
Abstract
Aim
To investigate the relationship between the serum levels of CEA, CA19-9, CA24-2, CA72-4, and AFP in patients with gastric cancer (GC) and their clinicopathological characteristics; to analyze the efficacy of these tumor markers in evaluating the prognosis of GC.
Methods
Overall, 389 patients with GC either located in the gastric cardia (132), the pyloric antrum (112) or the body of the stomach (145) were included in the study. Serum levels of CEA, CA19-9, CA72-4, and AFP were detected with the ECLIA method, while CA24-2 was measured with ELISA.
Results
First, the serum level of CEA in GC patients with a cardia-located cancer was significantly higher than in patients with pyloric antrum-located cancer (p=0.050). CA72-4 level in patients with GC located in the gastric body was significantly higher than in patients with cardia and pyloric antrum-located cancers (p=0.042 and p=0.039, respectively). Secondly, serum CA19-9 and CA24-2 levels in females with cardia-located GC were significantly higher than those in males with the same type of tumor (p=0.037 and p=0.033, respectively). Additionally, for females with gastric body-located GC the levels of CEA and CA72-4 were significantly higher than those in male patients with the same type of tumor (p=0.047 and p=0.048, respectively). Conversely, in female GC patients with pyloric antrum-located cancer the serum levels of CA19-9 and CA24-2 were significantly lower than those in male patients with the same type of cancer (p=0.013 and p=0.007, respectively). Moreover, CEA, CA19-9, CA24-2, and CA72-4 levels were strongly related to TNM grade and histological anatomy stage, whereas CEA and CA72-4 levels were strongly related to lymph node stage (p=0.000 and p=0.042, respectively). Patients with vascular embolism had higher serum levels of CEA, CA19-9, CA24-2, and CA72-4 compared with patients without vascular embolism (p=0.005, p=0.031, p=0.007, and p=0.014, respectively). In patients with distant metastases and ascites the levels of CEA, CA19-9, and CA24-2 were higher than in patients without these conditions (p=0.003, p=0.001, p=0.001, p=0.016, p= 0.011, and p=0.030, respectively). Serum CEA, CA19-9, and CA24-2 levels showed correlations with tumor invasive depth and growth types (p=0.001, p=0.040, and p=0.035, respectively). Patients with lump and catheter tumor growth types had significantly higher AFP levels than patients with invasion and anabrosis growth types (p=0.034 and p=0.005, respectively). Tumor size was correlated with the preoperative serum levels of CEA, AFP, and CA72-4 (p=0.007, p=0.020, and p=0.008, respectively). Additionally multiple linear regression analysis showed that preoperative levels of CEA and CA72-4 were correlated to TNM stages, CA19-9 and CA24-2 levels were correlated to both gender and distant metastasis, and AFP was correlated only to ascites. During follow-up there were 115 deaths. Median survival time for GC patients with negative preoperative CEA was 18.07 months, and was 10.97 months for patients with preoperative CEA positive levels (p=0.0005). Similarly, the median survival time for GC patients with negative preoperative CA72-4 was 33.60, and was 16.03 months for patients with preoperative CA72-4 positive levels (p=0.0041).
Conclusions
The preoperative levels of CEA, CA19-9, CA24-2, CA72-4, and AFP were closely related to TNM grade, gender, distant metastasis and ascites. These makers seem to play important roles in predicting recurrence and metastasis, and in evaluating prognosis.
Introduction
Gastric cancer (GC) is a disease with high mortality and high death rates. Two-thirds of the GC cases occur in developing countries. Among these, 42% of the cases are located in China, predominantly in villages; in these cases most patients are diagnosed already at advanced stages of the disease. It's important to find the simple and feasible markers to diagnosis and monitor the gastric cancer. Clinical evidence and recent research indicate the high diagnostic sensitivity and specificity of some tumor markers, including CEA, CA19-9, CA24-2, CA72-4, and AFP, that have been found in digestive tract, lung and ovary carcinomas (1-13). Moreover, these markers strongly correlated with tumor recurrence and metastasis (14-21). However, the combination of these 5 tumor markers has not been used to perform clinical assessment and prognostic evaluation of GC. In this study, the abovementioned tumor markers were measured in GC patients at specific intervals during postoperative follow-up as to assess the main clinicopathological characteristics affecting preoperative marker levels, as well as to establish whether the measurement of these markers could help in monitoring tumor recurrence and metastasis, and assessing of prognosis.
Materials and Methods
Patients
This study included 389 patients who underwent surgical resection for primary GC between August 2005 and January 2008. No main organ dysfunction was found in these patients and normal bone marrow, liver and renal functions were assessed for inclusion in the study. The median patients’ age was 57.9 years (range, 22-80 years). Patients’ characteristics are presented in Table I. All patients were divided into 4 groups representing their tumor staging, assessed according to the international Tumor Node Metastasis (TNM) staging system.
Patient And Disease Characteristics
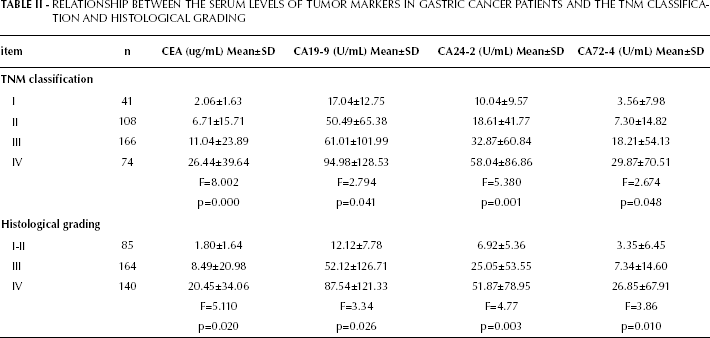
Relationship Between The Serum Levels Of Tumor Markers In Gastric Cancer Patients And The Tnm Classification And Histological Grading
Follow-up
Follow-up examination was performed once per trimester after surgical resection for the first year, and every semester for the years thereafter. The follow-up program included: clinical examination, hematological analyses, and tumor marker assay at each checkup; abdominal ultrasound and chest x-rays were scheduled every 6 months. In case of recurrence, diagnosis of the site of recurrence was established on basis of clinical and instrumental examinations. The follow-up end-date was June 30, 2011. All surviving patients were followed up for at least 3 years. Thirty-one patients died of postoperative complications or causes other than tumor recurrence during follow-up, and 36 patients, who interrupted the follow-up program, were excluded from the final evaluation. Ultimately, 322 patients were included. Of those, 244 were males and 78 females.
Tumor marker assay
The tumor markers CEA, CA19-9, CA24-2, CA72-4, and AFP were measured prior to surgery and at every follow-up examination. Serum samples from GC patients were collected and then centrifuged for 10 minutes at 3,000 rpm; serum was then immediately separated for examination.
Serum CEA, CA19-9, CA72-4, and AFP levels were measured by commercial electrochemiluminescence immunoassay (ECLIA) using Cobas 601 and reagent kits (Roche Diagnostics, Mannheim, Germany); CA24-2 levels were detected by ELISA using the FUJIREBIO diagnostics kit. The cutoff values of these tumor makers were previously established by our laboratory by taking into account several environmental factors (among which diet, living conditions and patient selection). Thus, cutoff values were set as follows: 3 ug/mL for CEA, 20 U/mL for CA19-9, 12 U/mL for CA24-2, 7 U/mL for CA72-4, and 15 ug/L for AFP.
Statistical analyses
Statistical analysis was performed using the SPSS 13.0 software. All data here reported are expressed as mean ± SD. Non-parametric tests were used for comparisons of numeric variables, differences in markers’ serum levels were evaluated by Kruskal-Wallis test, survival was estimated by the Kaplan-Meier method, and differences in survival were determined by the log-rank analysis. A p value <0.05 was considered significant.
Results
Figure 1 shows that CEA levels (16.73±28.29 ug/mL) in cardia-located GC were significantly higher than those of tumors located in the pyloric antrum (8.79±22.18 ug/mL, p=0.050). Similarly, CA72-4 levels in gastric body-located GC (26.88±72.82 U/mL) were significantly higher than those of tumors in the pyloric antrum (11.57±23.49 U/mL, p=0.042) and cardia (12.56±31.41 U/mL, p=0.039).
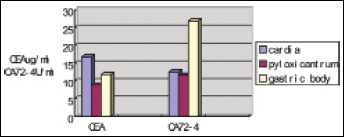
Comparison of the tumor markers in serum among the GC locater in cardia, pyloric antrum, and body of the stomach.
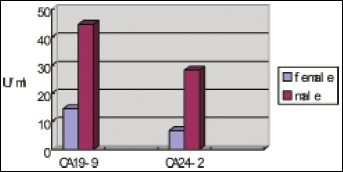
Figure 2 shows that CA19-9 and CA24-2 serum levels in females with cardia-located GC were significantly higher (105.23±129.27 U/mL and 73.79±95.88 U/mL, respectively) than their respective levels in males (38.19±74.68 U/mL and 23.18±46.26 U/mL; p=0.037 and p=0.033, respectively). Conversely, CA19-9 and CA24-2 levels in females with pyloric antrum-located GC were significantly lower (14.51±19.35 U/mL and 6.77±6.33 U/mL) than their respective levels in males (44.50±79.29 U/mL and 28.20±55.11 U/mL; p=0.013 and p=0.007, respectively) (Fig. 3).
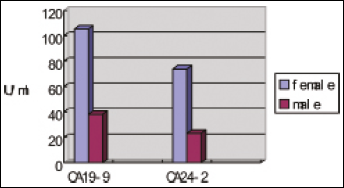
Comparison of the levels of CA19-9 and CA24-2 in female and male patients with cardia-located GC.
Comparison of the levels of CA19-9 and CA24-2 in female and male patients with pyloric antrum-located GC.
CEA and CA72-4 serum levels in females with gastric body-located GC were significantly higher (21.53±43. 98 ug/mL and 32.32±34.45 U/mL) than their respective levels in males (8.01±20.90 ug/mL and 12.86±20.15 U/mL; p=0.047 and p=0.048, respectively) (Fig. 4).
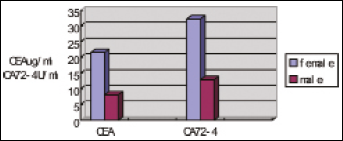
Comparison of the levels of CEA and CA72-4 in female and male patients with GC located in the gastric body.
Stratified analysis showed that CEA, CA19-9, CA24-2, and CA72-4 were significantly correlated to TNM grade and histological anatomy stage. Conversely, no difference was found among the same groups for the AFP levels (Tab. I).
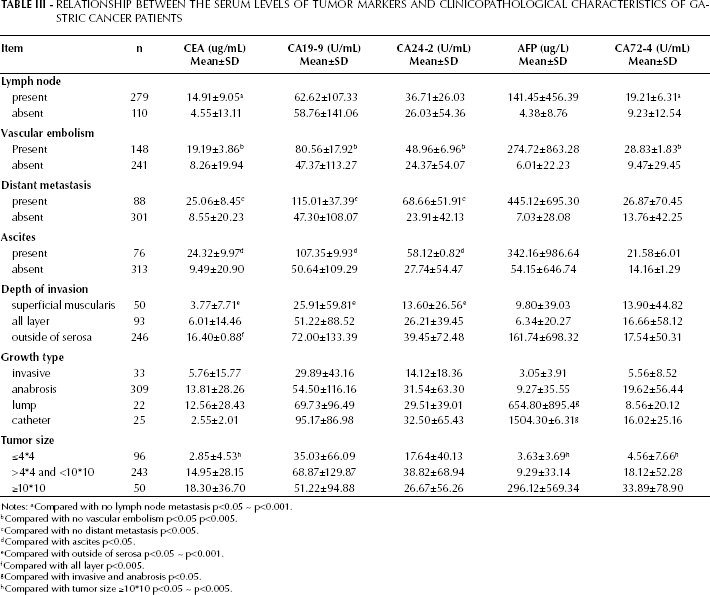
The patients’ clinicopathological and surgical features are shown in Table III. CEA and CA72-4 serum levels were significantly higher in patients with lymph node metastasis than without. Additionally, CEA, CA19-9, CA24-2, and CA72-4 levels in patients with vascular embolism were significantly higher than those without vascular embolism. CEA, CA19-9, and CA24-2 levels in patients with distant metastasis were significantly higher than in healthy controls. CEA, CA19-9, and CA24-2 levels in patients with ascites were significantly higher than in patients with no ascites. With regard to the depth of tumor invasion, CEA, CA19-9, and CA24-2 levels in tumors of the superficial muscularis were significantly lower than those of the serosa. AFP levels in lump and catheter growth types were significantly higher than invasion and anabrosis types. Tumor size was strongly correlated with the serum levels of CEA, AFP, and CA72-4.
Relationship Between The Serum Levels Of Tumor Markers And Clinicopathological Characteristics Of Gastric Cancer Patients
Notes:
Compared with no lymph node metastasis p<0.05 ~ p<0.001.
Compared with no vascular embolism p<0.05 p<0.005.
Compared with no distant metastasis p<0.005.
Compared with ascites p<0.05.
Compared with outside of serosa p<0.05 ~ p<0.001.
Compared with all layer p<0.005.
Compared with invasive and anabrosis p<0.05.
Compared with tumor size ≥10*10 p<0.05 ~ p<0.005.
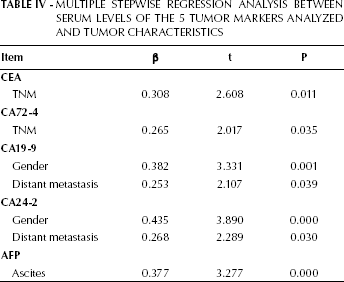
Multiple regression analysis showed that the preoperative levels of CEA and CA72-4 were correlated to the TNM grade, whereas the levels of CA19-9 and CA24-2 were correlated to gender and distant metastasis and, finally, AFP levels were correlated to the presence of ascites (Tab. IV).
Multiple Stepwise Regression Analysis Between Serum Levels Of The 5 Tumor Markers Analyzed And Tumor Characteristics
Overall 115 patients died during the follow-up period. The levels of tumor markers generally increased during follow-up while metastasis and deterioration increasingly occurred. The longest time interval between the increasing levels of the tumor markers and the appearance of the imaging features was 124 days. Median survival time for GC patients with negative preoperative CEA was 18.07 months, and was 10.97 months for patients with preoperative CEA positive levels (p=0.0005). Similarly, the median survival time for GC patients with negative preoperative CA72-4 was 33.60, and was 16.03 months for patients with preoperative CA72-4 positive levels (p=0.0041).
Discussion
GC is one of most common forms of cancer worldwide. In China, the mortality and incidence rates for GC are about twice as high as the world average level. The male/female incidence ratio is approximately 1.5-2.5. GC incidence increases with age; however, increasing numbers of young patients are being diagnosed with GC. GC is more common in the remote areas of the Shanxi province, in China. At the time of diagnosis patients had an advanced stage GC, which differed in terms of regional metastasis and ascites status. Tumor markers have been used for the early diagnosis of GC (20, 22-32), the assessment of treatment effectiveness and the monitoring of recurrences (12, 25, 33, 34). However, each tumor marker has its limitations in terms of diagnostic value, especially for the early diagnosis (35-37). It is therefore necessary to find new molecules and combine the testing of several of these tumor markers at the same time (13, 38-40).
In our study, we detected the serum levels of CEA, CA19-9, CA24-2, CA72-4, and AFP as to evaluate their efficacy in diagnosing GC, monitoring of tumor recurrence and metastasis, and assessment of prognosis. Our results showed that CEA, CA19-9, and CA72-4 serum levels strongly correlated with the degree of malignancy, generation, progress, invasiveness, and metastatic status of GC (15, 16, 18, 41-43). Thus, these markers may be used as predictors of early recurrence and metastasis (44-48). The direct association between lymph node involvement and hematogenous metastases from GC has been described in other studies (49, 50).
Additionally, we found that tumor marker levels were affected by the tumor location. CEA level in cardia-located GC was higher than that in pyloric antrum-located GC, whereas CA72-4 levels in gastric body-located GC were higher than those in antrum or cardia-located cancer. To our knowledge, there is no other study in the literature reporting similar analyses.
Our results showed that while in cardia-located GC the CA19-9 and CA24-2 levels were higher in female patients than in males, the levels of these same markers were reversed in gastric antrum-located cancers. Our results also showed that CA19-9 and CA24-2 levels in male patients were higher than in females, and this may be caused by the unequal gender ratio characterizing our study (males/females 1:2.6). On the contrary, CEA and CA72-4 levels in female patients were higher than in male patients. It is well known that CEA and CA72-4 levels are correlated to prognosis of GC patients and this may probably explain why female patients had worse outcomes and shorter survival times.
Stratified analysis showed that, unlike AFP, the serum levels of CEA, CA19-9, CA24-2, and CA72-4 were related to TNM stage and histological anatomy grade (1, 15, 18, 30, 51-55). The levels of these markers increased according to the progression of the tumor and were related to the burden of the tumor. Further analysis showed that AFP serum levels may correlate with ascites and that high AFP levels may predict peritoneum and liver metastasis (22, 56-60). Therefore, among the markers we studied, AFP was the best indicator of early peritoneum metastasis and liver metastasis in GC patients.
It has been reported that serum CEA, CA19-9, and AFP levels have been used to diagnose and monitor cancer recurrence and liver metastasis of GC (40, 48, 50, 61, 63). Ucar et al (12) reported that CEA levels were related to liver metastasis of GC, and that patients with lymph node metastasis or invasion depth beyond the serosa had increased CA19-9 levels. Additionally, the same study reported that the CA72-4 levels were related to all the 3 abovementioned factors, and that CA72-4 was the only marker that correlated with the 3-year accumulative survival rate (18, 54, 55, 64-67). Our findings that patients with lymph node metastasis had higher CEA and CA72-4 levels are supported by Fernandes et al (1) and Gora et al (39, 68, 69). While the high CEA, CA19-9, CA24-2, and CA72-4 levels were found in patients with cancer embolus, CEA, CA19-9, and CA24-2 levels increased along with tumor progressing (65, 71-74). We also found that tumor size affected the levels of tumor markers, as CEA, CA72-4, and AFP levels were significantly higher in larger tumors (≥10cm) than in smaller ones (≤4cm). In addition, the AFP levels were dramatically higher in lump and catheter GC, whereas the other markers considered did not change in relation to the tumor growth type.
Stepwise regression analysis showed that preoperative serum levels of CEA and CA72-4 were correlated with clinical stages, and both markers were indicators of poor prognosis (54, 55, 66, 67). The elevated levels of the tumor markers appeared earlier than the positive imaging results when the tumor recurred, with the longest interval being of 124 days. Therefore, these tumor markers could play an important role in the monitoring of tumor recurrence and metastasis, thus allowing identifying symptomless patients with tumor recurrence by routine postoperative serum checkups.
In summary, a combined test for CEA, CA19-9, CA24-2, CA72-4, and AFP levels may improve sensitivity of GC patients (75, 76). This study indeed shows that these specific tumor markers, examined postoperatively during follow-up, were useful to find early tumor recurrence and metastasis, and evaluate prognosis.