that place adult patients at a risk of multiple infections. Investigators interested in this concept have developed 10 clinical “warning signs” that could be used to identify adult patients with PID conditions (8). The principle behind the screening is that some of these patients may have a treatable disorder, that when treated could limit medical complications.
The aim of this study was to evaluate the prevalence of the ten “warning signs” of PID in adults among a cohort of patients with hip and knee PJI treated at our institution.
Patients and Methods
This study was approved by the institutional review board. Using our institutional database of PJI, we were able to assemble a descriptive study including a universe of 772 patients treated for PJI at our institution from 2000 to 2012. Inclusion criterion was more than 15 consultations at our healthcare network facilities before the diagnosis of PJI. We decided to do so in order to obtain reliable data concerning past medical conditions and treatments received at our institution, thus easily collected from our medical records. Different medical specialists, such as family physicians, internists, etc, conducted the medical consultations.
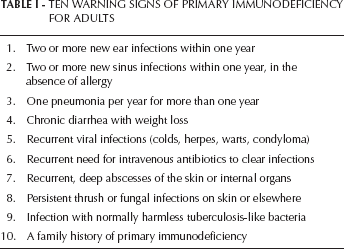
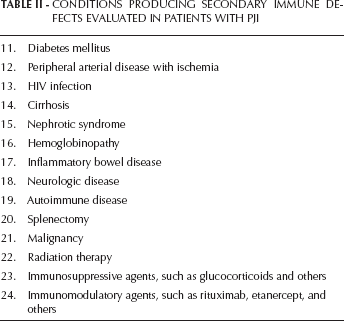
Retrospectively, all medical records were manually checked. From the 772 initial patients, 185 had more than 15 medical consultations before the diagnosis of PJI and were considered eligible for this study. All medical records were scrutinized to check for the presence of any of the “warning sings” for PID (Tab. I). In addition, we also evaluated for conditions that could potentially lead to secondary immunodeficiency (Tab. II).
TEN WARNING SIGNS OF PRIMARY IMMUNODEFICIENCY FOR ADULTS
CONDITIONS PRODUCING SECONDARY IMMUNE DEFECTS EVALUATED IN PATIENTS WITH PJI
In those patients with “warning signs” of PID and the absence of potential causes of secondary immunodeficiency, the confirmation of a PID was assessed in the medical records.
Results
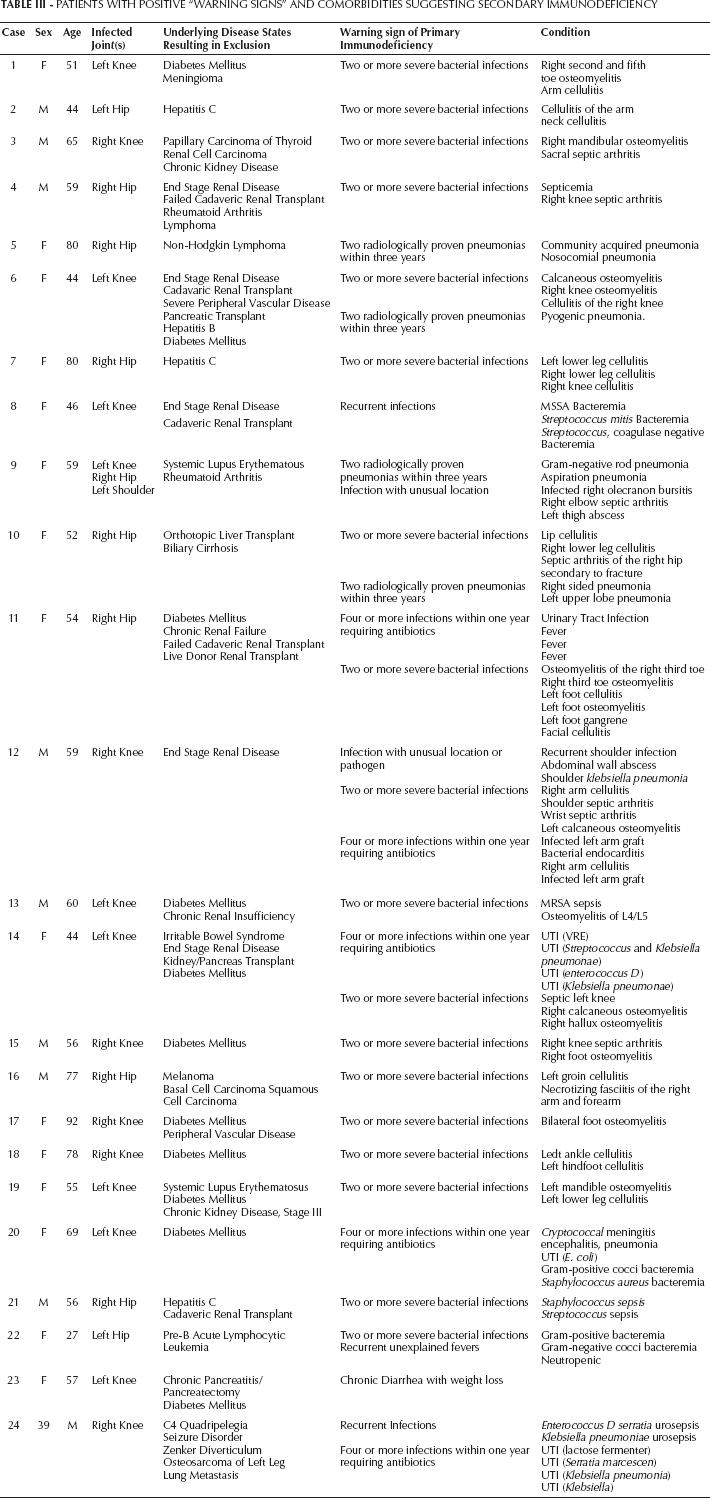
Among the 185 patients included, 27 (14.5%) presented with one or more “warning signs” of PID. Twenty-four of these twenty-seven patients (88%) had comorbidities that may have been potentially related to secondary immunodeficiency (Tab. III) and were thus not considered patients with a probable PID.
PATIENTS WITH POSITIVE “WARNING SIGNS” AND COMORBIDITIES SUGGESTING SECONDARY IMMUNODEFICIENCY
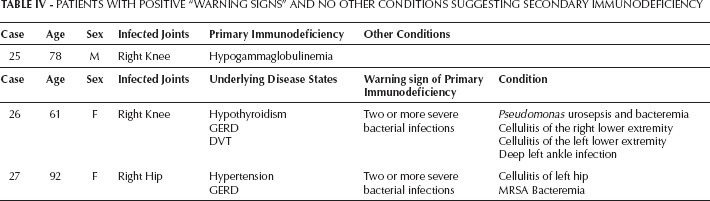
Only three patients had “warning signs” of PID and the absence of potential causes for secondary immunodeficiency. One patient with a knee PJI was diagnosed with hypogammaglobulinemia. In the other two patients the presence of a PID was not suspected nor confirmed by the attending physician (Tab. IV). Finally, the prevalence of confirmed PID in our cohort was 0.5%, but potentially it could be 1.6%. Unfortunately, none of these patients were available at the moment of this study to confirm the diagnosis of PID. It is important to disclose that our design does not allow us to calculate the sensitivity and specificity of the “warning signs” in our cohort.
PATIENTS WITH POSITIVE “WARNING SIGNS” AND NO OTHER CONDITIONS SUGGESTING SECONDARY IMMUNODEFICIENCY
Discussion
Our descriptive study demonstrated that the presence of “warning signs” of PID is not a rare event among a cohort of PJI patients. However, a majority of these patients presented with medical conditions that may produce a secondary immunodeficient state, thus potentially predisposing the patient to PJI. A PID was demonstrated only in one patient whereas in the other two cases the diagnosis was not verified.
PID can be classified in categories such as: 1) defects in immunoglobulins and/or complement proteins; 2) granulocyte (neutrophil) defects and 3) defects in cell mediated immunity. Although a vast majority of patients are diagnosed with PID during childhood due to recurrent infections, it has been proposed that in adults these conditions are more frequent than expected. The reason this may be true is because some of the disorders are of mild to moderate severity (selective IgA deficiency, IgG subclass immunoglobulins, etc) and thus not frequently identified. However, it is important to remark that in adults with recurrent infections, secondary immune disorders due to comorbidities (i.e diabetes) or pharmacologic treatments (i.e corticosteroids) are much more common than PID, which is concordant with our observation. In our study, the only confirmed case was a patient in whom the final diagnosis was hypogammaglobulinemia, which is defined as a plasmatic level of immunoglobulin (Ig) under 5 g/L (9). In adults, this disorder is mainly secondary to lymphoproliferative disease and more rarely due to PID. As the patient was lost to follow up, we could not know his evolution.
We feel that these “warning signs” provide a new scope for the evaluation of patients with conditions predisposing them to PJI. Although these signs appear to be of minor relevance to specifically detect a PID (10), they certainly may serve as another tool to identify patients with an inherent increased risk of infection and allow for active management by the appropriate medical specialist. For instance, if a diabetic patient with a previous medical history of two recent skin infections or pneumonia, it may be a reasonable indicator that his or her immunologic status is not optimal. This patient may require further study and management before offering an elective total joint replacement.
Our study is a simple descriptive study presenting two main limitations. The first is its retrospective nature. In order to improve the accuracy of the information contained in the past medical history while optimizing data collection, we decided to include only patients with more than 15 consultations at our healthcare network. Although we established that number arbitrarily, we feel that the information contained in the medical charts in patients with more than 15 clinical visits previous to the diagnosis of PJI was sufficient to identify the presence of the “warning signs”. Using this criterion, our sample size was considerably reduced; however the final sample of 185 patients seems to be adequate for our purposes. The second limitation is the screening tool used to evaluate the probable presence of a PID. The “warning signs” have been criticized because of their lack of accuracy in some studies (11). However, we decided to use them because of their simplicity and more importantly because of the feasibility to be used in this retrospective study. Our observations demonstrated that the “warning signs” were not a good indicator of the presence of PID, because only one patient was finally diagnosed with that disorder. However, they may offer a new alternative to improve our screening tools in patients at risk of PJI. It is important to notice that 14% of the patients presented with at least one of these signs. We believe that a prospective study would better evaluate the predictive properties of these signs for the development of PJI.
In conclusion, the “warning signs” of PID may serve as an additional tool to improve the pre-operative evaluation in patients at risk of PJI.
Footnotes
Financial support: None.
Conflict of interest: Consultant: Zimmer, Smith & Nephew, ConvaTec, TissueGene, CeramTec, Medtronic. Royalties: Elsevier, Wolters Kluwer, Slack, Datatrace, Jaypee Publishers. Stock Options: CD Diagnostics, Hip Innovation Technology, PRN.