
Abstract
Objective
To evaluate the performance of mesothelin, CA125, HE4 and ROMA index in the detection of malignant ovarian tumors.
Study Design
This is a cross-sectional study including 199 women with adnexal masses (67 with malignant tumors and 132 with benign tumors) and 150 healthy women (controls). We used a recursive multivariate partitioning algorithm to assess the contribution of each of the serum markers and the ROMA index to the discrimination of women with malignant tumors. Also, the areas under the ROC curves (AUC) for each of the serum markers and for the ROMA index were compared using the Venkatraman's projection-permutation test.
Results
In the recursive model, CA125 had the best performance in discriminating women with malignant tumors. In women with normal-range CA125 levels, none of the other markers contributed to the discrimination of women with malignant tumors. In women with elevated CA125 levels, elevated HE4 levels were associated with an increased risk of harboring a malignant tumor. The AUC for mesothelin was smaller than that for all the other curves, and both the ROMA index and CA125 had better AUC than HE4.
Conclusion
In women with normal CA125 levels, neither mesothelin nor HE4 contributed to discriminate women with malignant ovarian tumors; however, for women with elevated CA125 levels HE4 may help discriminating those who have a malignant ovarian tumor.
Introduction
Ovarian cancer is the deadliest gynecologic cancer, being recognized as the fifth cause of death due to cancer in women (1). Brazilian estimates for 2012 show that roughly 6,000 women will be diagnosed with the disease in the country (2). Ovarian cancers are diagnosed from a larger group of women presenting with adnexal abnormalities, and approximately 10% of all women in the United States undergoes surgery due to an adnexal mass. Only a small percentage of these women (17%-23%) will be diagnosed with an epithelial ovarian cancer (EOC) (3).
CA125 measurement is an important component of the workup of a woman with an adnexal mass (4). In women with tumors classified as potentially malignant with ultrasound, higher CA125 levels were associated with an increased risk of finding a histologically malignant tumor (5-7). Unfortunately, in premenopausal woman, abnormal CA125 levels may be associated with benign conditions such as endometrioma, follicular cysts, cystadenoma, abscess, and pregnancy. High serum concentrations of CA125 are also found in women with pancreatic, stomach, colon and rectum cancers, as well as in metastatic disease (8). This explains the tremendous amount of effort that has been spent in finding new ovarian cancer serum markers that could be used together with, or instead of, CA125 (9).
HE4 (human epididymis protein 4) is a relatively new serum marker for the diagnosis of ovarian cancer. HE4 has been shown to display increased sensitivity for detecting ovarian cancer compared to that of CA125 alone (10). Moore et al (11) developed a mathematical model to classify patients with a pelvic mass into high-risk or low-risk groups for having EOC, the Risk of Ovarian Malignancy Algorithm (ROMA), which combines CA125 and HE4 levels along with menopausal status in a logistic regression model. In recent studies, the ROMA index has been shown to outperform the Risk of Malignancy Index (11). In a meta-analysis including 11 studies from Africa, Europe and North America (12), the ROMA index has been shown to distinguish EOC from benign pelvic masses. The ROMA index was less specific but more sensitive than HE4. However, the ROMA index and HE4 were both more specific than CA125. HE4 levels in healthy women were associated with age, and one recent study showed that the median serum HE4 levels in premenopausal women is significantly lower than in postmenopausal women (13).
Mesothelin is another of the novel serum markers under investigation for the differentiation of adnexal masses (14). This marker is a membrane-bound protein present in normal mesothelial cells lining the body cavities, and is highly expressed in cells from malignant mesothelioma as well as in most EOC (15). The mesothelin/CA125 interaction may facilitate peritoneal metastasis by initiating cancer cell attachment to the mesothelial epithelium (16). The soluble mesothelin-related peptides were found to be elevated in sera of EOC patients.
The combined use of serum mesothelin, HE4 and CA125 may be of use in the setting of ovarian cancer screening and detection; also, these markers can contribute to the diagnosis of the disease in its early stages (14, 17, 18). The present study aimed at evaluating if the reported performance of CA125, HE4 and ROMA index in discriminating women with adnexal malignancies from women with benign adnexal masses or healthy women can be reproduced in a large sample of Brazilian women who attended gynecological consultations in a dedicated tertiary hospital.
Methods
We included 199 women with adnexal tumors (67 of whom were later diagnosed as having malignant tumors) operated between January 2010 and January 2012, and 150 healthy women (hereafter named “controls”) who attended the gynecological clinics of the institution due to other conditions not related to adnexal masses (treatment of climacteric ailments, human reproduction, and other apparently healthy women), in that same period. The study was approved by the ethical committee of the Faculty of Medical Sciences/UNICAMP, protocol #1092/2009. All women included in the study gave written informed consent. For women with andnexal tumors and controls we collected additional data such as age, menopausal status, and body mass index (BMI) (in Kg/m2). Peripheral blood was collected for serum quantifications of mesothelin, CA125 and HE4.
Serum Samples and Marker Assays
All serum samples were stored in aliquots at -80°C until analysis. The level of serum mesothelin was determined using the MESOMARK enzyme immunometric assay Kits (EIA) (Fujirebio Diagnostics, Göteborg, Sweden), according to the manufacturer's instructions. Values were expressed in nmol/L. Automated analysis of CA125 was performed using the OM-MA test (Siemens Medical Solutions Diagnostics, Tarrytown, USA). Values were expressed in U/mL. The level of serum HE4 was determined using the HE4 enzyme immunometric assay Kits (EIA) (Fujirebio Diagnostics, Göteborg, Sweden) according to the manufacturer's instructions and values were expressed in pmol/L. The ROMA index uses the results for HE4 and CA125 to generate a predictive index (PI) for EOC, calculated by the formulas proposed by Moore at al (19) for premenopausal and postmenopausal women. The ROMA index was used to stratify women into high-risk or low-risk groups for having a pelvic mass that is, respectively, malignant or benign.
Surgery and Pathological Assessment
Surgeries for diagnosis and/or treatment of the adnexal masses were performed at the hospital of the Department of Obstetrics and Gynecology of the Faculty of Medical Sciences (FCM/Unicamp) and the techniques and surgical procedures were chosen and performed according to medical indication. All patients with cancer were fully staged. The mean time elapsed between blood collection and surgery ranged from 24 hours or less, for emergency procedures, to a maximum of 120 days. The gold standard was the histopathological diagnosis of surgical specimens. Pathological processing and interpretation were performed by members of the Department of Pathologic Anatomy of the FCM/Unicamp following the guidelines of the World Health Organization International Classification of ovarian tumors (20).
Statistical Analysis
Data were entered into a Microsoft Excel (Microsoft Corp., Redmond, WA, USA) spreadsheet and analyzed with the R Environment for Statistical Computing software (21). All statistical calculations were performed using 95% confidence intervals (95% CI), and considered a p<0.05 as statistically significant. The sample size was calculated on the basis of the sensitivity of CA125 and HE4 reported in previous studies. With a 5% significance level, 80% statistical power and 12% error limit for the sensitivity, the minimal number of women with malignant tumors should be 64 and, based on the prevalence of malignancy, 122 women with benign tumors were needed for discrimination. The number of controls was estimated to be 149, with a total number of 335 women. We first calculated the proportion of women with elevated tumor markers across the histological strata of the tumors. Standard cutoff points were used: CA125 levels were considered positive when ≥35 U/mL in both pre and postmenopausal women. HE4 was considered positive when ≥70 pmol/L in premenopausal women and ≥140 pmol/L in postmenopausal women (22). In premenopausal women, a ROMA index ≥13.1% was considered high-risk, and the ≥27.7% cutoff point was used for postmenopausal women. Mesothelin was considered positive if ≥1.5 nmol/L in both pre and postmenopausal women. Box and whisker plots were generated in order to depict the distribution of serum marker concentration and ROMA index across selected subsets of women (Fig. 1). Next, the means and the interquartile ranges of the serum marker concentrations for various groups of women were calculated. We performed pairwise comparisons of the serum marker concentrations in the different groups of women, formed on the basis of the tumor histological classifications and stage (for carcinomas) using the Tukey's Honestly Significant Differences (Tukey's HSD) test. Receiver Operator Characteristics (ROC) curves were generated for each of the serum markers and the ROMA index (Fig. 2), having as the event of interest the identification of women with malignant tumors. Pairwise comparisons of the areas under the curves (AUC) were performed using Venkatraman's projection-permutation test (23). Finally, we used a recursive partitioning algorithm, based on a linear regression model to confirm the contribution of each marker to the diagnosis of malignant tumors. Patient's age and serum marker levels were included in the recursive partitioning regression model, and a conditional inference tree was generated. In short, conditional inference trees estimate a regression relationship by binary recursive partitioning in a conditional inference framework. Roughly, the algorithm works as follows: (i) tests the global null hypothesis of independence between any of the input variables (age, CA125, HE4 and mesothelin levels) and the response (histological diagnosis of the ovarian mass), and stops the computation if this hypothesis cannot be rejected. Otherwise selects the input variable with the strongest association to the response. This association is measured by a p value corresponding to a test for the partial null hypothesis of a single input variable and the response. (ii) Implements a binary split in the selected input variable. (iii) Recursively repeats steps (i) and (ii). Branches of the generated inference tree bifurcate when a statistically significant association is detected (p<0.05).

Box and whisker plots representing mean serum concentrations and the interquartile ranges of mesothelin (nmol/L), HE4 (pmol/L), CA125 (U/L), and ROMA index (%). Plots A, D, G, J: entire sample, comparing controls, women with benign and malignant tumors; plots B, E, H, K: only women with malignant tumors, plots comparing epithelial, stromal, germinative and metastatic tumors; plots C, F, I, L: only women with epithelial invasive tumors; the plots compare marker concentrations according to disease stage. P values were calculated with the Tukey's HSD (Honestly Significant Difference) test.
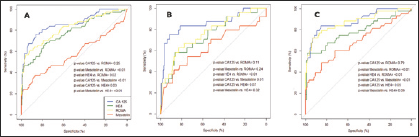
ROC curve analysis of CA125, HE4, mesothelin and ROMA index to evaluate their performance in discriminating women with malignant tumors from those with benign tumors or healthy women. A) Entire cohort; B) Premenopausal women; C) Postmenopausal women. Pairwise comparisons of the AUC for the serum markers were performed using the Venkatraman's Projection-Permutation test. AUC values: A) CA125=85.8%, HE4=77.8%, mesothelin=57.3%, ROMA=81.9%; B) CA125=85.5%, HE4=74.4%, mesothelin=63.6%, ROMA=76.4%; C) CA125=88.1%, HE4=78.4%, mesothelin=68.1%, ROMA=87.4%.
Results
The main clinical features of the women included in this study are shown in Table I. The mean age of women with malignant tumors was significantly higher than that of women with benign tumors and controls. Consequently, the proportion of postmenopausal women was significantly higher in the group of patients with malignant tumors compared to the other groups. BMI was evenly distributed across the study groups. Stage information for malignant tumors and mean serum concentrations of the studied markers across the study groups are also shown in Table I. More than 50% of the women with malignant tumors had stage I disease. Mean serum concentrations of CA125, HE4 and mesothelin were statistically similar in women with benign tumors and controls. However, the serum concentrations of the 3 markers were significantly elevated in women with malignant tumors compared to either those with benign tumors or controls (Tab. I).
Key Clinical Features of Women with Ovarian Malignant Tumors, Benign Tumors and Controls
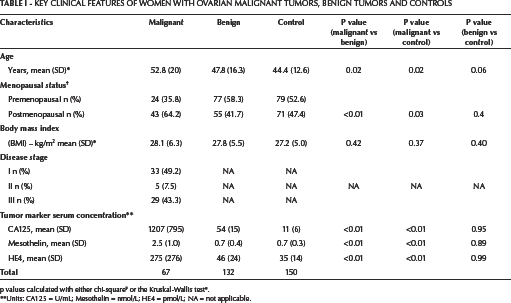
the Kruskal-Wallis test
p values calculated with either chi-square
Units: CA125 = U/mL; Mesothelin = nmol/L; HE4 = pmol/L; NA = not applicable.
Table II shows the proportion of women with different histological subtypes of malignant tumors with elevated tumor marker levels. Epithelial malignant tumors prevailed over the other histological types, but in the present sample 21% of the malignant tumors were of germinal or stromal histology. CA125 levels were positive in 45/67 (67%) women with malignant tumors. In the subset of women with malignant epithelial tumors, 29/37 (78%) had elevated CA125 levels. However, none of the women with mucinous adenocarcinomas and only 3/10 women with borderline tumors had positive CA125 levels. HE4 levels were positive in 28/67 (41.7%) women, while mesothelin levels were positive in 17/67 (25.4%) cases. Women with mucinous adenocarcinomas had normal levels of mesothelin and HE4. None of the women with borderline epithelial tumors had abnormal HE4 or mesothelin levels (Tab. II).
Proportions of Women with Malignant Tumors with Elevated ∗ Serum Levels of the Tumor Markers
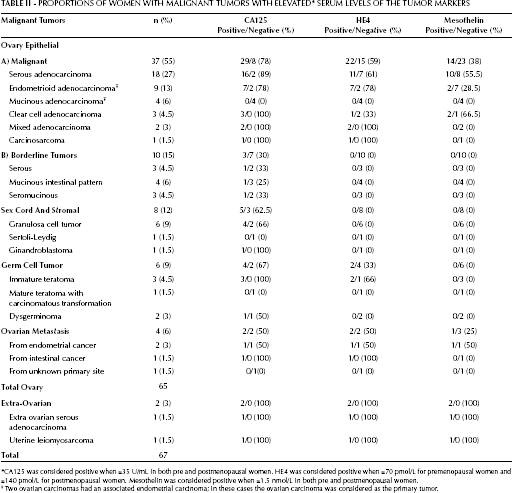
CA125 was considered positive when ≥35 U/mL in both pre and postmenopausal women. HE4 was considered positive when >70 pmol/L for premenopausal women and >140 pmol/L for postmenopausal women. Mesothelin was considered positive when >1.5 nmol/L in both pre and postmenopausal women.
Two ovarian carcinomas had an associated endometrial carcinoma; in these cases the ovarian carcinoma was considered as the primary tumor.
Epithelial tumors prevailed over other histological types in women with benign tumors. Germinative (mature teratomas) and stromal tumors (fibromas) were also common. CA125 was positive in 23/132 (17%) women with benign tumors. Women with cystadenomas, fibromas, teratomas and endometriomas presented the highest proportions of positive CA125 levels among women with benign tumors. HE4 levels were positive in only 3/132 (2%) women with benign tumors (2 with epithelial tumors and 1 with endometrioma). Mesothelin was positive in 11/132 (8%) women, evenly distributed accross the histological subtypes (Tab. III). Of the 23 women with benign tumors and positive CA125 levels, both HE4 and mesothelin levels were positive in only 1 case each (data not shown in Table).
Proportions of Women with Benign Tumors with Elevated ∗ Serum Levels of the Tumor Markers
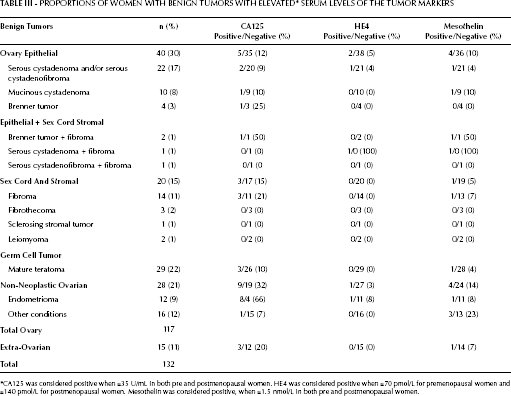
CA125 was considered positive when ≥35 U/mL in both pre and postmenopausal women. HE4 was considered positive when >70 pmol/L for premenopausal women and >140 pmol/L for postmenopausal women. Mesothelin was considered positive, when >1.5 nmol/L in both pre and postmenopausal women.
Figure 1 shows box and whisker plots representing the key distributions of HE4 and CA125 serum concentrations and ROMA index in the following groups: controls and women with benign or malignant tumors (plots A, D, G, J); women with malignant tumors, comparing those with epithelial, stromal, germinative and metastatic tumors (plots B, E, H, K); women with epithelial invasive tumors, according to disease stage (plots C, F, I, L). CA125, HE4, ROMA index and mesothelin were significantly elevated in women with malignant tumors compared to women in either of the other groups. The concentrations of the 3 serum markers and the ROMA index were similar in women with benign tumors and controls. The same was true for women with borderline tumors, benign tumors, and controls (data not shown in the figure). Women with ovarian carcinomas had CA125, HE4 and mesothelin levels significantly higher than women with malignant stromal tumors, germ cell tumors and healthy women. The CA125, HE4, and mesothelin levels and the ROMA index were significantly higher in women with stage III/IV carcinomas compared to women with stage I/II carcinomas and controls. On the other hand, the serum concentrations of all the markers, except mesothelin, were significantly higher in women with stage I/II carcinomas when compared to the control group and those with benign tumors.
In Figure 2, the ROC curves for each marker were compared. When comparing the curves for women regardless of their menopausal status (A), the AUC for mesothelin was significantly smaller than that for all the other curves. The AUC for CA125 and ROMA index were significantly higher than that for HE4 alone. In premenopausal women (B), the ROMA index performed better than HE4 alone, and CA125 performed better than mesothelin. In postmenopausal women (C), the ROMA index and CA125 performed better than mesothelin, and the ROMA index performed better than HE4. AUC values for each ROC curve are displayed in the footnote of the Figure.
Figure 3 is a graphical representation of a conditional inference model (conditional inference tree), in which CA125, HE4, mesothelin levels, and patient age were included. CA125 level was the factor that had the greatest capacity to discriminate histologically benign from histologically malignant tumors (p<0.001), as shows the first branch bifurcation of the tree. For patients with normal CA125 levels, neither age nor the HE4/mesothelin levels contributed any further to the detection of histologically malignant tumors. In contrast, in the group of women with elevated CA125 levels, the branch bifurcation shows that HE4 levels contributed significantly to the detection of histologically malignant tumors (p<0.001).
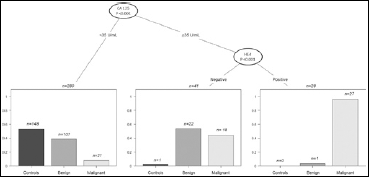
Conditional inference tree for pathologically confirmed tumor malignancy based on a recursive partitioning regression model. Only significant associations are displayed in the tree, at branch bifurcations. Variables included in the model were: age, CA125, HE4 and mesothelin levels. Of note, although included in the model, age and mesothelin do not appear in the tree because no significant association between these variables and the pathological diagnosis of malignancy was found.
Discussion
In this cohort of Brazilian women, the associated or stand-alone use of HE4 and CA125 was of little, if any, use for the discrimination of women with malignant ovarian tumors from women with benign tumors or healthy controls. The accuracy of CA125 for the detection of malignant ovarian tumors was higher than those of HE4 and mesothelin. Women with an adnexal mass and elevated levels of CA125 and HE4 had a significantly higher probability of harboring a malignant ovarian tumor than women with normal HE4 levels. However, women with malignant epithelial tumors, especially with serous, endometrioid, clear cell, and mixed carcinomas, had a significantly higher probability of having elevated CA125 and HE4 levels. Also, only women with carcinoma (primary or metastatic) had elevated levels of mesothelin. However, women with mucinous carcinomas and the majority of those with borderline tumors had normal CA125 levels, and in these cases HE4 and mesothelin were in their normal ranges.
CA125 levels were significantly higher in women with malignant tumors; the same was true for HE4 and mesothelin. Overall, HE4 was negative in all women with malignant tumors who also had negative CA125 levels, thus resulting in a lower sensitivity and worse accuracy than CA125. The ROMA index and CA125 had better AUC than HE4; unfortunately, the ROMA index was less sensitive than CA125 as a stand-alone marker. However, we did not set the 75% specificity threshold, and instead used the point on the ROC curve at which we had minimal false-negative and false-positive results (24). Women with malignant germinative or stromal tumors rarely had positive CA125 and HE4 levels. These data are in accordance with other studies that showed that HE4 may help detecting ovarian carcinoma (19, 24).
Women with serous adenocarcinomas had higher levels of CA125, HE4 and mesothelin than women with other types of carcinoma (14). Also, in this subset of women with carcinomas, the levels of the 3 markers were significantly higher in women with stage III/IV disease compared to women with stage I/II disease. However, women with stage I/II disease had significantly higher levels of CA125 and HE4 (while mesothelin was at normal levels) compared to women with benign tumors and controls. Abdel-Azeez et al (14) and Fritz-Rdzanek et al (17) found significantly higher levels of mesothelin in women with stage III/IV disease compared to women with stage I/II disease. Therefore, HE4 levels may be of clinical significance in women with early stage carcinomas, since only half of these women have elevated levels of CA125.
Bandiera et al (4) observed that in a group of 21 women with early stage ovarian carcinomas, 11 had elevated levels of HE4, 15 had elevated levels of CA125, and ROMA index was suggestive of malignancy for only 14 women. Moore et al (22) reported that when the ROMA index was used in a preset specificity of 75%, its sensitivity was 85.5% for the detection of stage I/II carcinomas in women with adnexal masses. In another study, the same authors classified as at high-risk for malignancy 75% of the women with early stage carcinomas (11). However, in other studies, CA125 was still the best option for the detection of early stage carcinomas, because HE4 levels have been found to be elevated only in women with advanced disease (7).
All women with mucinous carcinomas had negative CA125, HE4 and mesothelin levels, regardless of the tumor stage. Our findings agree with those of Van Gorp et al (9) and Yip et al (5), who studied, respectively, a cohort of Belgian and American women. Conversely, Abdel-Azeez et al (14), studying a cohort of Egyptian women, found that 66% of the patients with mucinous carcinomas who had low levels of CA125 had elevated levels of HE4. In their study, mesothelin was not elevated in women with mucinous carcinomas.
In our study, women with borderline ovarian tumors rarely had elevated levels of the markers: only 3/10 (30%) women had elevated CA125 levels and none had elevated levels of HE4 or mesothelin. Ponceletet et al (25) reported that 82/202 (40.5%) women with borderline tumors had elevated levels of CA125. Moore et al (3) using the ROMA index classified 14 of 19 women with borderline tumors as at high-risk. Since then, in many studies, CA125, HE4 and the ROMA index have been shown to fail in differentiating borderline tumors from benign tumors or healthy women (26, 27, 28).
As a limitation of our study, we used a Siemens platform for the measurement of the serum levels of CA125 (OM-MA test Siemens Medical Solutions Diagnostics, Tarrytown, USA) and the HE4 EIA Kit (Fujirebio Diagnostics) to measure the serum levels of HE4. We must acknowledge that many different CA125 platforms have been developed and are not directly comparable. For this reason there are different cutoffs to distinguish high and low-risk groups using the ROMA index, depending on the platform employed to measure the serum levels of the biomarker. In fact, the ROMA index was developed using the Abbott Architect platform to measure CA125 and the HE4 EIA Kit (Fujirebio) to measure HE4. The optimal ROMA index cutoffs for these 2 platforms have been determined and are 27.7% for postmenopausal women and 13.1% for premenopausal women. When using a different platform, such as the Abbott Architect platform, to measure both CA125 and HE4, the optimal cutoffs have been determined to be 25.3% for postmenopausal women and 7.4% for premenopausal women. To date there have been no published data examining the ROMA index cutoffs for the Siemens CA125 platform and the Fujirebio HE4 platform combination. These cutoffs may be somewhat different than the cutoffs determined for the combination of the Abbott Architect CA125 and HE4 EIA reported by Moore et al 2011 (11) and used in this paper.
In our series, 8 among the 12 women with endometrioma had CA125 levels higher than 35 U/mL and HE4 was positive in only 1 case. In premenopausal women, HE4 played a better role in predicting which adnexal masses were benign. In these women, several clinical conditions, like endometriomas, are associated with elevated levels of CA125. In these cases, CA125 levels are usually elevated. Holcomb et al (29) observed that 85% of 229 premenopausal women with adnexal masses actually had benign tumors; 41% of these women had elevated levels of CA125 and only 8% had elevated levels of HE4. Moore et al (30) found that 37% of 593 pre or postmenopausal women had elevated levels of CA125.
Because benign adnexal tumors can be treated safely by non-specialized gynecologists, the presurgical differentiation of tumors would benefit medical assistance (31). In conclusion, our results suggest that women with an adnexal mass and elevated levels of CA125 and HE4 have a significantly higher probability of harboring an ovarian carcinoma than those with normal HE4 levels. We also observed that HE4 was useful in detecting early stage disease. However, in general, women with mucinous carcinomas and borderline tumors had normal CA125 levels and, for these women, the determination of serum HE4 levels had no clinical importance. HE4 can contribute to the identification of women with benign tumors among those with an adnexal mass and elevated levels of CA125, as is true for endometriomas. On the other hand, the serum concentrations of mesothelin are seldom increased in malignant tumors. Mesothelin levels are similar in women with stage I/II carcinomas, women with benign tumors, and healthy women. Based on our results, it is not clear whether these new tumor markers should be recommended in the clinical setting for discrimination of women with adnexal masses.