
Abstract
Introduction:
At present there is no predictive value univocally associated with the success of chemotherapy. Biomarkers produced by ovarian cancer (HE4 and Ca125) could have a good prognostic significance. The aim of this study is to prove the ability of biomarkers to identify patients with the highest risk of non-optimal response during the chemotherapy, and to predict which patients will most likely develop recurrence of disease.
Methods:
We analyzed 78 patients with epithelial ovarian cancers who underwent surgery in the biennium 2016–2017. All the patients underwent chemotherapy after surgery or interval debulking surgery following neoadjuvant therapy. Serum levels of HE4 and Ca125 were measured at diagnosis and at each cycle of chemotherapy. We established the degree of response to the treatment by computed tomography scan, and the patients were followed up (median: 10 months). The parameters of progression-free survival and disease-free survival were related to serum levels of biomarkers.
Results:
Both CA125 and HE4 values became negative at the fourth cycle in the patients with good response to chemotherapy. HE4 increased earlier than Ca125. The parameters that best correlated with a long progression-free survival were: negativization of the marker after the third cycle of chemotherapy (HE4: odds ratio (OR) 5.5; Ca125: OR 9.1) and biomarker serum levels lower than the mean value in the affected population at the time of diagnosis (HE4: OR 3.4; Ca125: OR 3.7).
Conclusions:
We can conclude that the monitoring of HE4 and Ca125 during chemotherapy, especially at the third cycle, is recommended, because their variation is a good prognostic factor.
Introduction
Ovarian cancer is the second most common malignant gynecological tumor in developed countries with an incidence of 9.1 per 100,000 and a mortality of 5 per 100,000; it is also the third most common malignant gynecological tumor in developing countries with an incidence of 5 per 100,000 and a mortality of 3.1 per 100,000. 1 Overall survival (OS) in malignant ovarian cancer is related to the stage at diagnosis: actually 90% of stage I disease is alive at 5 years compared with 75%–80% of stage II, and 35%–40% at stages III and IV. 2 This poor result is largely related to the diffusion of the disease beyond the ovary at the time of diagnosis in 75% of patients. 3 Mortality has slightly decreased in the last 30 years. 4 After cytoreductive surgery and adjuvant chemotherapy, the majority of patients report a clinical complete remission. However, 50%–70% of patients will experience a relapse associated with chemo-resistance 2 : this is one of the major challenges to deal with in ovarian cancer research. 5 Hence, there is a need of suitable biomarkers that might predict platinum sensitivity, surgical outcome, and finally survival.
Up to now, the most promising new indicator seems to be human epididymis protein 4 (HE4). 6 In fact, it was shown as an earlier indicator of recurrence of ovarian cancer compared to CA125, with a lead time of 5–8 months. 7 The sensibility and specificity of HE4, alone or in association with other markers (CA125, CA72.4), seem to be higher for relapse diagnosis compared with CA125 alone. 8 Despite this, CA125 has been traditionally used to monitor response to treatment and to detect recurrence. This biomarker is highly specific, but not suitably sensitive for monitoring a complete response to primary therapy because not all epithelial ovarian cancers (EOC) produce elevated CA125 (e.g. in mucinous tumors). 9 Therefore, growing interest about the role of new serum biomarkers has been observed over recent years as published by our study group. 10
Many algorithms have been proposed combining different parameters 11 : RMI was proposed in 1990 by Jacobs et al., 12 using CA125, ultrasound findings, and menopausal status. With recent formula variations, its sensitivity rises to 96.7% with 84% specificity. In 2009, Moore et al. 13 proposed a new algorithm: Risk of Ovarian Malignancy Algorithm (ROMA). 13 They associated HE4 and CA125 levels according to the menopausal status, defined by the absence of menstruation or clinical signs of menopause for 6 months. Recently, ROMA was reported as having a non-significant different specificity to CA125 (approximately 92.5%). 14 At the same time, ROMA was more sensitive than HE4 (96.7% and 73.3%, respectively) but with less specificity (80% vs. 98.6%). 15 The dual measurement of CA125 and HE4 appears to be the best diagnostic tool over both ROMA and RMI algorithms. 12
In the present study, we correlated the serum levels of CA125 and HE4 before each chemotherapy cycle together with their response curve to the clinical response to treatment, platinum-sensitivity, and progression-free survival (PFS).
Materials and methods
This prospective observational study was conducted on 78 women with EOC who underwent surgery in the period from 1 January 2016 to 31 December 2017 at Sant’Anna Hospital - A.O.U. Città della Salute e della Scienza of Turin. The study was approved by the Local Ethics Committee and all patients gave written consent. Patients were staged according to 2014-FIGO International classification 16 and underwent first-line surgery followed by first-line chemotherapy or neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) and subsequent chemotherapy.
The measurements of HE4 and CA125 serum levels were assessed by an electro-chemo-luminescence assay on an automated cobas® 6000 platform (Roche AQ18 Diagnostics, Rotkreuz, Switzerland). The value of serum biomarkers was obtained at the time of diagnosis, before interval surgery for patients who underwent neoadjuvant chemotherapy and the day before each cycle.
Chemotherapy schemes in use were: carboplatin and Taxol (66 patients, 84.6%), carboplatin and liposomal doxorubicin (2 patients, 2.6%), or carboplatin alone (10 patients, 10.6%). Patients received a median of six cycles. Patients with stage IIIB, IIIC, and IV without contraindications underwent bevacizumab maintenance therapy; the markers level was not measured at every cycle during maintenance therapy. The residual tumor was reported after surgery as equal or greater than zero.
To assess treatment results we considered: PFS, disease-free survival (DFS), 2-year survival and platinum-resistance assessment. We referred to standard definitions: platinum sensitive patients, if the DFS period was longer than 6 months after the end of first-line chemotherapy; platinum resistant patients, if the DFS period was shorter than 6 months after the end of first-line chemotherapy; platinum refractory patients, if progression occurred during first-line chemotherapy; PFS from the initial diagnosis to recurrence of the disease; DFS from the end of chemotherapy to relapse; and OS from the initial diagnosis to death, last contact, or loss of follow-up. Platinum-resistant and platinum-refractory patients were defined as non-responders to first-line chemotherapy.
At the end of the therapeutic process, patients were included in follow-up programs in which—according to the latest international guidelines—clinical evaluation with pelvic examination and measurement of CA125 is often carried out every 3 months for 2 years, then every 6 months for 3 years, and then annually. 17 During follow-up visits, the rising of markers above the threshold value of 35 IU/mL, or new symptoms, was an indication for computed tomography, and the standard RECIST criteria were adopted.
A residual tumor (RT) of zero was considered an optimal cytoreduction, while a suboptimal cytoreduction was diagnosed with a visible residual mass.
For statistical analysis SPSS ver. 20 (SPSS Inc., Chicago, IL) was used. Contingency tables were created for the study of categorical variables; frequency data were evaluated using the exact Fisher test or Pearson Chi-square test. Mean values of HE4 and CA125 were not normally distributed and were compared adopting a non-parametric U-Mann Whitney test, for normally distributions Student’s T test for was used. To assess the influence of HE4 and CA125 markers on PFS, Kaplan–Meier curves were obtained. The differences from classes were evaluated using the Log-rank test. For this purpose, we tested different parameters: median baseline and 75th percentiles of the baseline of marker values, 50% decrease of serum markers after surgical treatment, and normalization of the markers after the third course of chemotherapy. The area under the curve (AUC) was calculated with a receiver operating characteristics (ROC) analysis. Finally, monovariate analysis of PFS was performed using logistic regression Cox Proportional Hazard models to derive odds ratio (OR) and confidence intervals (CIs) to predict patient outcome, including response to platinum therapy (responders vs. non-responders), relapse, and 2-year survival. Parameters studied in the multivariate Cox analysis included age, FIGO stage, grade, residual disease at surgery, and serum HE4 and CA125 values. Age was assessed as a continuous variable; FIGO staging was divided into I/II versus III/IV, grade G1+G2 versus G3; and residual disease into optimal versus suboptimal surgery. The P values were considered significant for values of α <0.05.
Results
Median age at diagnosis was 62 years (range 36–83 years). Most patients (62.8%) were diagnosed with advanced cancer (stage III–IV) while 37.2% were diagnosed with early stage cancer (stage I–II). As reported in the literature, the majority of tumors had serous histotype (53.8%); however, the endometrioid type was well represented (30.8%). A total of 59 patients underwent primary debulking surgery (PDS) and 19 underwent neoadjuvant chemotherapy followed by interval debulking surgery. Residual tumor after surgery was reported in 19 patients. Study population characteristics are reported in Table 1.
Clinical-pathological characteristics of the study group.
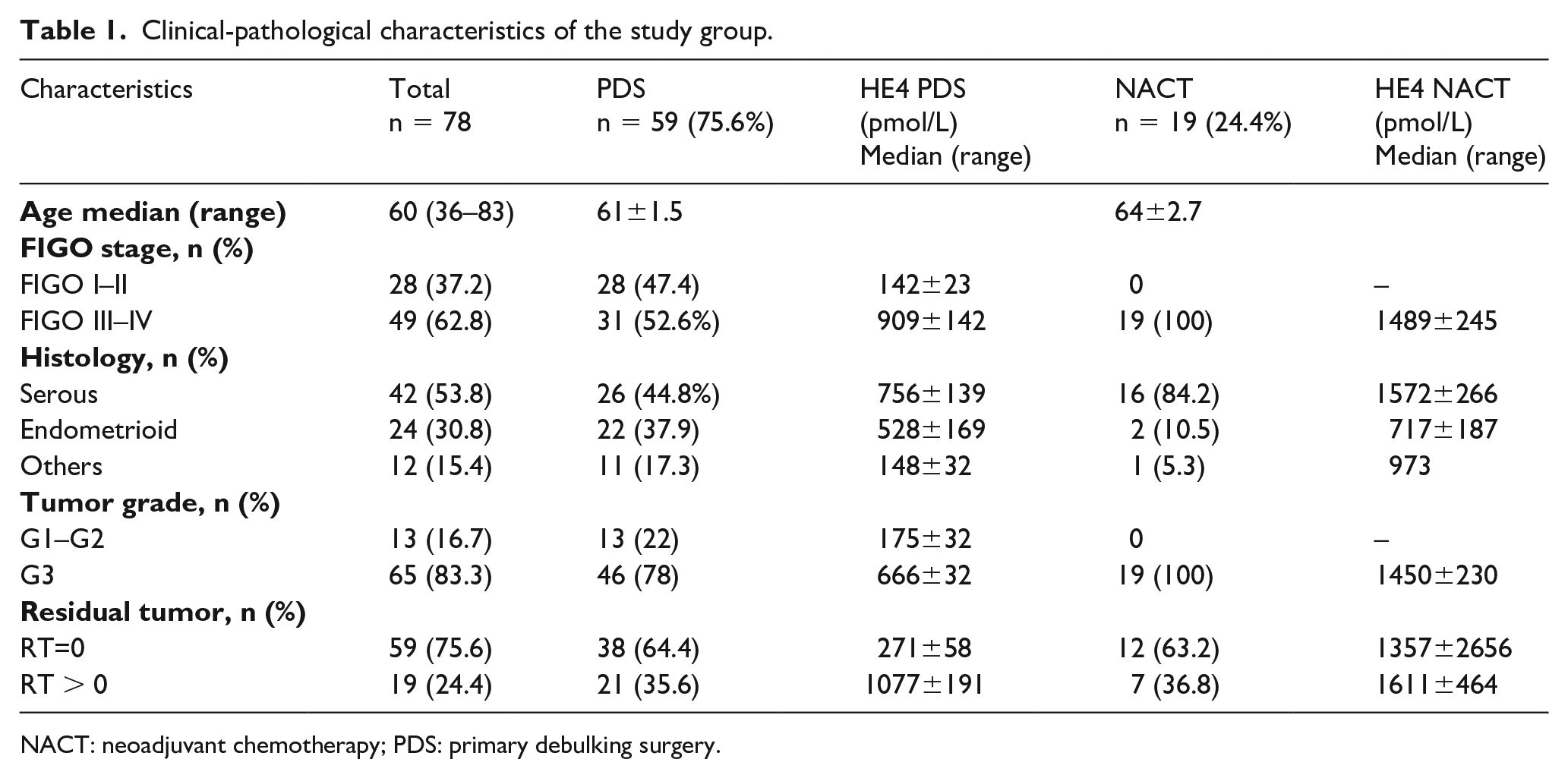
NACT: neoadjuvant chemotherapy; PDS: primary debulking surgery.
Considering HE4 values at the time of diagnosis, we observed a mean value of 775 pmol/L (median 374; range 54–3711) while a mean value of 1387 IU/mL for CA125 (median 426; range 20–36448).
In Table 2 we report the mean value of the two biomarkers at diagnosis according to the clinical and histological characteristics of the disease.
Comparison of the median levels of serum HE4 and CA125 according to prognostic factors, PFS, OS, and platinum-sensitivity.
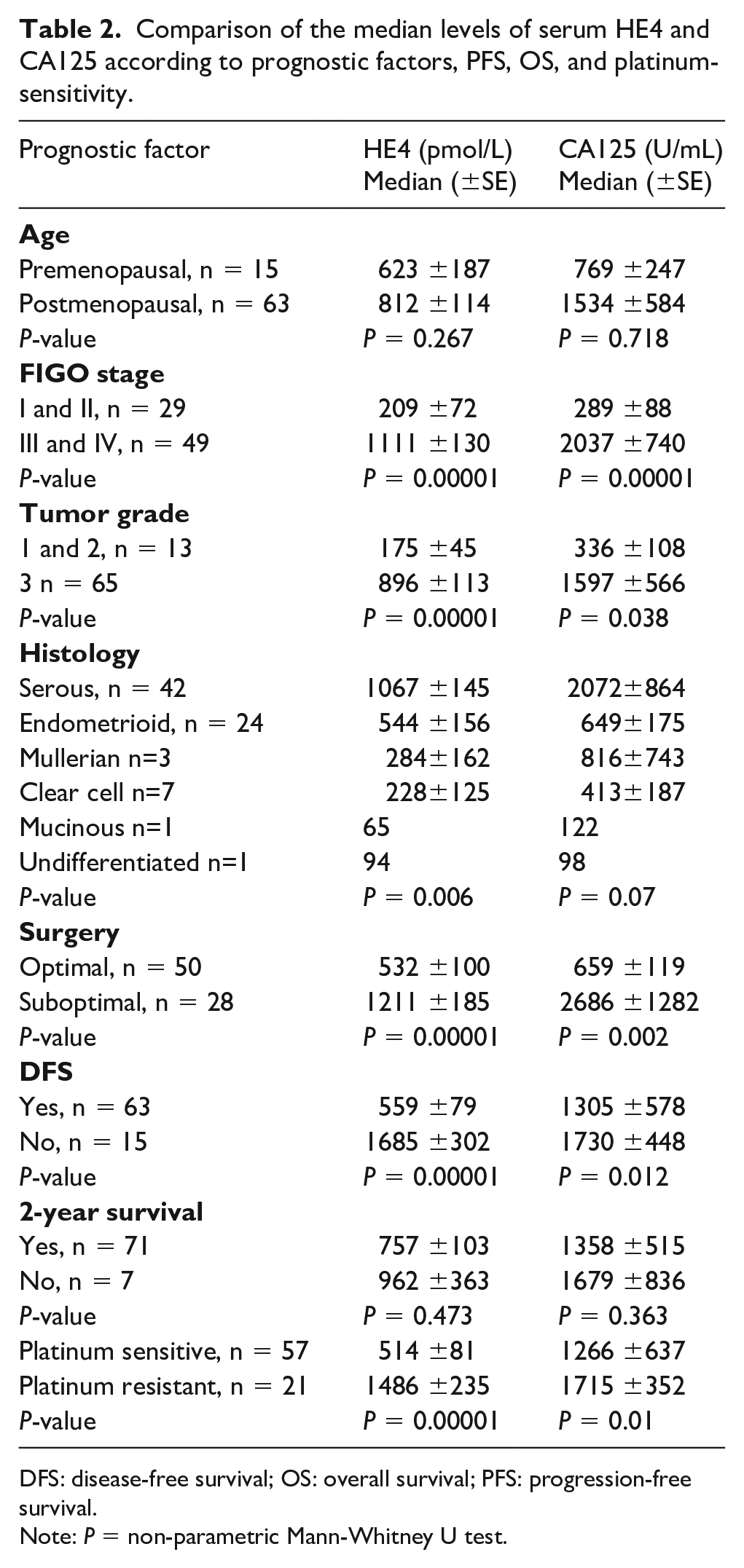
DFS: disease-free survival; OS: overall survival; PFS: progression-free survival.
Note: P = non-parametric Mann-Whitney U test.
In analyzing the time course of average marker values at each cycle we observed that they reached normal values at the fourth cycle and then remained negative until the end of chemotherapy.
Of the 78 patients, 57 (73.0%) were sensitive to chemotherapy, 13 were partially resistant (16.6%), and 8 were refractory (6.4%). In the sensitive group, we noticed a median value of normalization of HE4 at the third cycle (106.07 pmol/L) and of CA125 at the fourth cycle (29.02 IU/mL); while the resistant/refractory patients showed a fluctuating trend with an increase already at the sixth cycle for HE4 (918.73 pmol/L).
To determine the predictive value of baseline serum levels of HE4 and CA125, ROC curves and AUC were determined. In Figure 1 we report AUC curves and values for the ability of HE4 and CA125 to predict surgical outcome (Figure 1 (a)), platinum sensitivity (Figure 1 (b)), 2-year OS (Figure 1 (c)), and finally to reach a disease survival status (Figure 1 (d)). P values are reported in the chart.
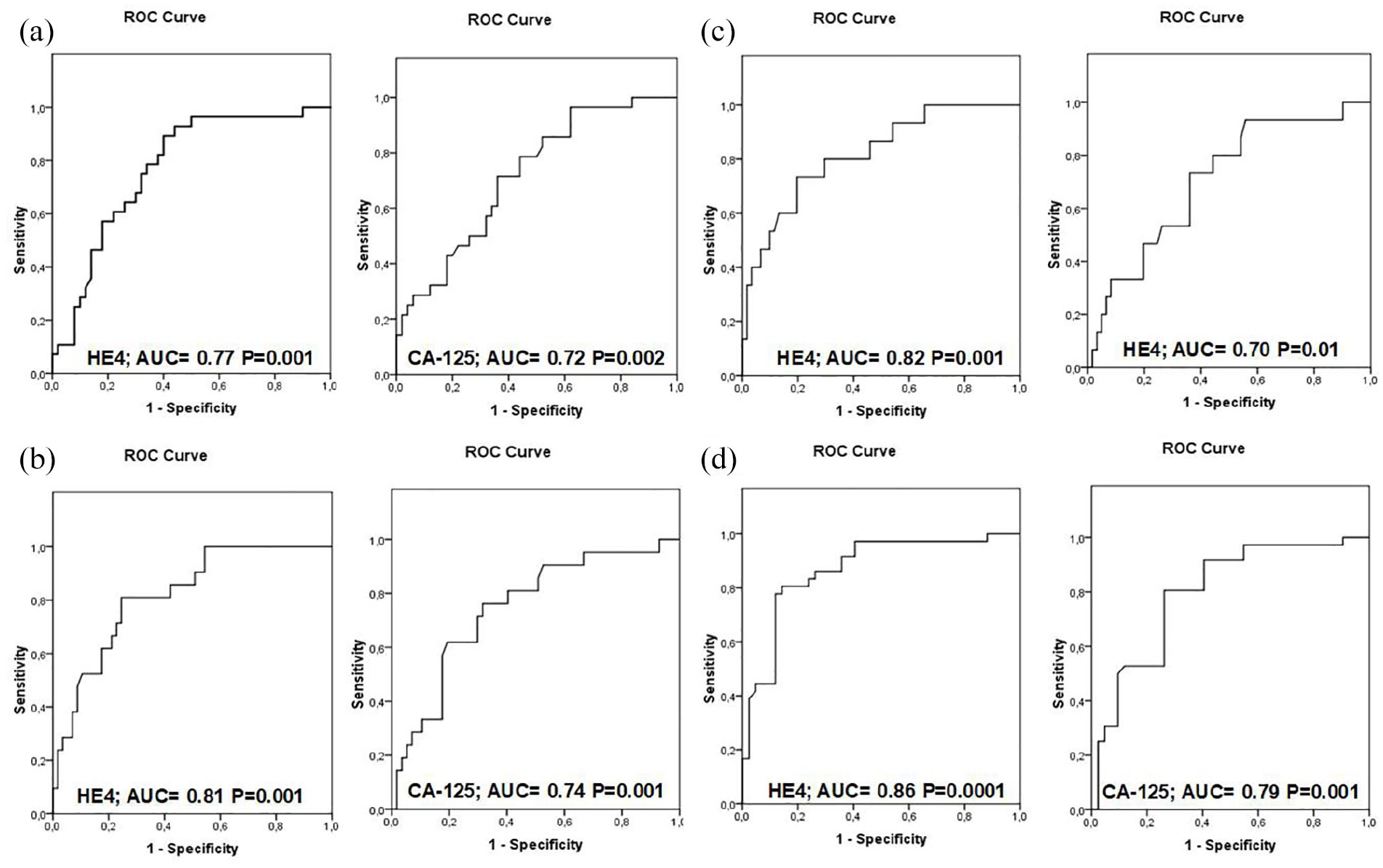
ROC curves of plasma HE4 and CA125. (a) Maximal cytoreduction with RT=0 vs. suboptimal debulking with RT>0. (b) Platinum sensitive vs. platinum resistant/refractory. (c) Reached 2-year survival vs. did not reach 2-year survival. (d) Reached DFS vs. did not reach DFS.
Overall, considering the study patients, the median PFS was 21 months (95% CI 17.7, 24.3) overall, 22 (95% CI 18.7, 25.2) months in the PDS group and 18 (95% CI 13.1, 22.8) months in the group receiving NACT and IDS. Data concerning the median OS time were 27 (25–29) months in the entire study population; however, at this time further survival analysis are not reported for the low number of events encountered in the study population. The 2-year survival was obtained in 91% of the patients; 73% were platinum-sensitive (78% in the PDS group and 58% in the NACT group), while DFS was not reached in 19% of the patients (15.3% in the PDS group and 31.6% in the NACT group).
To study HE4 and CA125 serum levels as prognostic factors we chose the following parameters: the median value at the start (HE4 = 374 pmol/L; CA125 = 426 mIU/L), the 75th percentile at the start (HE4 = 1040 pmol/L; CA125 = 1206 mIU/L), 50% reduction of pre-surgical value after surgery, and normalization of the marker levels after the third course of chemotherapy.
The survival analysis was conducted based on the Kaplan–Meier curves, and the Log-rank test was adopted to compare the curves (Figure 2). The duration of PFS was significantly influenced by the values of both HE-4 and CA125 markers before treatment (50th percentile, P=0.0001 and 75th percentile, P=0.0001), and the normalization of marker levels after the third course of chemotherapy (P=0.0001). However, there was an impact of the 50% reduction in HE4 levels after surgical treatment (PDS or IDS, P=0.002). In fact, the 50% reduction in CA125 was not as significant (P=0.089). The analysis of PFS stratified by normalization at the third cycle of the serum level of both HE4 and CA125 showed a significant separation of the curves. This observation was valid from the first months of follow-up (P=0.0001).
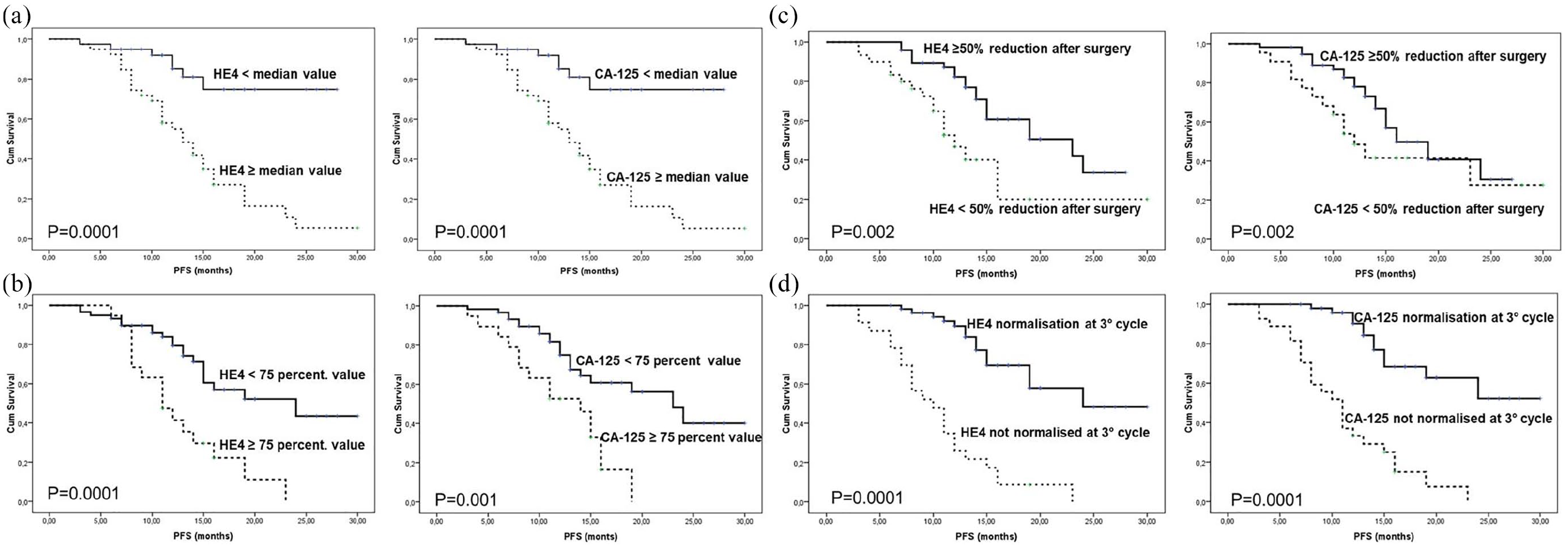
Progression-free survival by HE4 and CA125 serum initial levels and time course. (a) Preoperative serum marker levels median values. (b) Preoperative serum marker levels 75th percentile. (c) 50% reduction of serum marker levels after surgery. (d) Normalization of serum markers at III chemotherapy cycle.
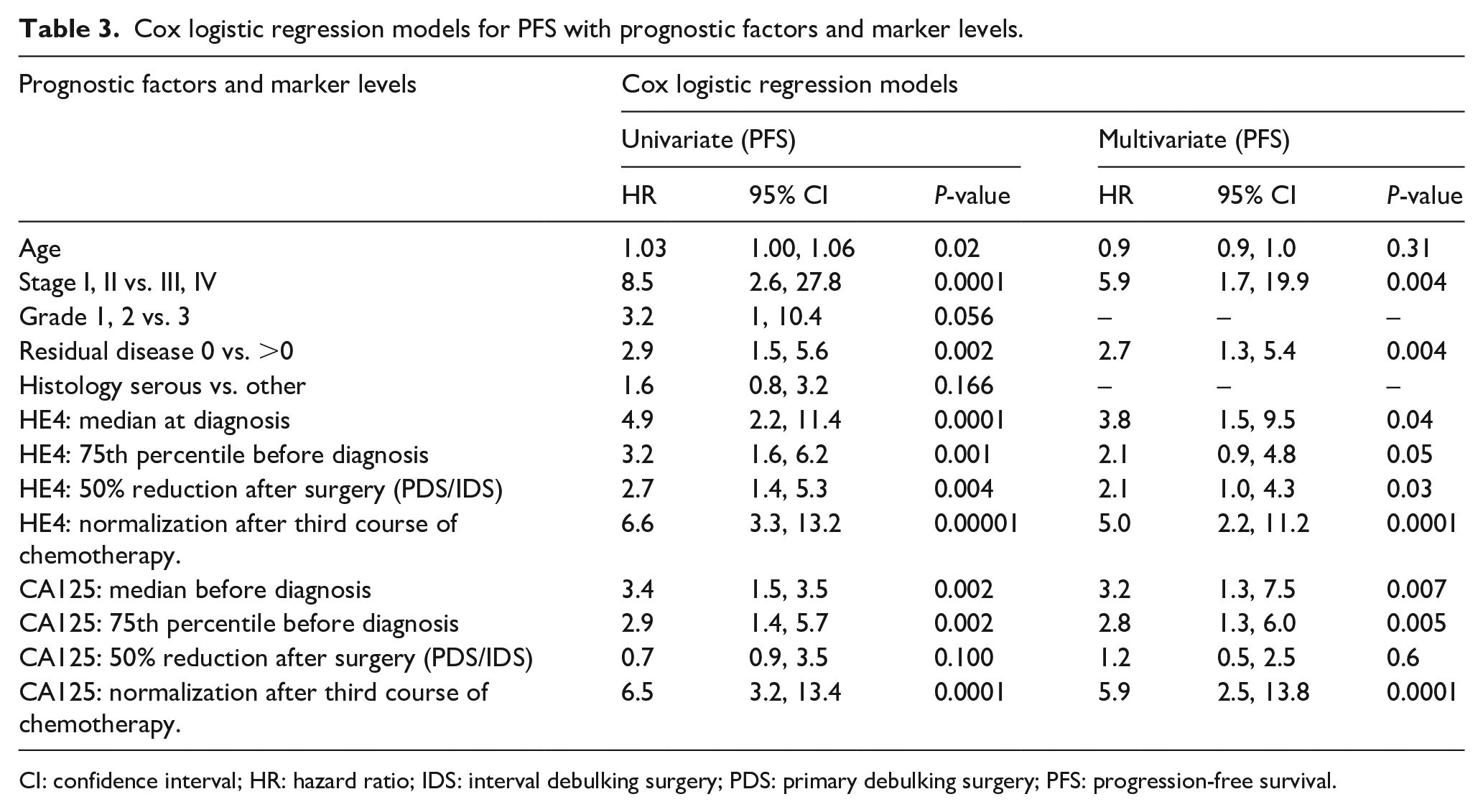
We conducted univariate and multivariate regression logistic analyses according to Mantel-Cox to assess the influence on PFS of prognostic factors, as well as the levels of the HE4 and Ca125 markers measured during the treatment (Table 3). In multivariate analysis only HE4 or CA125 are considered independently to avoid multi-collinearity.
Cox logistic regression models for PFS with prognostic factors and marker levels.
CI: confidence interval; HR: hazard ratio; IDS: interval debulking surgery; PDS: primary debulking surgery; PFS: progression-free survival.
We found in both the univariate and the multivariate analyses that among classical prognostic factors, the residual disease and stage, as expected, wielded the strongest weight on PFS. Among HE4 and CA125 markers, the univariate analysis demonstrated a similarly significant influence on PFS (baseline values above and below the median hazard ratio (HR) = 4.9, P = 0.0001; values above and below 75th percentile—HR = 3.2, P = 0.001; at least 50% reduction before surgery HR = 2.7, P = 0.004) but above all the normalization after the third course of treatment HR = 6.6, P = 0.00001; similar values were found on the univariate analysis for the same parameters with CA125. In the multivariate model stage, shown in Table 3, the values of HE4 and CA125 inserted individually provided good prognostic relevance with the normalization of the marker after third course of treatment (HR = 5.0 and 5.9 respectively, P = 0.00001) and initial values above and under the median level at diagnosis (HR = 3.8 and 3.2 correspondingly, P = <0.05).
Patients undergoing IDS showed no difference in biomarkers decrease between III and IV cycle, because of the longer time interval between the two measurements due to surgery.
Discussion
HE4 is certainly one of the most studied biomarkers in ovarian cancer; however, despite the large number of published studies, the role of this protein has not been established yet. Many studies confirmed the effectiveness of HE4 in the preoperative diagnostics of patients affected by ovarian tumors and verified its specificity. As demonstrated by Ferraro et al. 18 the sensitivity of HE4 and CA125 overlaps (79%), while HE4 exhibits a significantly higher specificity compared to CA125 (93% vs. 78%). They also confirmed that HE4 overcomes CA125 in the diagnosis of ovarian cancer.
In a study of eight patients followed for 20 months after debulking surgery, five women showed a rise in the levels of the tumor markers (HE4 and CA125). In these patients, the rise of HE4 always preceded the CA125 by 5–8 months and coincided with the recurrence of the disease, as confirmed by instrumental examination and by the death of three patients. 7
In our analysis, HE4 has a more rapid decrease rate during chemotherapy than CA125, which has a delay of 21 days, while it seems that HE4 is re-detected faster than CA125 in patients who did not have a good chemotherapy response.
Chudecka-Gøaz et al. 19 showed that the PFS was correlated with the preoperative HE4 values. In our paper, we agree with that analysis: both HE4 and CA125 higher than the median and the 75th percentile are independent factors associated with short PFS and platinum resistance. Furrer et al. 20 showed that a cut-off value at the time of diagnosis of 277 pmol/L for HE4 and 282 IU/mL for CA125 could identify patients affected by EOC with a significantly higher risk of recurrence. In our study, with the consolidated factors that correlated with shorter PFS—RT, FIGO stage, and grading—we found that HE4 and CA125 values at diagnosis (higher or lower than 50th percentile/75th percentile) and the normalization of markers at the third cycle of chemotherapy are clearly related to a longer PFS.
A survival study has not yet been performed because of the short follow-up time and lack of events. We can assert that preoperative plasma HE4 levels might be useful for the clinical management of women with EOC, as it might identify women with worse prognosis. A better knowledge of women’s risk profiles could contribute to the improvement of their follow-up.
Some authors suggest a combination of CA125 and HE4 at a cut-off of 70 pmol/L to improve the overall sensitivity and specificity of CA125 alone, suggesting a useful application of HE4 in strategies for surveillance of ovarian cancer recurrence. 8 In the same way, the association of the two markers is the most effective parameter: during chemotherapy a singularly observed marker has a good prognostic value, but the monitoring of both markers increases the efficacy.
In our study, we can say the usefulness of adding the marker HE4 to CA125 was functional in seven cases (about 9%) that were negative to CA125 at diagnosis and positive to HE4. Furthermore, from the data that can be inferred from the ROC curves, the performance of the HE4, for the considered parameters, is superior.
According to the Kumarasamy et al. 21 review, the possibility of using HE4 as a prognostic marker has not been adequately explored. Looking at the Lan et al. 22 results, the normalization of CA125 level in serum after three cycles of chemotherapy may predict the favorable outcome of patients with advanced ovarian cancer if it was pathologic at the beginning of treatment. In detail, if the RT after primary surgery is good (RT=0 or =0.5 cm) the probability of achieving a complete response after chemotherapy is better when the CA125 serum level is negative after the third course of chemotherapy compared with the patients in which this result is not achieved despite the surgical procedure. 22 According to our study, at the univariate analysis the absence of CA125 normalization at the third cycle correlates with a bad prognosis (OR 6.5 P=0.0001), and the same parameter referred to HE4 has an excellent predictive value (OR 6.6 P=0.0001). These parameters hold on at multivariate analysis (P=0.0001) with stage (OR= 5.9; P=0,004) and residual disease (OR=2.7, P=0.004).
In conclusion, according to our data it can be assessed that—taking into account that HE4 has a higher sensitivity and specificity in the diagnostic phase than CA125—the association of the two markers seems beneficial, or at least HE4 performs well even in the therapeutic monitoring phase. Despite the fact that the single marker trend is a good prognostic factor, the simultaneous evaluation of the two markers showed an overlapping tendency with some advantages in favor of HE4, which is re-detected faster than CA125 in patients who did not have a good response to chemotherapy. For this reason, we decided to include it in the analysis in early stages too in order to check if this trend was applicable despite of the stage of the disease.
Our data should be confirmed by further studies with larger samples and longer follow-up in order to understand the impact of these data on the natural history of ovarian cancer, DFS, and in OS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.