
Abstract
Background
This study aimed to evaluate the correlation between neutrophil to lymphocyte ratio (NLR) with overall survival (OS) of esophageal squamous cell carcinoma (ESCC) patients.
Method
Records of patients with diagnosed ESCC were reviewed. Leukocyte counts and patients' characteristics were extracted from their clinical records to calculate NLR. Correlation between NLR and baseline characteristics with overall survival (OS) was then analyzed using Cox regression. The patients were then separated into higher and lower NLR groups according to median NLR. OS was further compared between the 2 groups.
Results
A total of 1281 patients were included in the study. Cox regression analysis showed a significant correlation of NLR with OS of ESCC patients. The median pretreatment NLR was identified as 2.86. Higher NLR was associated with worse prognosis in terms of OS.
Conclusions
Pretreatment NLR is independently associated with OS of ESCC patients. Therefore, NLR may be used as a predictive indicator for pretreatment evaluation and adjustment of treatment regimen.
Keywords
Introduction
Esophageal cancer (EC) is a common malignancy, ranking sixth in all cancer death causes worldwide (1) and third in China (2). In 2015, the prevalence rate of EC was estimated to be 477,900, and EC caused 375,000 deaths in China. In Western countries, the major histological type of esophageal cancer is adenocarcinoma (AC), while in China, esophageal squamous cell carcinoma (ESCC) is the dominant type (2). Patients with ESCC usually have a poor prognosis. Despite the various advances in multimodal treatment strategy, the 5-year overall survival rate is still only 15%-25%. To optimize the treatment strategy, it is critical to identify those patients with worse prognosis.
The prognosis of ESCC patients has been reported to be correlated with age, TNM stage, metastasis and tumor locations, as well as various therapeutic methods (3, 4). Currently no gold standard criteria are available for prediction of patients' prognosis or to instruct treatment regimen choices. Therefore, identification of a useful prognostic biomarker would be of great significance in the clinical treatment of ESCC patients.
Recently, it has been proposed that systemic inflammation plays a critical role in cancer tumorigenesis and development (5, 6). Tumor tissue is located in a specific metabolically active and hypoxic microenvironment. In addition, immunological response and inflammation are also important for tumor progression. A general immune-inhibitive environment is induced to protect tumor tissue from the body's immune system defenses. On the other hand, low levels of inflammatory response may help to maintain tumor heterogeneity and induce certain populations of tumor stem cells which are critical for resistance and metastasis of tumor tissue (7). It has been reported that various inflammation markers, such as various cytokines and C-reactive protein, are correlated with prognosis of cancer patients at multiple levels, including treatment response, progression and overall survival (8-11).
Neutrophil to lymphocyte (NLR) ratio is a widely recognized indicator of modified inflammation response (12). It has been reported that NLR is correlated with prognosis of a wide range of patients, including those with lung cancer (13), rectal cancer (14), prostate cancer (12) etc. Since the NLR rate can be calculated from a regular laboratory examination of the clinical records of patients, it has the potential to be used as a practical prognostic biomarker for cancer patients. The cutoff value and predictive value of NLR have been tested in various studies (15, 16). However, in ESCC patients, only a limited number of studies have been carried out to test the correlation of NLR with patients' prognosis (17-19). In addition, due to the differences in ethnic and geographical origins among patients, the predictive value of NLR needs to be tested in different populations. Therefore, the current study aimed to determine the correlation of NLR with overall survival of ESCC patients in China.
Method
Study design and patients
This was a retrospective observational study. Records of consecutive patients with newly diagnosed ESCC in the Department of Thoracic Surgery, Jining No. 1 People's Hospital, from January 2005 to June 2015 were reviewed.
Inclusion criteria included newly diagnosed patients with ESCC confirmed by biopsy, with availability of complete blood cell counts (CBCs) and neutrophil and lymphocyte counts at diagnostic examination.
Exclusion criteria included previous malignancy history, distant metastases, death within 30 days from diagnosis, complication with systemic inflammation disease such as rheumatic conditions or lost follow-up in the first year after discharge.
Baseline characteristics and NLR data were extracted from the clinical records. All NLRs were calculated before patients' treatment. Survival status was collected through phone contact when necessary. The correlation between NLR and baseline characteristics was then analyzed.
The study was approved by the ethics committee of Jining No. 1 People's Hospital. Since the study only involved retrospective review of patients' clinical records, the informed consent form was waived by the committee.
Intervention
The clinical treatment regimens were chosen according to the guidelines for treatment of EC (Chinese version). Most patients underwent esophagectomy surgery with cisplatin plus 5-fluorouracil regimen and/or intensity-modulated radiation therapy (IMRT) as adjuvant therapy or neoadjuvant therapy.
Outcome measurement and data extraction
The study mainly aimed to analyze the correlation between NLR and overall survival of ESCC patients. Overall survival was defined as the time from the day of treatment initiation – whether surgery, chemotherapy or radiotherapy (whichever was carried out first) – until the date of confirmed death. Patients with records of being alive at the last available follow-up were considered as censored data.
Neutrophil and lymphocyte counts at diagnostic examination were extracted from the clinical records. The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count.
In addition, patients' characteristics such as age, sex, tumor staging, carcinoembryonic antigen (CEA), albumin (ALB) and globulin (GLB) were collected from the clinical records.
Follow-up
The patients were regularly followed up every 3 months for the first 18 months through revisits or phone calls after initiation of treatment. After 18 months, patients were followed up every 6 months through phone calls. In some cases, additional follow-up data were collected through a phone call during the study process.
Statistical analysis
SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis in the current study. A 2-sided p value <0.05 was considered to be statistically significant. Continuous data were expressed as means ± standard deviation (SD). Categorical data were expressed as frequency, ratio or percentage. Overall survival of patients was analyzed with Kaplan-Meier survival curves. Univariate and multivariate Cox regression analysis was used to determine the correlations between NLR, as well as baseline characteristics, with overall survival. The log-rank test was used to compare survival between different patient populations.
Results
Baseline demographics and clinical characteristics
A total of 1,281 patients were included in the current study, with 988 men and 293 women. The detailed baseline characteristics of patients are listed in Table I. The surviving ESCC patients at the end of followed-up (survival group) were significantly younger than those who died (deceased group) during follow-up (age 57.7 ± 8.9 vs. 60.2 ± 27.7, p = 0.028). Serum levels of CEA in the survival group were 2.9 ± 2.8 ng/mL, significantly lower than those of the deceased group (3.5 ± 3.5 ng/mL, p = 0.006).
Baseline demographics and clinical characteristics
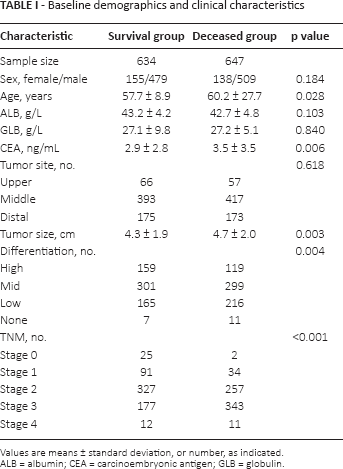
Values are means ± standard deviation, or number, as indicated.
ALB = albumin; CEA = carcinoembryonic antigen; GLB = globulin.
To analyze the relationship between NLR and disease outcome, the patients were chronologically divided into training group (n = 727) and validation group (n = 554). NLRs were calculated among all ESCC patients enrolled. In the training group, NLRs were significantly lower in the survival group (2.4 ± 0.9) than in the deceased group (3.3 ± 1.6, p<0.001). A similar trend was observed in the validation group (p<0.001). In patients overall, NLR was lower in the survival group than in the deceased group (2.4 ± 0.9 vs. 3.4 ± 1.7; Fig. 1).
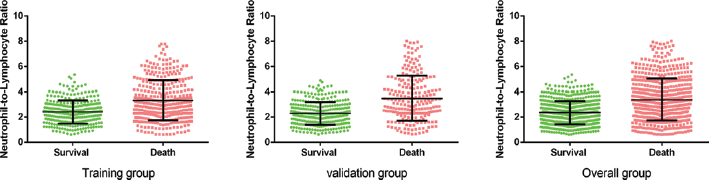
Different neutrophil to lymphocyte ratio (NLR) levels in survival group and deceased group. In the training group, NLRs were significantly lower in the survival group (2.4 ± 0.9) than in the deceased group (3.3 ± 1.6; p<0.001). A similar trend was observed in the validation group with 2.3 ± 0.9 in the survival group, which was lower than the 3.5 ± 1.8 in the deceased group (p<0.001). In overall patients, NLR in the survival group was 2.4 ± 0.9, lower than the 3.4 ± 1.7 in the deceased group.
Factors associated with NLR
The median NLR of patients at diagnostic examination was 2.86. We stratified patients into a low-NLR group (NLR <2.86) and high-NLR group (NLR ≥2.86). The proportions of ESCC patients in each TNM stage were significantly different between those 2 groups. A total of 19 patients were in stage 0, and 79, 337, 251 and 13 in stage 1, 2, 3, 4, respectively, in the low-NLR group. Whereas 8, 43, 211, 223 and 9 patients were in stage 0, 1, 2, 3 and 4, respectively, in the high-NLR group (p = 0.021; Tab. II).
Factors associated with neutrophil to lymphocyte ratio (NLR)
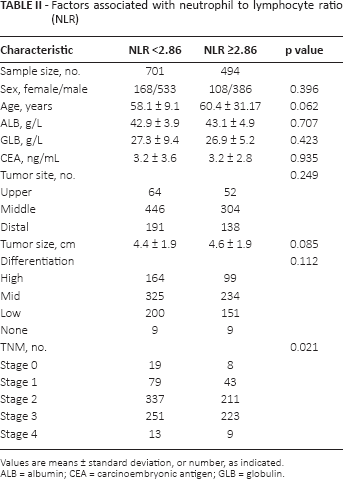
Values are means ± standard deviation, or number, as indicated.
ALB = albumin; CEA = carcinoembryonic antigen; GLB = globulin.
Association of NLR and clinical outcomes
To determine the prognostic impact of NLR on ESCC patients, Kaplan-Meier survival analysis was performed. In the training group, Kaplan-Meier analysis indicated that ESCC patients with high NLR were associated with significantly worse prognosis, in terms of overall survival rate (p<0.001). Consistently, low NLR was positively correlated with favorable overall survival outcome in the validation cohort (p<0.001). In line with the training and validation groups, the results in the overall group indicated that ESCC patients with high NLR were likely to have lower overall survival rates (Fig. 2).
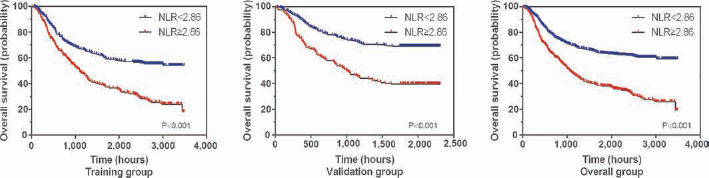
Association of neutrophil to lymphocyte ratio (NLR) and clinical outcomes. In the training group, Kaplan-Meier analysis indicated that esophageal squamous cell carcinoma (ESCC) patients with high NLR had significantly worse prognosis, in terms of overall survival (p<0.001). Consistently, low NLR was positively correlated with favorable overall survival (p<0.001) in the validation cohort. The results in the overall group indicated that ESCC patients with high NLR were likely to have a shorter overall survival.
Stratified survival analyses were conducted to further reveal the prognostic significance of NLR. Data showed that NLR was associated with overall survival in male and female ESCC patients, in ESCC patients with well-moderate and poor-un-differentiated differentiation, and in patients with TNM stage I-II and TNM stage III-IV disease (Supplementary Figure 1, available online at www.biological-markers.com – Stratified survival analyses of prognostic value of NLR).
Analysis of the independent factors for overall survival
Cox regression analysis was used to determine correlations of age, sex, TNM stage, tumor location, differentiation, ALB, GLB, CEA and NLR with overall survival. As shown in Table III, univariate analysis detected age, CEA, tumor size, tumor differentiation, TNM stage and NLR as correlated factors for overall survival. While in multivariate analysis, age (hazard ratio [HR] = 1.002, 95% CI, 1.000-1.005; p = 0.03), CEA (HR = 1.039, 95% CI, 1.013-1.065; p = 0.003), tumor size (HR = 1.057, 95% CI, 1.006-1.111; p = 0.028), TNM staging (HR = 2.172, 95% CI, 1.796-2.628; p<0.001) and NLR (HR = 1.892, 95% CI, 1.567-2.284, p<0.001) were identified as independent factors correlated with overall survival.
Analysis of independent factors for overall survival
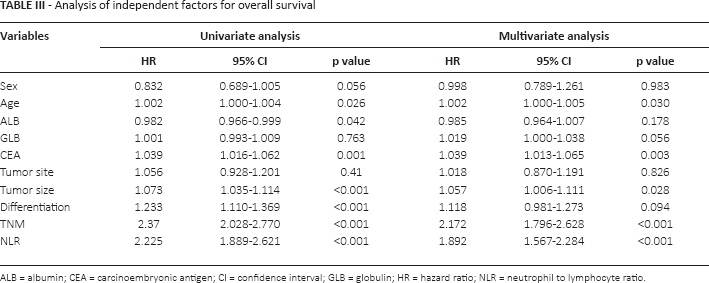
ALB = albumin; CEA = carcinoembryonic antigen; CI = confidence interval; GLB = globulin; HR = hazard ratio; NLR = neutrophil to lymphocyte ratio
In addition, a receiver operator characteristic (ROC) curve analysis was conducted to verify the prognostic and predictive capability of NLR (Supplementary Figure 2, available online at www.biological-markers.com – ROC curve analysis to verify the prognostic value of NLR). The results indicated that the area under ROC curve was 0.687 (95% CI, 0.656-0.717; p<0.001), the sensitivity was 54.2% and the specificity was 74.3%, when the NLR cutoff value was set to >2.91.
Discussion
The results of the current study showed that in patients diagnosed with ESCC in our center, the overall survival was associated with NLR, as well as with other recognized risk factors including age and TNM stage. Patients with higher pretreatment NLR had worse prognosis in terms of overall survival compared with those with lower NLR. These results demonstrated that NLR may be used as a prognostic predictor for ESCC and a potential target for therapy development.
ESCC is the major type of esophageal cancer in China. This histological type accounts for more than 80% of EC patients there. To avoid bias, the study only included ESCC patients. Whether NLR is associated with overall survival in EC patients of other histological types was beyond the scope of the current study and needs to be further addressed.
ESCC has much a greater prevalence in the male population than in the female population, especially in China (2). Differences in smoking habits may account for the imbalanced morbidity in the different sexes. In the current study, men accounted for about 77% of the total study subjects. This proportion is consistent with previous studies of ESCC in a Chinese population (19, 20). In the current study, sex was not identified as an independent factor correlated with overall survival of ESCC. This may be due to the relatively small sample size and inefficient female patient sample size. Therefore, the impact of the sex of a patient on overall survival with ESCC needs to be further confirmed in future studies. In addition, patients' characteristics such as the distribution of cancer stages, tumor location and differentiation status were all consistent with previous studies. These results indicate that the general clinical features of Chinese ESCC patients in different regions might not be significantly different. Therefore, the results of this study may be used as a reference in other similar studies in ESCC patients of China.
There is a strong linkage between cancer and inflammation (9, 21, 22). Inflammation can not only affect the outcome of a series of diseases, but can also affect the occurrence and development of tumors (23-26). Serum markers including neutrophils, platelets and lymphocytes and others derived from the peripheral blood have been proven to be significantly associated with a series of diseases and tumor progression (27-30). Some indicators such as the systemic immune-inflammation index (SII) and platelet to lymphocyte ratio (PLR) have emerged as prognostic factors in many cancers, including ESCC (31, 32). In the current study, we revealed that pretreatment NLR was significantly associated with prognosis of ESCC. How to combine these inflammatory parameters into 1 equation to provide more accurate prognostic predictions for ESCC requires further study.
NLR has been reported to be correlated with patients' prognosis in different cancer studies. It has been reported that the pretreatment median NLR ranged from about 1.5 to 3.3 (13, 14, 33). For example, it has been reported that a median preoperative NLR of 2.1 was of significant prognostic value for disease-specific mortality in ESCC patients who underwent surgery (34). In various cancer patients, it has been shown that NLR cutoffs ranging from 1.9 to 4.2 were of significant predictive value for treatment responses (12, 18, 35). In the current study, the median pretreatment NLR in ESCC patients was estimated to be 2.3. This result is consistent with previous studies. Various studies in different patient populations have identified a relatively small variation in pretreatment NLR. These results indicate that NLR may be a stable characteristic and therefore may have practical value in prognostic prediction of patients' outcome.
The current study had some limitations. Firstly, this was a relatively small sample size retrospective study with limited statistical power. Due to considerations of data intactness, only overall survival, and not progression-free survival or other patient outcomes, was analyzed. Also, some other baseline characteristics, variations in therapy regimens, as well as interactions between variables may have caused bias in the results. Despite this, the results indicated that NLR has a high probability to be useful as a predictive marker for the prognosis of ESCC patients.
In conclusion, results from the current study showed that pretreatment NLR was independently associated with overall survival of ESCC patients. Therefore, NLR may be used as a predictive indicator for the pretreatment evaluation and adjustment of treatment regimen.
Footnotes
Financial support: None.
Conflict of interest: The authors declare they have no conflict of interest.