
Abstract
Purpose:
To investigate the association of DNMT3B -283T>C polymorphism with the risk of lung or gastric cancer, which was followed by a meta-analysis.
Methods:
The genotyping of -283T>C was performed by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and was confirmed by sequencing.
Results:
The results of this case-control study showed that -283T>C was not associated with the risk of lung or gastric cancer, and further stratified analysis according to age, gender, smoking status, and alcohol status confirmed the present finding. However, data from a meta-analysis in the Asian population revealed a significant association between -283T>C and lung cancer risk in the allelic model (C vs. T: odds ratio [OR] = 1.28, 95% confidence interval [CI], 1.06-1.55, p = 0.01) and two genetic models (CC vs. TC: OR = 1.29, 95% CI, 1.04-1.59, p = 0.02; CC vs. TC + TT: OR = 1.30, 95% CI, 1.06-1.60, p = 0.01).
Conclusions:
These results provided evidence that the DNMT3B -283T>C polymorphism might significantly contribute to the lung cancer risk in the Asian population, but not the gastric cancer risk in the Chinese population.
Introduction
Lung cancer (LC) and gastric cancer (GC) have been the leading cancers with a high incidence and mortality rate for many years in China, especially in the Hubei province (1-3). Clinically, surgical resection has been the primary treatment for the earlier stage of LC and GC patients because of its high therapeutic efficiency (2, 4). Unfortunately, most LC and GC are detected in patients at the advanced stage, during which period the surgical resection is no longer appropriate for the treatment of tumors (4, 5). Thus, an effective early diagnosis strategy is urgently needed.
As a key epigenetic modifier, DNA methylation plays an essential role in tumorigenesis (6-8). In mammals, DNA methylation patterns are established by the de novo methyltransferases (DNMT3A and DNMT3B) (6, 7, 9). Interestingly, accumulated evidence has demonstrated that DNMT3B promotes tumorigenesis, and abnormal expression of DNMT3B is responsible for the aberrant DNA methylation in carcinogenesis (10, 11).
Currently, genetic association studies are a powerful approach for identifying the susceptibility of the genetic variation underlying complex diseases, like cancer (12). Single nucleotide polymorphisms (SNPs) are the most common form of human genetic variation, and thus may contribute to an individual’s susceptibility to cancer. Moreover, certain SNPs in the promoter region of genes have been shown to influence promoter activity and gene expression (13, 14). Thus, some promoter SNPs of the DNMT3B gene may be able to influence its DNA methylation enzymatic activity, thereby modulating the susceptibility to LC and GC. Until now, the following three polymorphisms in the DNMT3B gene promoter region have aroused much interest: -149C>T (rs2424913, in the transcription start site), -579G>T (rs1569686, in the exon 1B transcription start site) and -283T>C (rs6087990, in the exon 1A transcription start site). However, in vitro luciferase assays have shown that -283T>C, but not -149C>T or -579G>T, is the real functional SNP that is able to alter the DNMT3B promoter activity (15, 16).
Recently, -283T>C has been widely studied to explore the association of DNMT3B with the risk of cancer (15, 17-21). However, the results from previous studies remain conflicting rather than conclusive. Moreover, none of the studies so far have attempted to evaluate the association between -283T>C with susceptibility to LC and GC in the Hubei Chinese population.
The meta-analysis is a statistical tool for combining the results from different studies on the same topic, thus increasing statistical strength and precision (22). In view of this, we conducted a meta-analysis combining results from previously published literature and our case-control study herein performed in the Chinese population of Hubei province, to provide a more precise estimation of the association between DNMT3B -283T>C with the risk of LC and GC.
Material/subjects and methods
Subjects
A total of 550 LC patients, 460 GC patients, and 800 normal controls were recruited in the current study. All subjects were Chinese and living in Hubei province. The normal controls were selected from cancer-free individuals who visited Wuhan Xinzhou District People’s Hospital for regular physical examinations, or who volunteered to participate in the epidemiology survey during the same period. The LC and GC patients were confirmed histopathologically and were volunteers recruited from the Hubei Cancer Hospital and Wuhan Xinzhou District People’s Hospital. This study was approved by the Ethical Committees of Wuhan University of Technology, and written informed consent for the genetics analysis was obtained from all subjects or their guardians.
The genotyping of DNMT3B -283T>C polymorphism
Samples were collected into blood vacuum tubes containing ethylenediaminetetra-acetic acid (EDTA) and stored at 4°C. Genomic DNA was extracted within 1 week of sample collection by proteinase K digestion as previously described (23). The transition of T>C of rs6087990 creates a BanI restriction site, and polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to detect the -283T>C polymorphism in the exon 1A transcription start site of the DNMT3B gene. The primers for PCR reaction were: 5-GAAAAAGGCCCCAGAAGGCG-3 (forward) and 5-GGCGGGGACGAGGGAAATTT-3’ (reverse). For quality control, 20% randomly selected PCR-amplified DNA samples were examined by DNA sequencing, and the results were 100% concordant.
Statistical analysis
The chi-square test was used to compare the differences in age, gender, smoking status, and alcohol status between patients and normal controls. Genotypic frequency of -283T>C was tested for departure from the Hardy-Weinberg equilibrium (HWE) using the χ2 test. To evaluate the association between DNMT3B -283T>C and cancer risk, OR (odds ratio) and 95% confidence intervals (CIs) were calculated by unconditional logistic regression analysis. All statistical tests were two-tailed with p<0.05 set as the significance level, and were performed using SPSS 15.0 software (SPSS).
Meta-analysis
We searched the all publications updated to March 2017 from the PubMed, EMBASE, and ISI Web of Science databases without language restriction. The following words were searched: “DNMT3B or DNA methyltransferase 3B,” “rs6087990/-283T>C,” and “lung cancer or gastric cancer.” References listed in retrieved articles were also checked for missing information. Next, the studies were eligible for inclusion in the meta-analysis if they met the following criteria: (i) studies on humans; (ii) investigation of the DNMT3B -283T>C and risk of LC or GC; (iii) case-control study design; (iv) valid data were accessible to estimate the OR and its 95% CI; and (v) HWE equilibrium should be established in controls.
We calculated the departure from the HWE for the controls in each study using Pearson’s goodness-of-fit χ2 test. Different ethnicity descents were categorized as Asian and Caucasian. The analyses were conducted in Review Manager 5.3 (Cochrane Collaboration). Heterogeneity was evaluated with the χ2 test and the inconsistency index (I2). By the heterogeneity test, heterogeneity was considered significant when p<0.1 was consistent with possible substantial heterogeneity. If p≥0.1, we used the fixed-effect model to calculate the combined OR (the Mantel–Haenszel method) (24), otherwise, the random-effects model (Der Simonian and Laird method) was conducted (25). The significance of combined OR was determined by the Z test.
Results
The characteristics of LC patients, GC patients, and normal controls are presented in Table I. The distributions of age, gender, smoking status, and alcohol status did not differ significantly between LC patients and normal controls, and between GC patients and normal controls, which suggests that matching based on these 4 variables was adequate.
Characteristics of LC patients, GC patients and normal controls
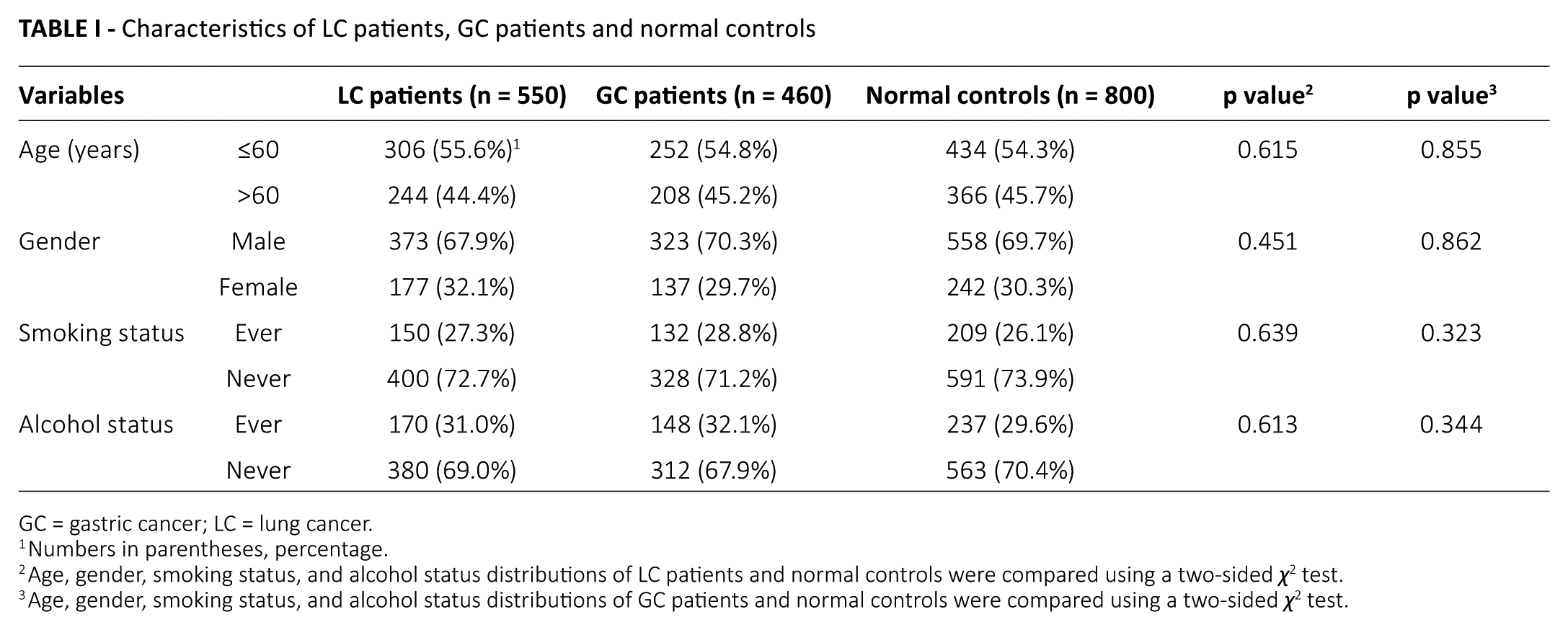
GC = gastric cancer; LC = lung cancer.
Numbers in parentheses, percentage.
Age, gender, smoking status, and alcohol status distributions of LC patients and normal controls were compared using a two-sided χ2 test.
Age, gender, smoking status, and alcohol status distributions of GC patients and normal controls were compared using a two-sided χ2 test.
In this study, the DNMT3B -283T>C was successfully genotyped in a total of 1810 subjects. No significant deviation from HWE was observed for -283T>C in normal controls (p = 0.916), which suggests that the enrolled control subjects were representative. Table II shows the allele and genotype distributions of -283T>C and its association with the risk of LC and GC. The distributions of -283T>C allele were similar in LC patients and normal controls (p = 0.077), and in GC patients and normal controls (p = 0.193). Concordantly, there was no significant association between -283T>C genotypes and the risk of LC or GC in 5 genetic models (CC vs. TC, CC vs. TT, TC vs. TT, CC vs. TC + TT, and CC + TC vs. TT). These results indicate that the DNMT3B -283T>C polymorphism might not be associated with the risk of LC or GC in the Chinese population.
Genotype and allele distributions of DNMT3B -283T>C polymorphism and its association with the risk of LC and GC
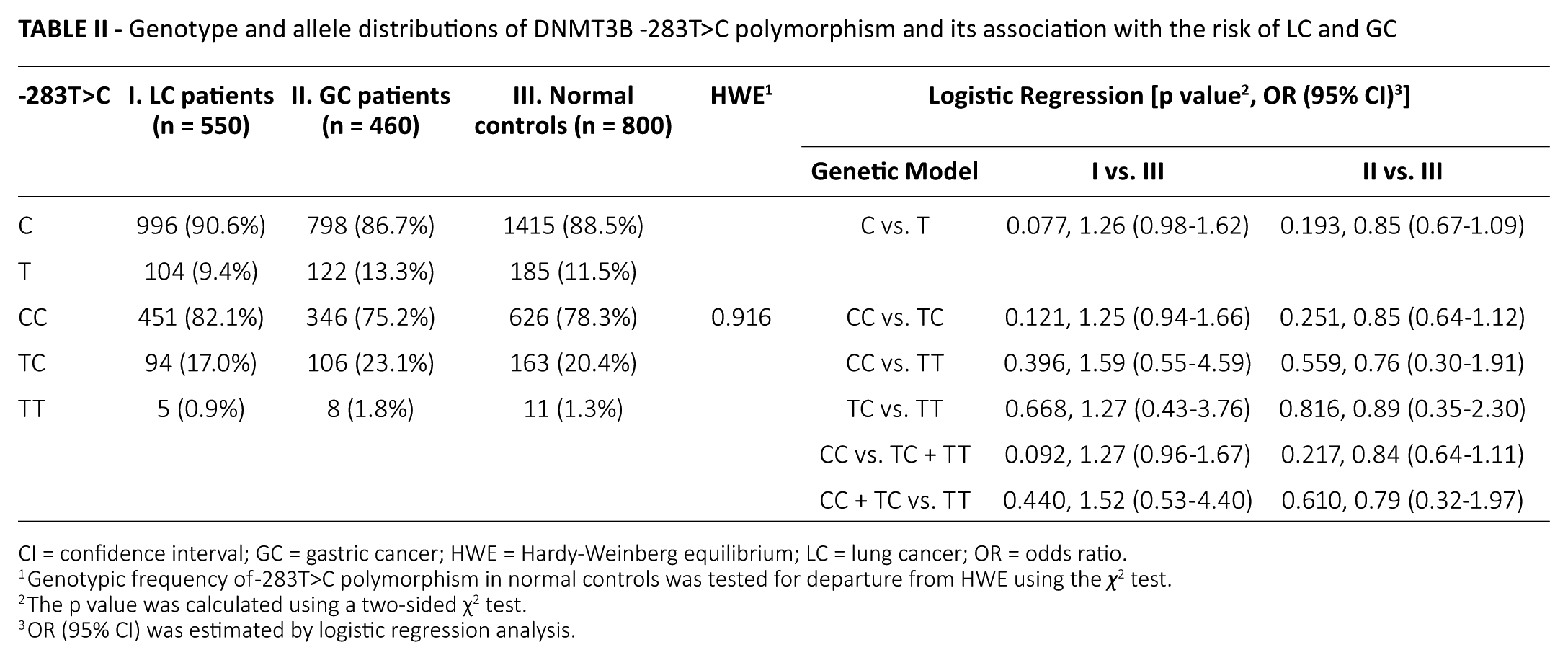
CI = confidence interval; GC = gastric cancer; HWE = Hardy-Weinberg equilibrium; LC = lung cancer; OR = odds ratio.
Genotypic frequency of -283T>C polymorphism in normal controls was tested for departure from HWE using the χ2 test.
The p value was calculated using a two-sided χ2 test.
OR (95% CI) was estimated by logistic regression analysis.
Age, gender, smoking, and drinking were important factors in lung and gastric carcinogenesis (2, 26). Therefore, a stratified analysis of -283T>C according to age, gender, smoking status, and alcohol status was performed in this study (Tab. III). All genotype frequencies were in agreement with the HWE among normal controls in each subgroup (p>0.05). Similarly, no significant association of -283T>C and the risk of LC or GC was found in any stratified factors, which suggests that these factors might not affect the association between -283T>C and the risk of LC and GC.
Stratification analysis of DNMT3B -283T>C genotype and allele according to age, gender, smoking status, and drinking status in LC and GC patients
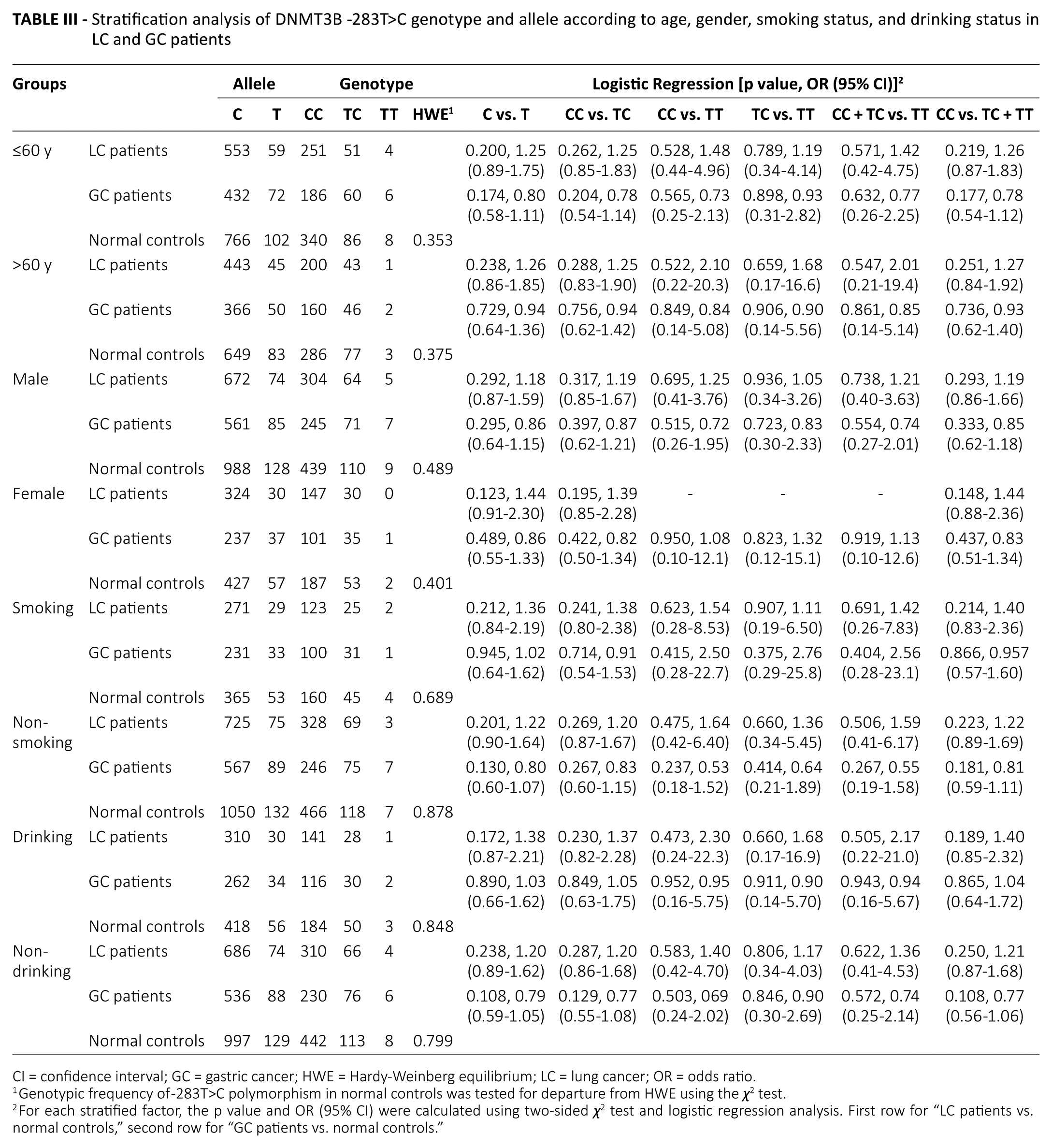
CI = confidence interval; GC = gastric cancer; HWE = Hardy-Weinberg equilibrium; LC = lung cancer; OR = odds ratio.
Genotypic frequency of -283T>C polymorphism in normal controls was tested for departure from HWE using the χ2 test.
For each stratified factor, the p value and OR (95% CI) were calculated using two-sided χ2 test and logistic regression analysis. First row for “LC patients vs. normal controls,” second row for “GC patients vs. normal controls.”
Table IV shows the main features of the current and previous studies that evaluated the association of -283T>C and the risk of LC or GC (15, 17). According to the inclusion criteria, the study of Lee et al (15) and the current study were finally included in the following meta-analysis to comprehensively assess the association between -283T>C and LC risk. Table V, shows that the frequency of the -283C allele was significantly higher among combined LC patients than combined normal controls (C vs. T: OR = 1.28, 95% CI, 1.06-1.55, p = 0.01), indicating the -283C allele was associated with an increased risk of LC. We also found a significant association between -283CC with the increased risk of LC in 2 genetic models: CC versus TC (OR = 1.29, 95% CI, 1.04-1.59, p = 0.02) and CC versus TC + TT (OR = 1.30, 95% CI, 1.06-1.60, p = 0.01). Therefore, the DNMT3B -283T>C polymorphism might significantly increase the risk of LC in the Asian population.
Characteristics of the current and previous studies
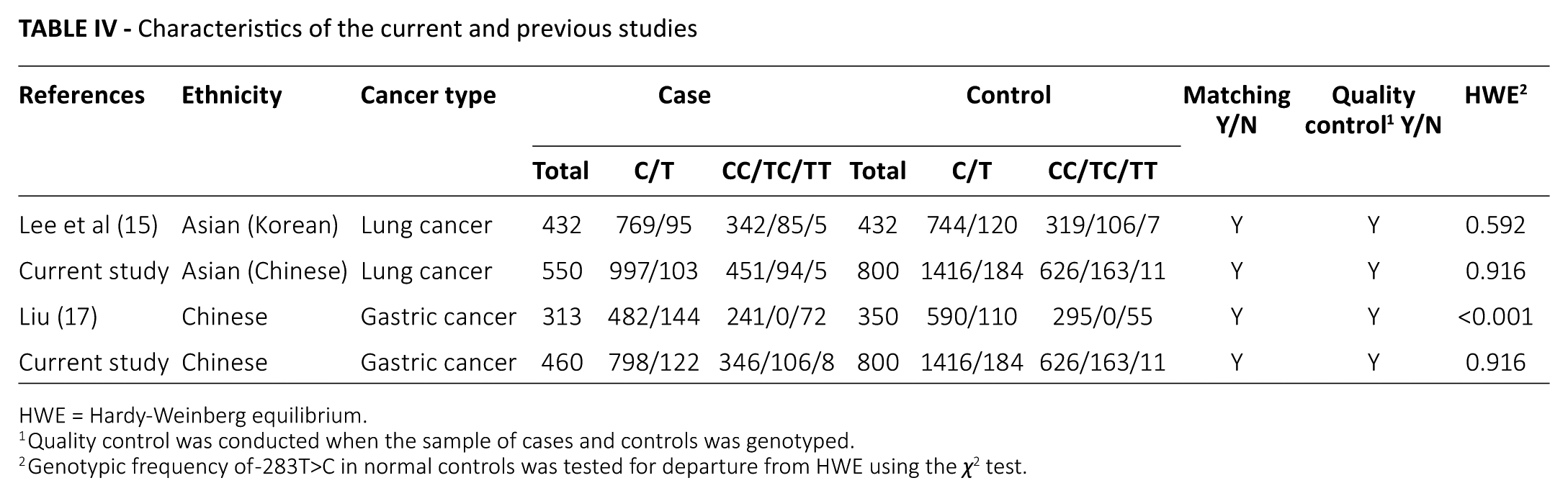
HWE = Hardy-Weinberg equilibrium.
Quality control was conducted when the sample of cases and controls was genotyped.
Genotypic frequency of -283T>C in normal controls was tested for departure from HWE using the χ2 test.
Pooled OR and 95% CI of the association between -283T>C with the risk of lung cancer
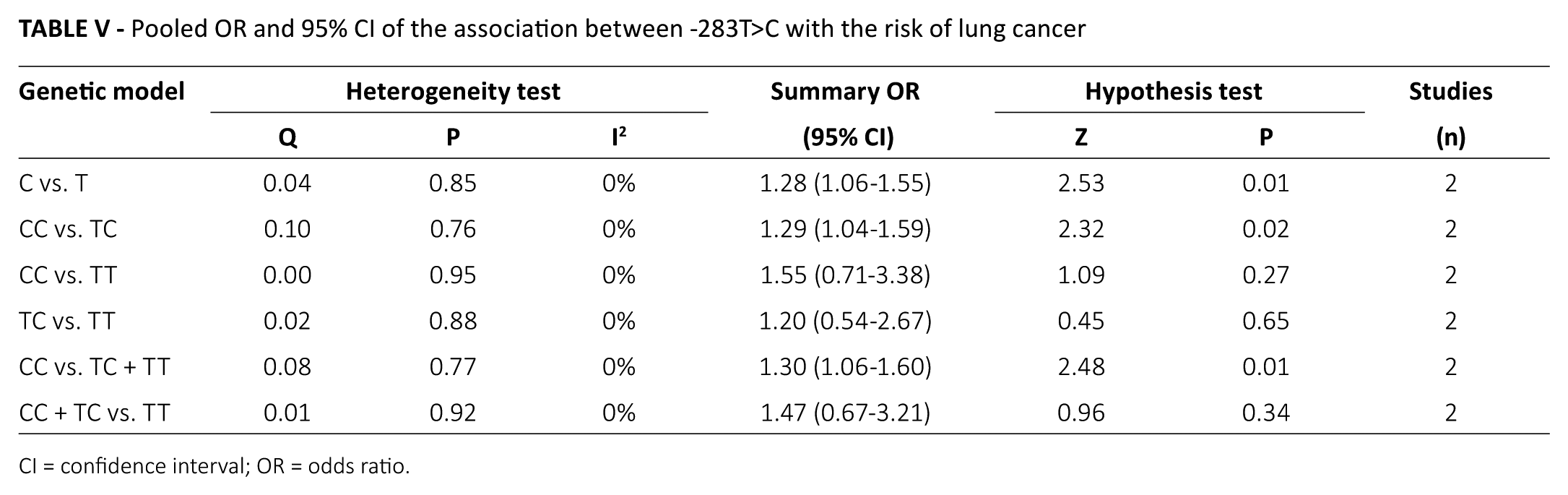
CI = confidence interval; OR = odds ratio.
Discussion
In this case-control study, no significant association was found for -283T>C and the risk of LC in the Chinese population. However, Lee et al (15) found that rs6087990 was significantly associated with LC risk in the Korean population. Specifically, the -283T>C conferred an increased risk of LC (15). This discrepancy might be partially attributed to different environments, lifestyles, and genetic backgrounds among different ethnic populations. Moreover, LC is a heterogeneous and complex disease, which consists of non-small-cell lung cancer (including adenocarcinoma, squamous-cell carcinoma, and large-cell carcinoma) and small-cell lung cancer. Currently, technological advances have enabled the comprehensive analysis of genetic perturbations in LC. It was interesting to observe that the histological subtypes of LC share the driver mutations (e.g., EGFR, KRAS and ALK), but their frequencies of driver mutations are not similar (27, 28). These facts suggest that various histological types of LC may represent different disease entities, which might also contribute to the differences in the results.
In the following meta-analysis, the -283T>C was shown to significantly increase the LC risk in the Asian population, which was consistent with the results of Lee et al (15) in the Korean population, which suggests that a relatively larger sample size might guarantee a significant association between -283T>C and LC in the Chinese population. The interesting question is why the -283T>C polymorphism could affect individuals’ susceptibility to LC. Previously, Lee et al (15) revealed that the -283T allele had a significantly lower promoter activity (~50%) compared with the -283C allele (p<0.001). Therefore, compared with the -283T allele, the -283C allele would lead to the increased expression of DNMT3B, which finally increased LC susceptibility. Collectively, these results explain how the -283T>C affected individuals’ susceptibility to LC and further confirmed an oncogenic role of DNMT3B in LC (11, 29).
Meanwhile, we also showed that there was no significant association of -283T>C and the risk of GC in the Chinese population of Hubei province. Liu (17) had previously performed an association study between -283T>C and the risk of GC in the Chinese population of Jiangsu province. However, in that study, the genotype frequency of -283T>C was not in agreement with HWE in normal controls (p<0.001), which suggests that the enrolled control subjects were not representative. In view of this, a meta-analysis of -283T>C and GC risk was not feasible. Therefore, further confirmatory studies should be undertaken in populations from other regions of China because the present observations only involved the Hubei province Chinese population.
In conclusion, our results demonstrated that the DNMT3B -283T>C polymorphism might be associated with a significantly increased risk of LC in the Asian population, but might not be associated with the risk of GC in the Chinese population. However, additional studies with a larger sample size and in different ethnic populations are needed to confirm or further reinforce our present findings. To evaluate the precise results, studies with gene–environment and gene–gene interactions are essential.
Footnotes
Acknowledgements
The authors thank all the subjects and investigators enrolled in this study.
Disclosures
Financial support: This work was supported by grants from National Natural Science Foundation of China (81502427 and 21404083), and by the Fundamental Research Funds for the Central Universities (WUT: 2017IVA106).
Conflict of interest: None of the authors has financial interest related to this study to disclose.