
Abstract
Purpose
To describe a minimally invasive method to create multifocal full-thickness surgical iridectomy biopsies.
Methods
Seven patients suspected to have diffuse iris melanoma underwent multifocal surgical iridectomy biopsy through a single 1.0-mm clear corneal incision. A 25-G inked trocar was used to create one visible corneal portal, through which the anterior chamber was filled with sodium hyaluronate 1%. Then, a 25-G aspiration cutter probe was introduced through the corneal incision such that the aspiration portal was occluded by the iris biopsy sites. Then aspiration (600 mm Hg) cutting (300 cuts per minute) was used to create full- and partial-thickness surgical iridectomy biopsies at multiple locations. After each biopsy the probe was removed, and its contents aspirated into a separate 3-mL syringe (marked by clock hour location). The sodium hyaluronate 1% was removed and wound checked for leakage.
Results
Diagnostic specimens were obtained in all cases. Five were found to be diffuse iris melanomas and 2 were indeterminate iris melanocytic proliferations. No patients developed a secondary increase in intraocular pressure, hyphema, infection, cataract, or vision loss. No cases of intraocular tumor dissemination were observed. No patient complained of glare or monocular diplopia. Three of 7 corneal wounds were self-sealing.
Conclusions
Multifocal surgical iridectomy biopsy can be minimally invasive and effective allowing for partial- and full-thickness iris biopsy. Use of a 25-G aspiration cutting probe allowed for small incision surgery, rapid rehabilitation, and no significant complications.
Introduction
Biopsy-proven iris melanomas have been found to carry a 10.7% risk for metastasis (1–2–3). Thus a safe method of iris tumor biopsy is needed. Anterior uveal tumors are accessible for biopsy, cytologic, histopathologic molecular and genetic evaluation (4–5–6). Specimens can be obtained by fine-needle aspiration biopsy, wide-incision surgical iridectomy, or aspiration cutter techniques (7–8–9–10–11). Fine-needle aspiration biopsy typically involves placing a 25 gauge sharp needle tip (4 mm long, 0.8 mm wide) through the cornea and aqueous, then into or onto the iris tumor. Scraping the tumor liberates cells that are manually aspirated by an assistant through extension tubing. However, piercing or partially embedding a sharp-edged (4 mm long, 0.8 mm wide) needle tip into a 0.8-mm-thick iris risks lacerating the lens, iris blood vessels, and ciliary body. Though typically self-limited, secondary fine-needle aspiration biopsy-related hyphemas are common (9).
In contrast, surgical iridectomy biopsy yields the best tissue for histopathology and immunohistopathologic analysis (12, 13). However, surgical iridectomy or biopsy involves dissection of a relatively large surgical corneal or scleral wound. After the iridectomy, this wound must be sutured, risking astigmatism, glare, and the need for subsequent rehabilitation (13, 14). Surgical iridectomy biopsy for diffuse or multifocal iris melanoma would require an open-sky, penetrating keratotomy.
Herein, we describe a technique for minimally invasive, multifocal, aspiration cutter-assisted iris biopsy. This is a variation of the Finger iridectomy technique (FIT) that has been shown to offer cells for cytology (like fine-needle aspiration biopsy) as well as small pieces that can be evaluated by histopathology and immunohistochemistry (like surgical iridectomy biopsy) (11). Unlike our prior reports, this study describes its use to diagnose diffuse anterior uveal tumors by obtaining multifocal iris biopsies through a single corneal incision.
Methods
Privacy and informed consent
Each patient signed treatment consent and Health Insurance Portability and Accountability Act of 1996 forms. Observation, biopsy, and treatment were discussed as indicated. When biopsy was planned, the risks and potential benefits of fine-needle aspiration biopsy and incisional and multifocal aspiration cutter biopsy techniques were also discussed. This research conforms to the tenets of the Declaration of Helsinki and internal review board approval was obtained from The New York Eye Cancer Center.
Surgical preparation
Each patient was medically cleared for anesthesia. One hour prior to surgery, the eye was treated with topical pilocarpine hydrochloride 1%, timolol maleate 0.5% and the patients given PO acetazolamide 500 mg. Once in the operating room, the patient's face and eye were prepped with an iodine-based topical antibiotic.
Multifocal FIT
An eyelid speculum was placed and the operating microscope adjusted to maximally visualize the anterior segment. Then a 0.3 forceps was used to stabilize the eye at the limbus. An inked 25-G trocar was then used to create a blue, visible, and shelved incision through clear juxtalimbal cornea. Though it penetrated the anterior chamber, the clear corneal incision guaranteed that any liberated cancer cells would exit the patient's body. Incisions were typically made at a position on the most superior 90 degrees of the cornea. Sodium hyaluronate 1% (Healon, Advanced Medical Optics, Santa Ana, CA, USA) was used to fill the anterior chamber and served to maintain the anterior chamber depth and position the iris tumor for biopsy.
The saline infusion line was disabled. Then an unprimed, 25-G aspiration biopsy cannula (probe) was inserted into the anterior chamber (Fig. 1). By rotating the probe along the axis of the corneal incision, we were able to access multiple iris locations. By rotating the probe along its central axis, the aspiration cutting portal was brought in contact with the iris or tumor for biopsy. Thus multiple iris biopsies were performed through a solitary corneal entry (Fig. 2).
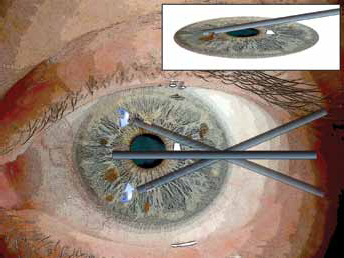
(Left) Rotation of the probe along the axis of the corneal incision allowed access to all the iridectomy biopsies demonstrated in Figure 2. (Right) Rotation of the aspiration cutter allowed controlled engagement and biopsy of the iris and iris tumors. (Robert Masini, NYC, NY, USA, artist)
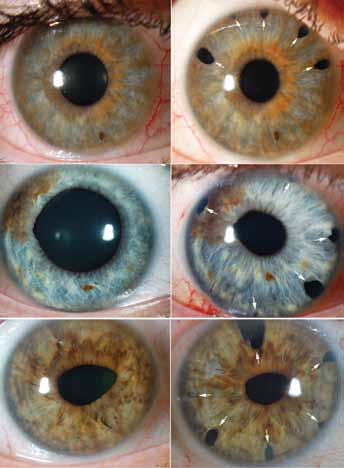
(Top) Case 3 shows multiple iris biopsies primarily along the superior aspect of the diffusely hyperpigmented, heterochromic iris (arrows). (Middle) Case 5 shows multifocal pigmented iris lesions through which biopsies were obtained (arrows). The retained 10-0 nylon corneal suture can be seen at 7:30. (Bottom) Case 6 was noted to have new-onset heterochromia, biopsied in each quadrant to diagnose diffuse iris melanoma (arrows).
During biopsy, the aspiration port was rotated so as to be occluded by visible tumor or iris. With the surgeon modulating, machine-assisted aspiration and cutting was performed. The settings were started on suction of 300 mm Hg and a cutting rate of 600 cuts per minute. These settings were then adjusted so as to maximize the efficiency of the process under direct visualization, while trying to keep the cut rate as low as possible.
Biopsies were mostly full-thickness iris; however, partial-thickness tumor biopsies were also achieved (Fig. 2). Each time the cutter was removed from the eye, an empty 3-mL syringe was attached to the effluent connector. Then the cutter portal was placed in saline solution and the aspirate flushed from the effluent tumor into the syringe (approximately 0.5 mL of saline). Full-thickness biopsies typically yielded pieces that could be visualized by looking at the syringe beneath the operating microscope. Then each receptacle syringe was marked according to the clock hours(s) from which the specimen was taken. The aspiration cutter was flushed (cleaned) with saline between each iris biopsy.
Upon completion of specimen collection, all syringes were immediately sent to pathology for cytologic evaluation. Then the residual sodium hyaluronate 1% was removed from the eye by manual aspiration irrigation and replaced by balanced salt solution. The corneal wounds were checked by Seidel test. If leakage was noted, the wounds were closed with a single 10-0 nylon suture (Ethicon, Somerville, NJ, USA). At the end of surgery, an antibiotic-steroid solution was injected beneath the conjunctiva and antibiotic-steroid ointment was placed on the eye. Due to sedation, the operative eye was temporarily patched and shielded. Patients were discharged (same day) on topical steroid, antibiotic, and agents to maintain intraocular pressure control. Our methods of cytopathology, histopathology, and immunopathology have been described (7, 11, 15). Genetic expression profiling was employed in one case (16, 17).
Results
Since 2009, 7 irises suspicious for containing diffuse, multifocal iris melanoma were biopsied (Tab. I). Diagnostic specimens were obtained in all cases. Five were found to be diffuse iris melanomas and 2 were indeterminate iris melanocytic proliferations. This minimally invasive iridectomy technique was found capable of yielding adequate specimens for evaluation in all cases. The mean number of iris biopsy sites was 5. Four of 7 cases (57%) required a 10-0 nylon suture to close the wound (Tab. II). A specimen was obtained in all cases and allowed for immunopathology in the 2 cases of indeterminate melanocytic tumors (Tab. II).
Patient and tumor characteristics
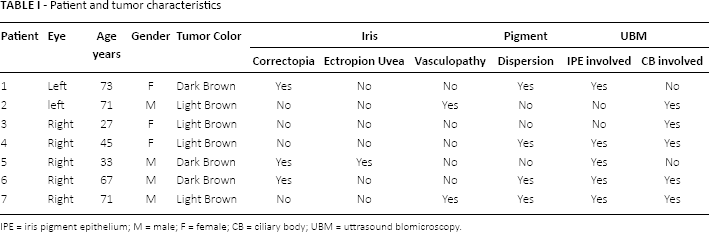
IPE = iris pigment epithelium; M = male; F = female; CB = ciliary body; UBM = uttrasound blomicroscopy.
Multfocal Iris biopsy results
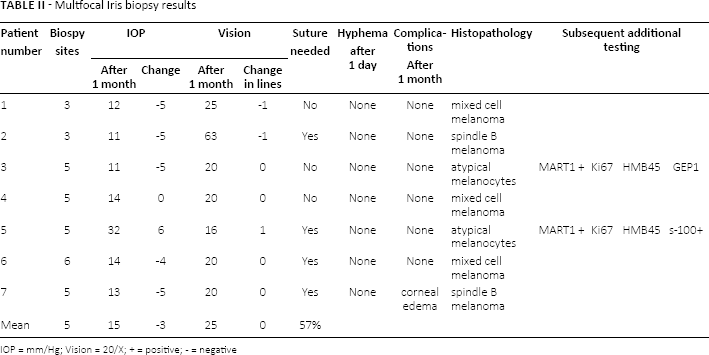
IOP = mm/Hg; Vision = 20/X; + = positive; - = negative
No patient developed a transient postoperative intraocular pressure spike related to the sodium hyaluronate 1%. In all but 2 cases, there was a reduction of intraocular pressure (mean 2, mode 5 mm Hg) 1 month after biopsy (Tab. II). Patient 5 exhibited an intraocular pressure rise of 12 mm Hg. However, he had tumor pigment dispersion-associated glaucoma prior to iris biopsy.
One month after surgery, all visual acuity measurements were within 1 Early Treatment Diabetic Retinopathy Study line of vision compared to that measured prior to treatment (Tab. II). No patients experienced post-biopsy glare or diplopia. While 1 patient developed transient corneal edema, no long-term complications could be related to the multifocal FIT (MFIT) technique.
Case examples
Case 3
A 27-year-old woman was referred to The New York Eye Cancer Center with a history of increasing pigmentation of the right iris. Ophthalmic examination revealed blue irides with heterochromia and no ectropion uvea, corectopia, or vasculopathy (Fig. 2, top). Her vision was 20/20, intraocular pressure was 16 mm Hg, and slit-lamp revealed 1+ flare without cell. While gonioscopy revealed no tumor in the angle, 35 MHz high-frequency ultrasound imaging revealed diffuse uveal (iris and ciliary body) thickening without angle blunting. The posterior vitreous face was hyperechoic. The posterior segments also displayed heterochromia consistent with ocular melanosis. In consideration of her ocular inflammation, a uveitis consultation was negative. Biopsy was performed (Fig. 2, top).
Case 5
A 33-year-old man was referred to The New York Eye Cancer Center for evaluation of an iris tumor and secondary glaucoma. Ophthalmic examination revealed a blue iris, a brown tumor, multiple smaller iris nevi, as well as mild ectropion uvea and corectopia (Fig. 2, middle). Bilateral gonioscopy revealed asymmetric hyperpigmentation involving the iris stroma and angle stuctures. High-frequency ultrasound imaging (35 MHz) revealed both atrophy and thickening of the ciliary body as well as generalized disruption of the iris pigment epithelium. A biopsy was performed (Fig. 2, middle).
Case 6
A 67-year-old man was referred to The New York Eye Cancer Center for diffusely increased pigmentation of the iris (heterochromia), ciliary body, and corneal endothelium (Fig. 2, bottom). There was marked corectopia without ectropion uvea or visible anterior uveal neovascularization. High-frequency ultrasound imaging (35 MHz) revealed focal thickening of the iris and ciliary body as well as iris pigment epithelial disruption. Biopsy was performed (2, bottom).
Pathology
Case 3 is shown as a representative example (Fig. 3). Here we see that in addition to cells, relatively large pieces of tissue were obtained. A review of the detailed characteristics of each specimen, descriptions of each patient's treatment, and outcomes are beyond the scope of this report.
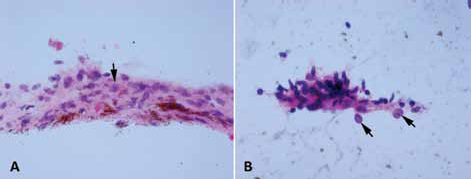
Representative pathology. This specimen from Case 3 shows single cells and iris tissue fragments with a diffuse melanocytic proliferation. Most melanocytes demonstrate bland spindle nuclei with fine chromatin and inconspicuous nucleoli. Occasional melanocytes (arrows) have ovoid nuclei with central nucleoli and margination of nuclear chromatin, suspicious for spindle cell melanoma. (
Complications
In this series, postoperative evaluations have revealed no wound leaks, hyphema, endophthalmitis, or cataract. These findings have largely been attributed to our use of a small incision, lack of surgical irrigation, and the size of this series. All surgeries were performed in the ambulatory setting. Patients were re-examined at least within 24 hours, 1 week, and 1 month after surgery. In this series, the melanomas were treated with a radioactive plaque and the indeterminate lesions have been observed at 5 and 3 years, respectively.
Discussion
Tumor size and ciliary body involvement are 2 evidence-based characteristics suggesting that diffuse iris melanomas may be particularly lethal (1, 2, 14, 18, 19). Often presenting as unilateral glaucoma, these tumors have been diagnosed after enucleation or (more recently) treated with glaucoma stents or tubes (20). It is reasonable to assume that a simple, relatively noninvasive method to diagnose diffuse iris melanoma can allow for newly reported vision- and eye-sparing anterior segment radiation therapy (21, 22).
This study demonstrates that multifocal iris biopsies can be performed through a solitary sub-millimeter clear corneal incision utilizing a 25-G aspiration cutter. No patient lost visual acuity, developed biopsy-related glaucoma, or had hyphema. In fact, 75% of patients showed reduced intraocular pressure (Tab. II). This technique has been found particularly helpful for the diagnosis of diffuse, multifocal iris melanoma. In this series, a pathologic diagnosis was achieved in all cases.
Unlike transscleral or transvitreal biopsy of posterior segment tumors, a transcorneal biopsy approach obviates any risk of subconjunctival tumor seeding. As compared to fine-needle aspiration biopsy, where cells are aspirated through a sharp needle, extension tubing, and into a 5- or 10-mL syringe, our technique uses a blunt aspiration cutter, machine-controlled aspiration, and cutting. In this series shows, as does our prior published experience, MFIT is associated with minimal risk of secondary hyphema and its sequelae. However, should hemorrhage occur, the aspiration cutter can be used to evacuate blood.
However, we must consider that the use of a single 25-G aspiration cutter for multiple biopsies is not perfect. Though the aspiration cutter was irrigated between biopsies, there exists the possibility of retained cells migrated to slides of subsequent biopsy sites. Though the viscoelastic was removed at the end of the procedure, there exists a risk of postoperative glaucoma in eyes at risk. Finally, unlike standard iridectomy or iridocyclectomy, MFIT yields less tissue for histopathologic evaluation of local invasion.
Vitreous cutters have also been employed to perform iridectomy for tumor biopsy and treatment for narrow angle glaucoma (23) Ghanem et al (5) used a cutter during phacoemulsification in patients with iridoschisis. Fastenberg et al (24) and Bechrakis et al (25) used a vitreous cutter-based system for biopsy of indeterminate intraocular tumors (some of which were located in the iris).
The MFIT is different from that described by these authors. It utilizes a single 25-G aspiration cutter probe to perform multiple iridectomy biopsies through a single 1-mm incision (under sodium hyaluronate 1%). Unlike the Ghanem technique, there is no scleral phacoemulsification incision or irrigation. Similarly, Bechrakis et al (24) employed a relatively large aspiration cutter (20-G) and a 21-G infusion cannula (to maintain anterior chamber depth). These corneal incisions were reported to require closure with 10-0 nylon sutures. Clearly, irrigation can make harvesting iris tumor fragments more difficult.
Herein, we report on the use of a 25-G aspiration cutter to perform minimally invasive biopsy of diffuse melanocytic iris tumors through a solitary 1-mm incision.