
Abstract
Purpose:
To investigate the safety and tolerability of total anterior segment palladium-103 (103Pd) eye plaque brachytherapy for multifocal iris melanoma.
Methods:
Interventional case series of 11 patients with multifocal iris melanomas. Anterior segment ultrasound revealed tumor size, location, and intraocular margins. Epicorneal amniotic membrane grafts protected the cornea and decreased pain during total anterior segment 103-Pd ophthalmic plaque brachytherapy.
Results:
Eleven diffuse iris melanomas were American Joint Committee on Cancer 8th edition–classified as T1 (n = 5, 45.5%) and T2 (n = 6, 54.5%). Plaque radiation was completed to a minimum mean tumor dose of 85 Gy (mean dose rate, 58.1 cGy/h). Ultrasonographic tumor thickness regression was 41% (follow up mean 58.7, median 50, range: 8–139 months). Despite 100% local control and 100% eye retention, one patient (9.1%) developed metastatic disease. Four eyes required cataract surgery. There was no corneal stem-cell deficiency, corneal opacity, radiation maculopathy, or optic neuropathy. While visual acuity prior to treatment was 20/40 or better in 10 (91%), 9 were 20/40 or better (81.9%) at last follow-up. Four (36%) had glaucoma prior to treatment and three eyes developed glaucoma after treatment for a total of 63%.
Conclusion:
Total anterior segment (103Pd) plaque brachytherapy resulted in local control, good visual acuity, eye and life preservation in the treatment of multifocal iris melanoma.
Introduction
Melanoma is the most common primary iris malignancy. 1 However, it is also the least common uveal melanoma. 1 Furthermore, multifocal iris melanoma, also called the diffuse-multifocal variant, is even less common.2,3 Such melanomas have been described as flat, infiltrating, or seeding through the anterior chamber. 3 Overall, metastatic rates of biopsy-proven iris melanomas range from 3% to 13% based on tumor size and ciliary body involvement.2–4
Iris melanoma treatments include local surgical excision, radiation therapy, and enucleation.1–11 While the primary goal is removal or destruction of the tumor, the evolving trends have been toward eye and vision preservation. Treatment depends on tumor size and location. Small well-circumscribed lesions have been treated with sector iridectomy or iridocyclectomy. Larger non-resectable melanomas are more likely managed with irradiation or enucleation.4–9
In 1952, Lloyd and Ellis 10 inserted radioactive tantalum wires into the eye to treat small iris melanoma as an alternative to enucleation. Since that report, multiple forms of episcleral radioactive plaque or external beam radiation therapy have evolved.6–9 Radiation has been found to be an eye- and vision-sparing alternative to resection and enucleation.
The use of externally applied radiation (plaque or proton) for iris melanoma circumvents risks associated with intraocular surgery (e.g. lens subluxation, hypotony, retinal detachment, endophthalmitis, phthisis, and sympathetic ophthalmia).5,12,13 In contrast, and dependent upon modality, radiation complications may include eye lash loss, dry eye, corneal opacity, iris neovascularization, and cataract. Side-effects have been related to each type of radiations’ dose rate and dose distribution.14,15 In general, anterior segment radiation allows for larger treatment margins compared to resection.16,17
Until recently, multifocal iris melanoma was treated with enucleation. 16 Often invading the angle and/or ciliary body, total anterior segment (including the ciliary body) irradiation has been required to treat the entire tumor.16–18
In a single case, total anterior segment 103Pd plaque radiation therapy was well tolerated by a patient who refused enucleation. 16 Since then, amniotic membranes have been used to buffer epicorneal plaque therapy, improve patient comfort, and protect the cornea.19,20 Herein, we present the first clinical case series of patients with multifocal iris melanoma treated by total anterior segment 103Pd plaque radiation therapy. It includes our experience with long-term safety as well as local and systemic cancer control.
Methods and materials
Patient privacy and informed consent
This study adhered to the tenets of the Declaration of Helsinki revised in 2000, the Health Insurance Portability and Accountability Act of 1996. It was approved by the institutional review board of the New York Eye Cancer Center. Informed consent included a detailed discussion of risks and potential benefits of enucleation and total anterior segment radiation therapy. The risks of the latter included the potential for corneal and scleral melting, limbal stem-cell deficiency, cataract, glaucoma, and anterior segment ischemia. Based on the literature, patients were informed that total 103Pd anterior segment plaque was unlikely to affect their macular retina or optic nerve. 21 Each patient gave written consent to have their findings and images published.
This series is a retrospective clinical study of 11 eyes of 11 consecutive patients with multifocal iris melanoma diagnosed by clinical examination and pathology.
Clinical diagnosis
Each patient provided a detailed medical history and was evaluated by best-corrected visual acuity (BCVA), pupillary, ocular motor examination, slit-lamp biomicroscopy, and intraocular pressure (IOP) measurements. Slit-lamp and gonioscopic photography were performed. Ophthalmoscopy with direct, indirect, and contact lens techniques were utilized. Cataract assessment was performed for phakic patients.
Each melanoma was assessed for intrinsic vascularity, pigment dispersion, corectopia, ectropion uveae, ciliary body invasion, and extraocular extension. Each was classified according to the 8th edition of the American Joint Committee on Cancer (AJCC) classification (Table 1). 4 The tumor base was measured in two perpendicular dimensions. The circumferential extent in the iris was measured by chord (mm) and number of clock hours of involvement and was determined by slit-lamp biomicroscopy, scleral transillumination (for ciliary body component of iridociliary melanoma), and ultrasonography. High-frequency ultrasonography biomicroscopy (UBM) was helpful for determining tumor height (apex), margins as well as interstitial iris and ciliary body extent (compared to normative values). 22 UBM was used to monitor tumors after plaque brachytherapy. 23 Examinations focused on angle blunting, ciliary body thickening, and retro-iridal tumor extension. 23 The clinical diagnosis was confirmed with pathology utilizing our multifocal iris biopsy technique. 24
Demographic and multifocal iris melanoma characteristics.
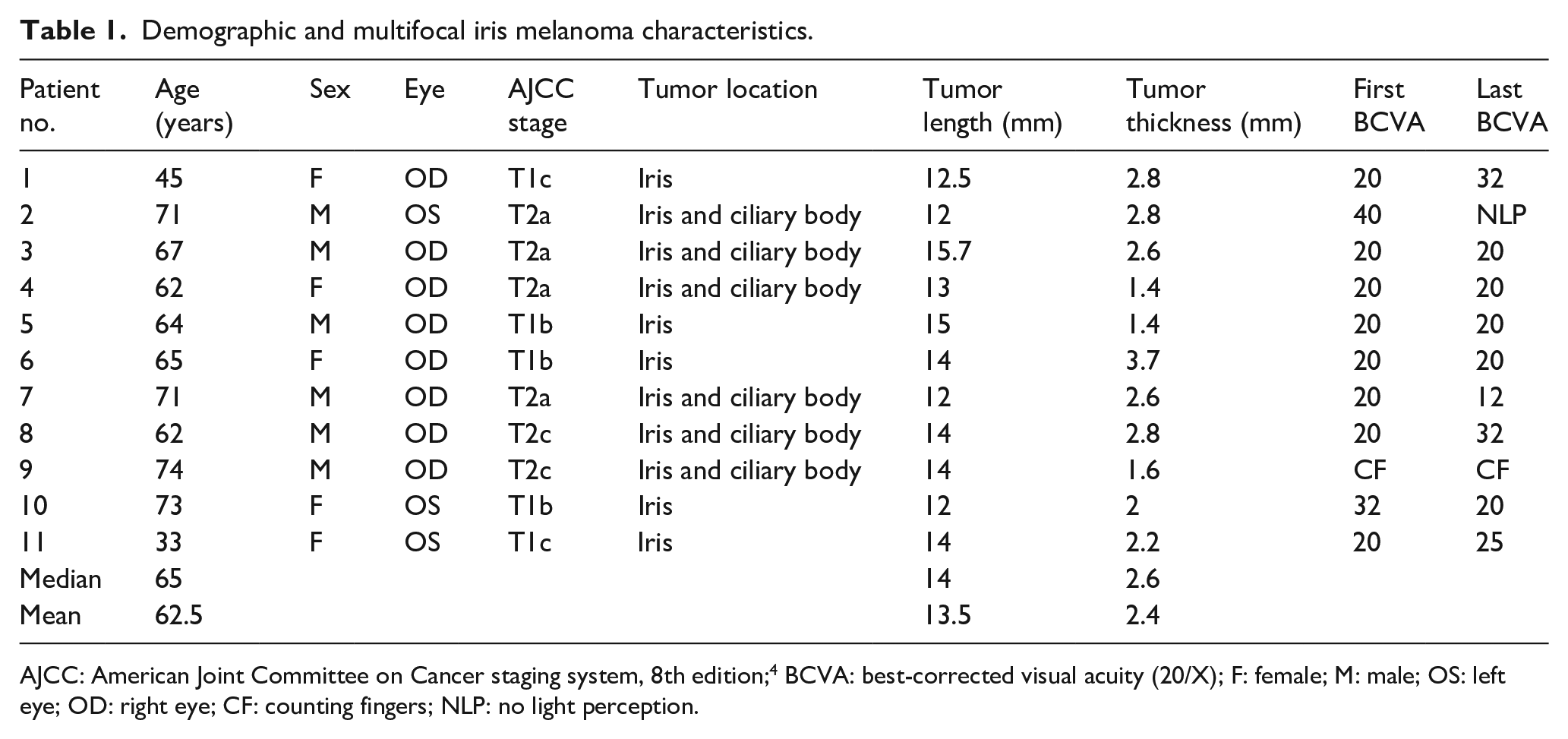
AJCC: American Joint Committee on Cancer staging system, 8th edition; 4 BCVA: best-corrected visual acuity (20/X); F: female; M: male; OS: left eye; OD: right eye; CF: counting fingers; NLP: no light perception.
Iris biopsy technique
Multifocal biopsy was performed in 10 eyes (90.9%) through a solitary sub-millimeter clear corneal incision utilizing an aspiration cutter using the Finger Iridectomy Technique (FIT).24,25 The transcorneal biopsy approach obviated any risk of subconjunctival tumor seeding. The diagnosis of multifocal melanoma was confirmed by histopathological analysis.
Metastatic workup
Metastatic surveys were performed prior to treatment and every 6 months thereafter. Pre-treatment staging involved whole-body 18-flourodeoxyglucose positron emission tomography computed tomography (PET-CT).26,27 Subse-quently, radiographic surveillance was performed utilizing computed axial tomography or magnetic resonance imaging of the abdomen.1,4,28
Radiation parameters
According to the American Brachytherapy Society 2014 consensus guidelines, comparative dosimetry was performed for each patient prior to radionuclide selection.28,29 In each case, the 103Pd radionuclide (vs 125I) was selected due to a more favorable intraocular radiation distribution to critical structures. 103Pd resulted in less radiation to the macula, optic disk, and opposite eye wall (Tables 2 and 3). 103Pd seeds (model 200) were employed at strengths up to 2 mCi (Theragenics Corporation, Buford, Georgia). Radiation data included the following: plaque diameter, number of radioactive seeds, duration of treatment, prescribed radiation dose (Gy), and dose-rate (cGy/h) to tumor apex, inner cornea, lens, optic disk, fovea, and optic disk (Table 2).
Calculated 103Pd radiation dose to intraocular structures and side-effects.
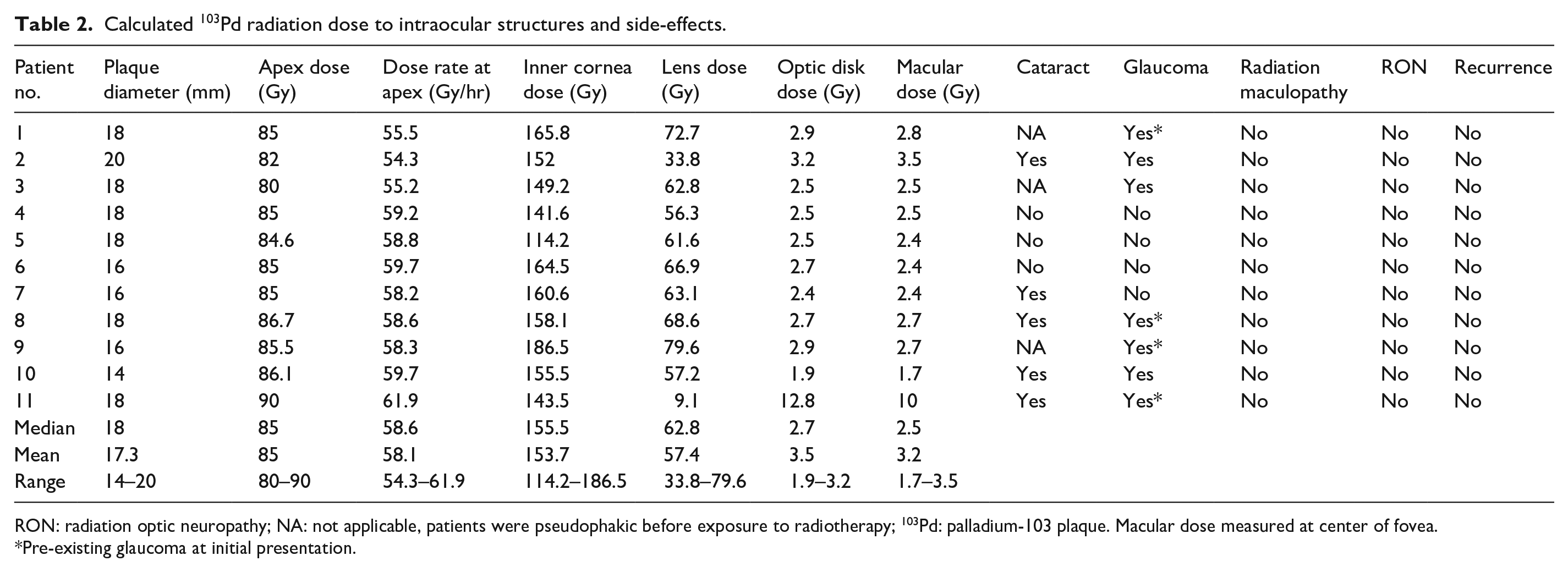
RON: radiation optic neuropathy; NA: not applicable, patients were pseudophakic before exposure to radiotherapy; 103Pd: palladium-103 plaque. Macular dose measured at center of fovea.
Pre-existing glaucoma at initial presentation.
Comparative intraocular radiation distribution (103Pd vs 125I vs 106Ru) in this series.
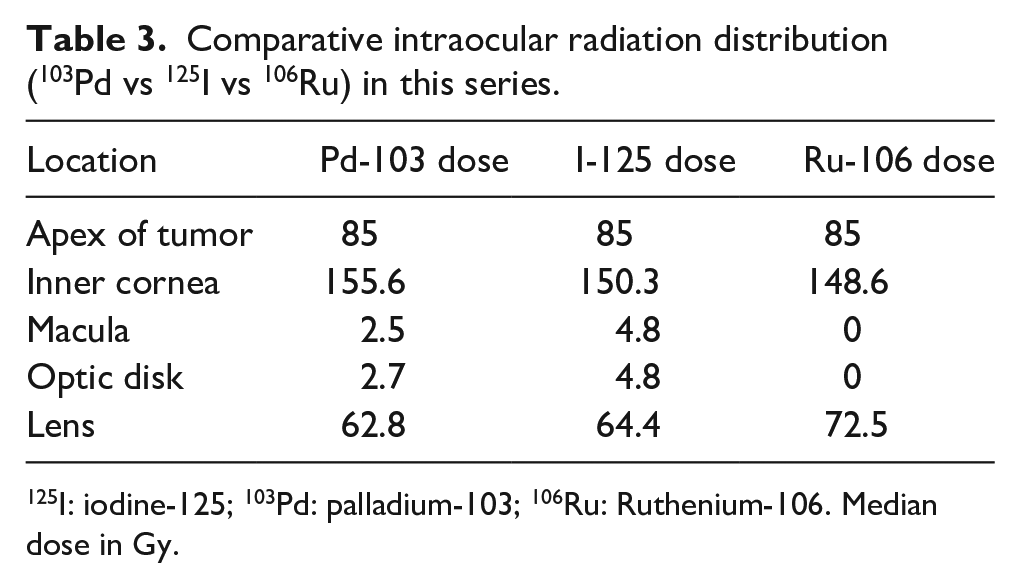
125I: iodine-125; 103Pd: palladium-103; 106Ru: Ruthenium-106. Median dose in Gy.
Plaque insertion technique
Tumor localization was dependent upon pre-operative UBM imaging measurements and tumor-mapping. Imaging and measurements included the entire anterior segment, ciliary body to ciliary body (360° ) as compared to normative values.22,23 Each plaque was placed as to cover the entire anterior segment plus a 2–3 mm margin to include the ciliary body and pars plana within the target zone. No tumors extended beyond the pars plana.
At surgery, a 360° conjunctival peritomy was performed, and Tenons’ fascia was opened in each quadrant. Epicorneal atropisol 1% (Iolab, Claremont, CA, US) was placed to stabilize the iris tumor position during brachytherapy. 30 A tissue marking pen was used to mark a 360° circle, equivalent to the plaque diameter on the sclera to define the target zone (Figure 1). Then a 20 × 25 amniotic membrane was placed over the cornea and sewn to sclera to buffer the gold plaque and seeds.19,20 The plaque was placed over the amniotic membrane (suture eyelets temporal), aligned with the prior episcleral marks and sewn to sclera. The anterior aspect of the plaque was covered by a Gunderson flap closed with a running 6-0 Vicryl suture (Figure 1). Antibiotic-steroid was placed at the end of surgery and then four times daily during the 7-day treatment.
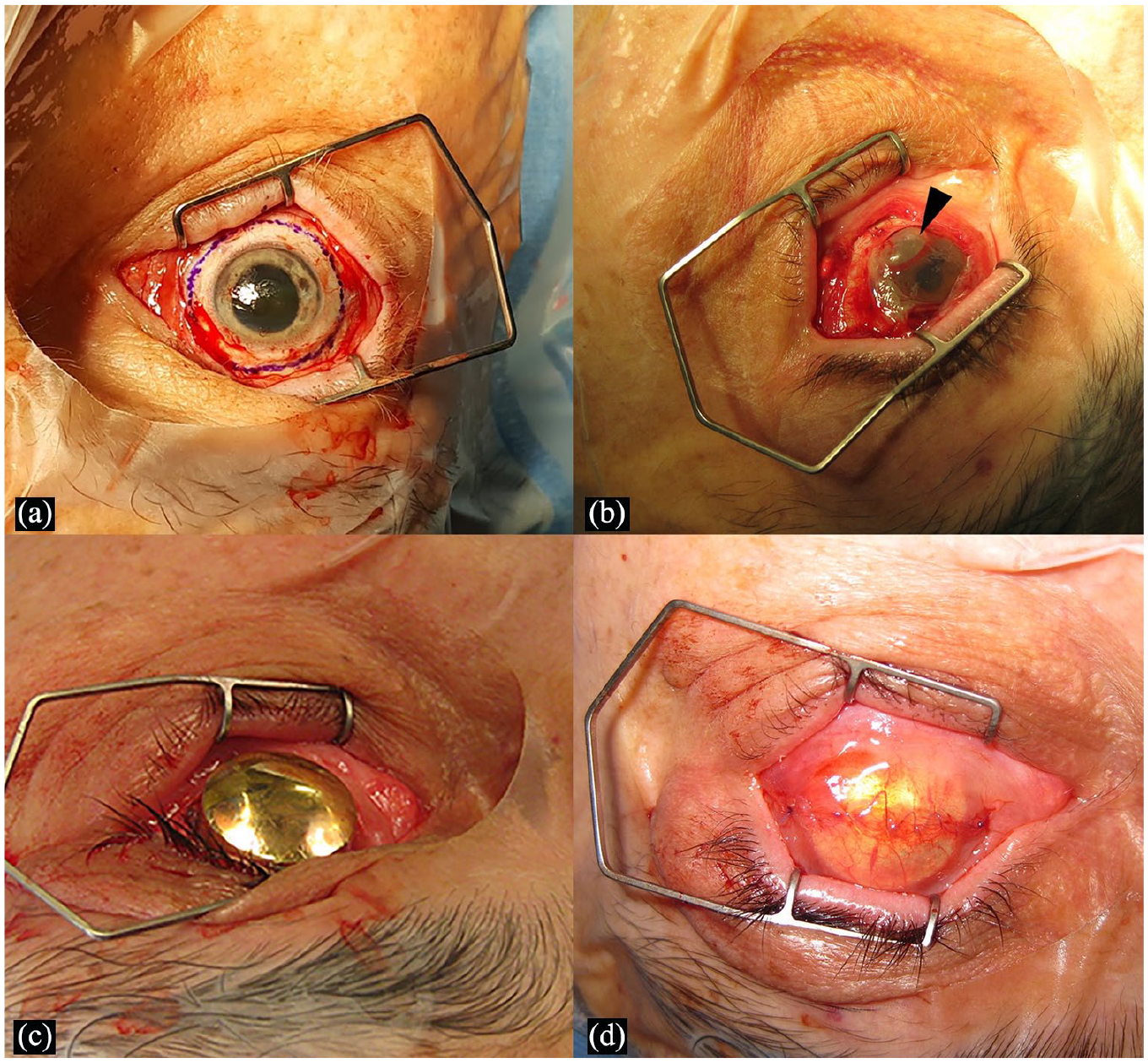
1(a–d): Representational external photographs showing the surgical technique of total anterior segment 103Pd plaque brachytherapy. (a): 360° paralimbal scleral marking equivalent to plaque diameter is used to define the target zone. (b) Note the transient air-bubble (arrow head) beneath the 25 × 25 mm amniotic membrane used to cover, buffer, and thus protect the corneal surface during treatment. (c) Standard round gold 103Pd radiation plaque aligned over the prior episcleral marks (a). (d) A Gunderson flap is used to cover the plaque and provide a smooth surface for eye lid closure.
Follow-up evaluations
Post-operative ophthalmic examinations were performed within 14 days, at 3 months and every 6 months thereafter. Ophthalmic oncology follow-up examinations focused on IOP, cataract progression and tumor response to treatment. Slit-lamp and gonioscopic photography and high-frequency ultrasonography, indirect ophthalmoscopy, fundus photography, fluorescein angiography, and optical coherence tomography were performed.
Results
Patients were aged 33–74 years (mean ± standard deviation (SD): 62.5 ± 12.6, median: 65 years). Right eye was involved in eight (72.7%) of the patients, and six (54.5%) were males. Multifocal iris melanoma confirmed with biopsy in nine patients. The 10th patient had unifocal disease, an initial biopsy and treatment with a partial anterior segment 103Pd plaque. However, 4.5 years later he developed, biopsy-proven multifocal iris melanoma treated by a second 103Pd plaque brachytherapy (to the entire anterior segment). The 11th patient presented with multifocal recurrence 4 months after being treated (elsewhere) with iodine-125 plaque radiation. According to the 8th edition of the AJCC staging system, there were five T1N0M0 (45.4%) and six T2N0M0 (54.5%) tumors. 4
Anterior segment tumor distribution
Five tumors were isolated to the iris and six (54.5%) had ciliary body involvement. The largest base diameter ranged 12–15.7 mm (mean ± SD: 13.5 ± 1.3, median, 14 mm) and largest tumor thickness ranged 1.4–3.7 mm (mean ± SD: 2.3 ± 0.7, median, 2.6 mm). Clinically visible circumferential extent in iris and angle ranged from 6–9 clock hours (median, 6). Multifocal biopsy-aided histopathologic examination confirmed the diagnosis of malignant melanoma of the iris.24,25 No vision loss, secondary glaucoma, or long-term complications could be attributed to tumor biopsy. The biopsy results reported epithelioid melanoma in two eyes and mixed spindle/epithelioid cells in eight.
Radiation treatment
Plaque sizes varied 14–20 mm (mean ± SD: 17.3 ± 1.6, median, 18 mm). Dosimetry study of radiation dose affecting vital intraocular structures showed that the median doses were as follows: tumor apex: 85 Gy (mean ± SD: 85 ± 2.5; range: 80–86 Gy); inner cornea: 155.6 Gy (mean ± SD: 153.8 ± 18.0; range: 114.2–186.5 Gy); central lens: 62.8 Gy (mean ± SD: 57.4 ± 19.8; range: 9.1–79.6 Gy); fovea: 2.5 Gy (mean ± SD: 3.2 ± 2.3; range: 1.7–10.0 Gy); and optic disk: 2.7 Gy (mean ± SD: 3.5 ± 3.1; range: 1.9–12.8 Gy) (Table 2).
Tumor response
A median of 41% (range: 15%–64%) reduction in tumor thickness was noted at a median 50 months (mean ± SD, 58.7 ± 47.1; range: 8–139 months) of follow-up by ultrasound biomicroscopy. The most common findings related to iris melanoma regression after 103Pd plaque brachytherapy were decreased intrinsic tumor vascularity, increased tumor pigmentation, decreased tumor thickness, and synchronous increased internal ultrasonographic reflectivity. 30
Local and systemic outcomes
In this series of 11 tumors, there was no evidence of local tumor recurrence at a median follow-up of 50 months. One patient has developed liver metastasis 2.5 years after total anterior segment plaque brachytherapy. Of interest, his was the tumor that recurred 4 months after initial 125I plaque elsewere. 31
IOP
The median IOP at presentation was 18 mmHg with four patients having pre-existing glaucoma. Following plaque treatment, three more patients developed glaucoma in absence of iris and angle neovascularization or significant melanomalysis. Six out of seven glaucoma patients had good IOP control with topical glaucoma medications and one (with pre-existing glaucoma) received an Ahmed glaucoma valve implant (New World Medical, Rancho Cucamonga, Los Angeles, USA).
Visual acuity
The final visual acuity was 20/16 to 20/40 in nine (out of 11) eyes (81.9%) and worse than 20/200 in two eyes (18.2%). Three or more lines of vision were lost in one patient, attributed to glaucoma leading to no light perception. Progressive or newly documented cataract was seen in five of eight phakic eyes (62.5%). The median time of development of cataract was 21.5 months (range: 12–36 months). Progression of pre-existing nuclear sclerosis was the most common type of cataract (four of five eyes). Four symptomatic cataracts were treated by extraction and intraocular lens insertion. No radiation-associated surgical difficulties were reported by the cataract surgeons.
Radiation complications
Despite total anterior segment plaque placement, no epiphora, eyelash loss, or visually significant dry eye were noted. Focal superficial corneal epitheliopathy was found in one eye (10%) in the early post-operative period (<1 month) which resolved with topical lubrication. Two of 11 patients had received prior anterior segment plaque brachytherapy with no additional anterior segment radiation toxicity. In this series, there were no clinical signs of corneal or scleral necrosis, radiation-induced retinopathy, maculopathy, or optic neuropathy (Figures 2 and 3).
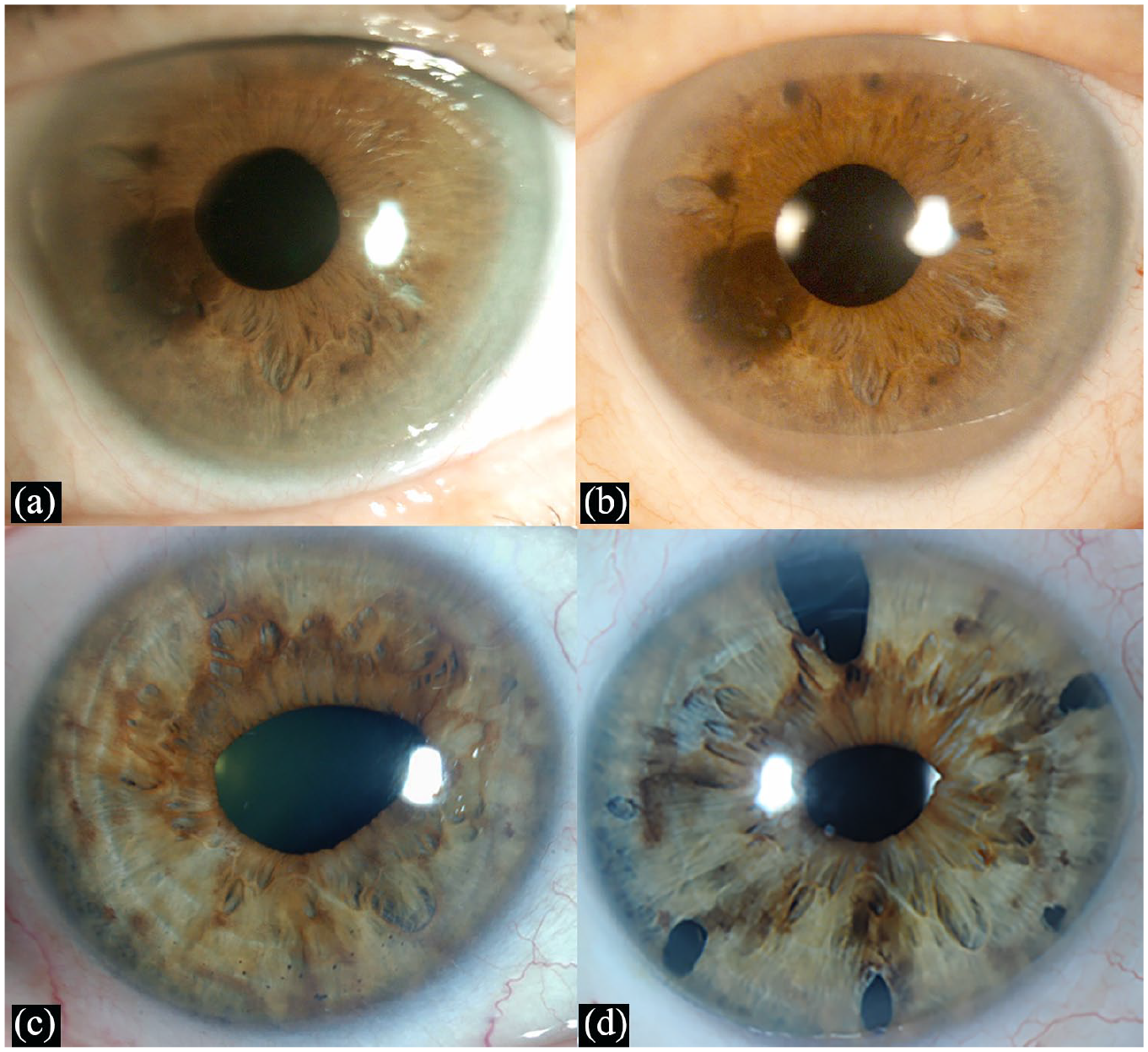
(a–d). Slit-lamp photographs of multifocal iris melanoma prior to and after total anterior segment 103Pd plaque brachytherapy: (a) pre-treatment, (b) 9 years post-treatment; note that diagnostic biopsy was performed with partial- and full-thickness iridectomy. (c) Pre-treatment, (d) 6 years post-treatment; note the significant decrease in iris pigmentation is associated with tumor regression.
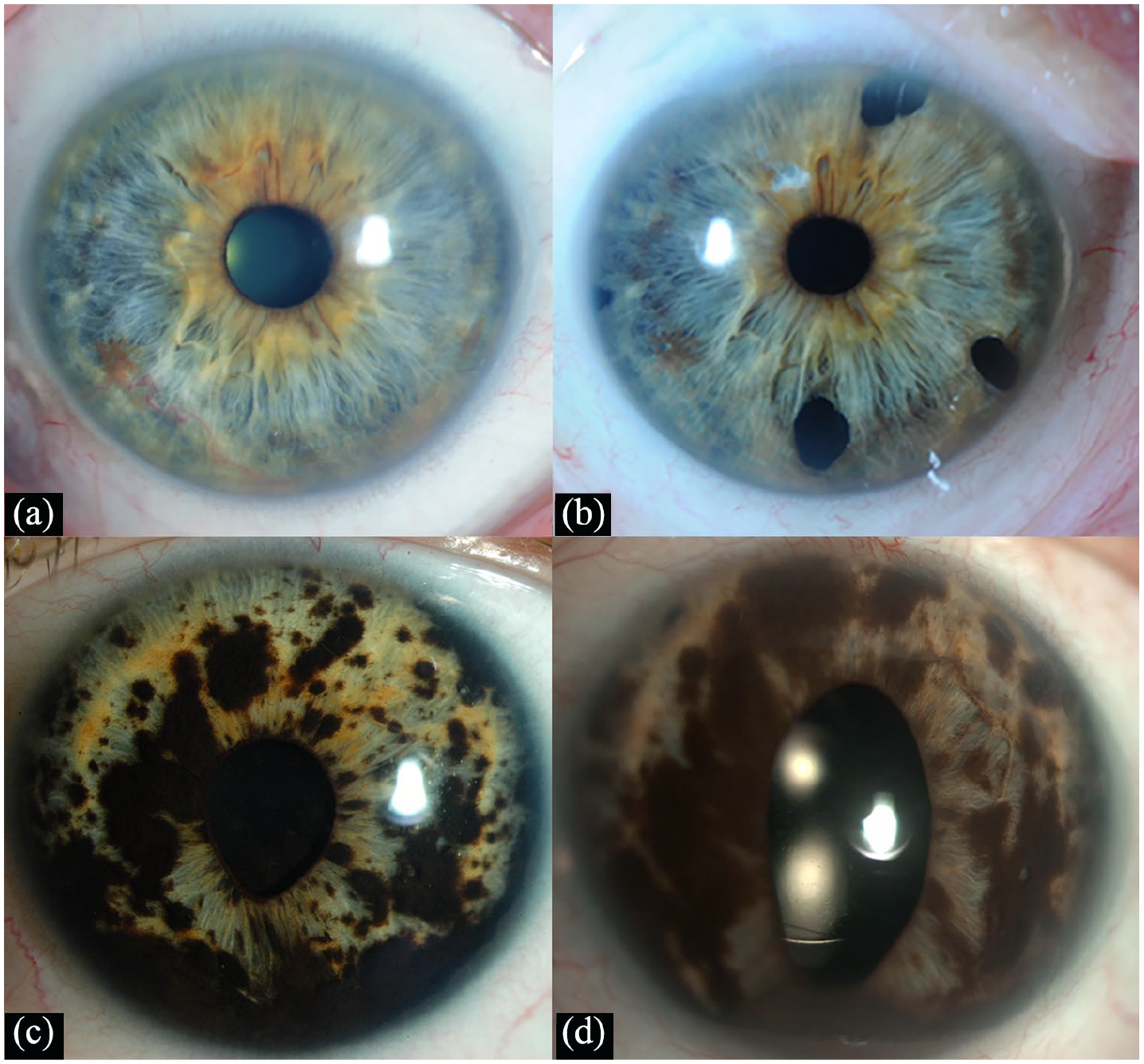
(a–d): Slit-lamp photographs of multifocal iris melanoma many years after total anterior segment 103Pd plaque brachytherapy: (a) Pre-treatment, (b) 4 years post-treatment, (c) pre-treatment, and (d) 3 years post-treatment. Note that all are pseudophakic and their corneas are clear.
Discussion
Total anterior segment ophthalmic plaque radiotherapy (103Pd) successfully controlled multifocal iris melanoma with no failures of local control nor need for secondary enucleation. Among phakic patients, rate of secondary cataract was high (n = 5/8, 62.5%) and successfully treated with cataract surgery. No patient developed keratopathy, radiation maculopathy or optic neuropathy. Moreover, at a mean follow-up of 50 months, 81.9% (9 of 11) patients maintained a BCVA > 20/30 at last follow-up. The patient who developed metastasis (after 2.5 years) was the one who had a history of failure of local control. 31
Few studies have investigated conservative management for multifocal or diffuse iris melanoma.
The first case of successful treatment of multifocal iris melanoma with 103Pd total anterior segment irradiation was reported by Petousis et al. 16 No significant complications were reported despite the high corneal radiation dose. A similar approach was employed in a single case by Lee et al. 32 using 125I seeds in a Collaborative Ocular Melanoma Study (COMS) plaque placed directly over the cornea. Corneal opacity in patients reportedly treated by 125I plaque radiotherapy and proton beam irradiation may be due to prescription dose or dose rate effects. Alternatively, the amniotic membrane grafts buffered and protected the cornea during 103Pd plaque brachytherapy.19,20
The plaque’s gold backing blocks radiation to sides and posterior resulting in no side-effects to adnexal tissue, eyelids, and healthcare personnel. In proton beam therapy, a radiation column is directed to the intraocular tumor through the front of the eye (anterior segment, eyelids, and/or orbit), and thus can result in eyelash loss, eyelid excoriation, corneal neovascularization and ulceration, severe dry eye, neovascular glaucoma, and cataract. 15 Compared to proton beam, sutured gold 103Pd epicorneal plaques move as the eyes move, leading to more reproducible radiation delivery.
Herein, we present a distinct entity where plaques were chosen as to cover all visible tumor plus additional margins which necessitated that the entire anterior segment was irradiated. In our center, both 125I and 103Pd seeds are available for radiation therapy. For each case, our choice of 103Pd was based on comparative pre-operative computerized dosimetry analysis of dose to normal ocular structures including the macula and optic nerve (Table 3).28,29
Whole anterior segment proton beam radiotherapy has been employed for treatment of multifocal iris melanomas. Konstantinidis et al. 17 used 58.4 CGE (cobalt gray equivalent) (53.1 Gy) in four fractions in 12 patients with median follow-up of 3.5 years and reported no tumor recurrence. Reported complications included the following: persistent corneal disease (33%), cataract (66%), and glaucoma (91.6%). Visual acuity was ⩽20/200 in 33% at the last follow-up. Since it is more difficult to localize proton therapy, Willerding et al. 18 used a total dose of 50 CGE in a heterogenous group of 54 patients (including cases of histopathologically proven iris nevi and melanocytoma). Local tumor control was 96.3% over 62.7 months mean follow-up. Cataract and glaucoma developed in 42.6% and 55.6% eyes, respectively, and visual acuity of 20/40 was preserved in 77.3% after surgery (Table 4).
Proton versus Palladium-103 anterior segment radiation.
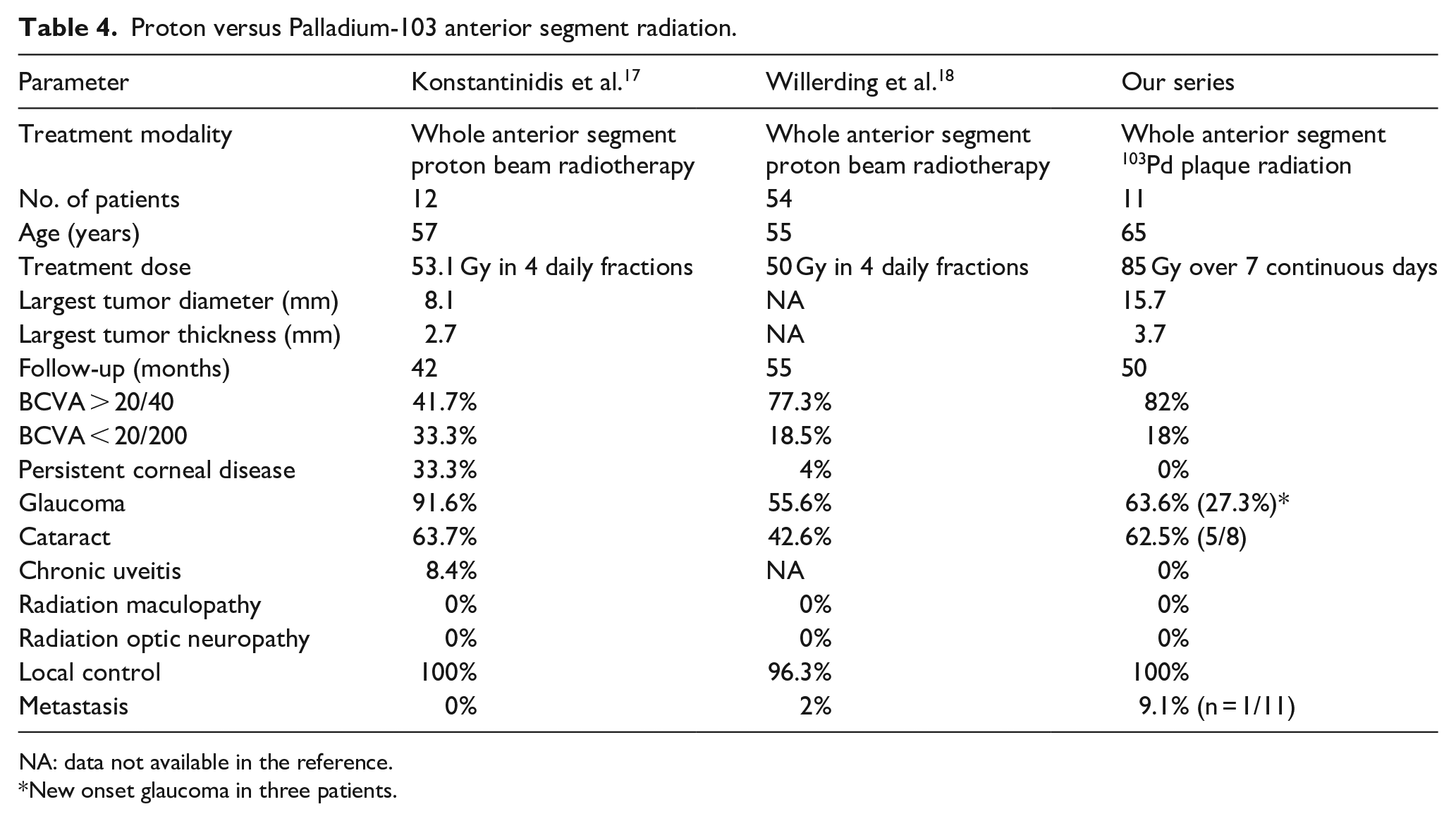
NA: data not available in the reference.
New onset glaucoma in three patients.
In our study, cataract was an expected, acceptable, and safely treatable consequence to iris brachytherapy. Elevated IOP was noted before treatment in four eyes (36.4%) and after radiotherapy in three additional eyes (27.3%). Glaucoma likely resulted from anterior chamber angle tumor and pigment seeding (but may have been affected by radiation therapy). 33 The post-radiotherapy-elevated IOP usually resulted from an open-angle configuration with increased pigmentation and no significant neovascularization. Patient discomfort with anterior segment plaque is due to metallic implant rubbing over cornea mitigated by use of total epicorneal amniotic membrane grafts. 20 In addition, Gunderson conjunctival flaps allowed the patient’s eyelids to glide over and leave the plaque relatively undisturbed.
Metastatic disease was seen in one patient (9.1%) in our study. Of interest, this tumor initially failed sectoral anterior segment plaque therapy and was finally locally controlled with a total 103Pd anterior segment plaque irradiation. Of note, the risk for metastasis has been shown to increase with local tumor recurrence of uveal melanoma. 31 This case emphasizes the need for high index of suspicion for multifocal disease in cases of clinically unifocal iris and iridociliary melanoma.
The retrospective design, small sample size, and the limited follow-up are shortcomings of our study. In addition, endothelial cell counts and quality-of-life assessments were not performed. However, this is the first reported clinical case series reporting the outcomes of total anterior segment plaque radiation for diffuse multifocal iris melanoma. This approach might increase the risk of cataract and glaucoma but is found to be effective in local tumor control, obviating the need for enucleation and providing excellent vision retention.
Conclusion
Palladium-103 plaque brachytherapy was a safe and effective globe-sparing treatment for multifocal iris melanomas. We found these patients to be suffering from pigment-related glaucoma prior to treatment. Radiation and tumor destruction affected the severity of glaucoma and cataract. However, there were no vision-limiting radiation side-effects on the cornea, macula, or optic nerve. Comparative studies of the available methods of radiation for multifocal iris melanoma are warranted.
Footnotes
Authors’ Note
This study was presented at the American Academy of Ophthalmology Annual Meeting, 2019.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.