
Abstract
Background
E-selectin is an adhesion molecule expressed on activated endothelial cells. E-selectin plays an important role in the process of inflammation and is also involved in the mechanism of cancer metastasis regulating the adhesion of circulating cancer cells to the blood vessels. The aim of our study was to determine whether an association exists between its most common gene polymorphism, S128R, and gastric cancer (GC).
Methods
We performed a case-control study of 88 GC cases and 480 controls to analyze the association between E-selectin S128R gene polymorphism and GC susceptibility. The genotyping analysis was done by PCR-restriction fragment length polymorphism method.
Results
The E-selectin S128R C allele, CA and CC genotypes were over-represented among the GC cases. No statistically significant association was observed between E-selectin S128R polymorphisms and tumor characteristics. However, carrying the C allele was associated with poor survival.
Conclusions
The E-selectin S128R C allele may confer an increased susceptibility to gastric cancer development and correlate with a poor prognosis.
Introduction
Gastric cancer (GC) is the fourth most common cancer and the second leading cause of death due to cancer worldwide. In 2008, more than 990,000 cases were recorded (7.8% of which were new cancers) with 738,000 deaths. More than two thirds of GC occurs in developing countries (1, 2). Carcinogenesis of GC is a complex and multifactorial process, in which genetic and environmental factors are involved. Environmental factors, such as Helicobacter pylori infection, may cooperate with genetic polymorphisms in an unknown manner, playing an important role in cellular immortalization and tumorigenesis (3, 4). On the other hand, the role of the immune system, by means of a large number of different molecules, is crucial for the maintenance of a healthy condition. In this context, many single nucleotide polymorphisms (SNPs) in proinflammatory and immunoregulatory genes are known, suggesting their role in tumor initiation and progression (5-7).
Selectins are cell adhesion molecules mediating the binding of leukocytes to the microvascular endothelium, and include 3 members: E-, P-, and L-selectin. E-selectin is expressed by endothelial cells as a response to cytokines. During inflammation, E-selectin plays an important role in recruiting leukocytes to the site of injury (8). E-selectin is correlated with the metastatic potential of malignant cells (9).
Several polymorphisms have been described within the E-selectin gene. The S128R gene polymorphism is the most common polymorphism in the Caucasian population (10-11). This polymorphism results in the substitution of a serine by an arginine at position 128 within the extracellular domain of the receptor, and enhances the adhesion of lymphocytes and myeloid cells to endothelial cells (12-14). The S128R polymorphism has been found to be associated with essential hypertension, inflammatory bowel disease, and atherosclerosis, which exhibit an increased interaction between endothelial cells and leucocytes (14-16). In addition, the role of S128R polymorphism has been studied in colon cancer and pancreatic cancer (17, 18). However, little is known about the consequences of the E-selectin variants in patients with GC (19).
In the present study, we tested and affirmed the hypothesis that the frequency of the S128R polymorphism is significantly higher in patients with GC compared to healthy controls.
Materials and Methods
Patients
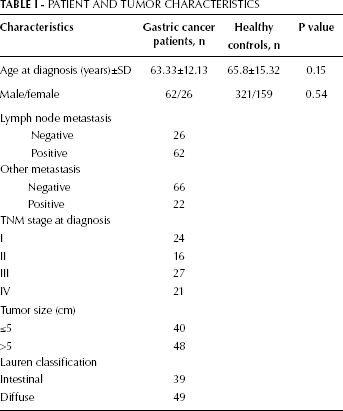
The subjects in this hospital-based case-control study were 88 unrelated GC patients and 480 healthy individuals (controls) matched for ethnicity, sex and age. All patients and controls were born and have been living in Greece. All patients gave their informed consent and the hospital review board approved the study. The patients were followed up until August 2010 or death. The median time ± standard deviation (SD) of follow-up was 36.27±19.5 months. Seventeen patients were lost to follow-up. The characteristics of the GC patients at diagnosis are presented in Table I.
PATIENT AND TUMOR CHARACTERISTICS
Genotyping
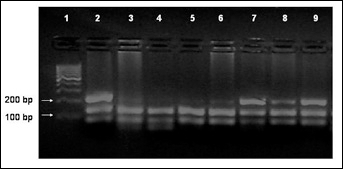
Genomic DNA was isolated from GC patients' paraffin-embedded cancer tissues and from peripheral blood of healthy individuals using NucleoSpin Tissue Kit (Macherey-Nagel, GmbH & Co. KG, Düren, Germany) according to the manufacturer instructions. Genotyping analysis was performed using PCR-restriction fragment length polymorphism (RFLP) method. The following primers were used: 5′-AAA ATC AAA GGC ACT CAG TAT AAG CA-3′ (in the forward direction) and 5′-GAA CGT GAG ATG GTG CTA CCA-3′ (in the reverse direction). The PstI restriction enzyme was used for genotyping by PCR-RFLP. The products were analyzed by electrophoresis in a 2% agarose gel and visualized using UV fluorescence after staining with ethidium bromide.
Statistical analysis
Statistical calculations were performed using the SPSS for Windows software package (SPSS, Inc., Chicago, IL, USA). Frequency and susceptibility of the polymorphism were compared with the chi-square (χ 2 ) test. Odds ratios (OR) and 95% confidence intervals (95% CI) were calculated with the corresponding χ 2 distribution test. The p values obtained were 2-tailed and significance was assumed for p values below 0.05. Hardy-Weinberg equilibrium was verified by calculating the expected frequencies and numbers and was tested using the goodness-of-fit χ 2 -test in patients and controls separately.
Results
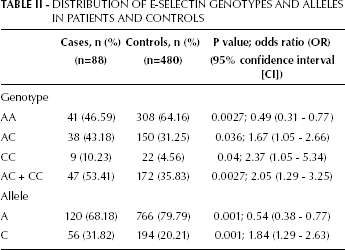
The histological characteristics of the patients are presented in Table I. Lymph node metastases were present in 70.45% of the patients. Only 22 patients (25%) suffered from distant metastases. The E-selectin genotypes and allele distribution among patients and healthy controls are presented in Figure 1 and Table II. The observed genotype frequencies were in accordance with the Hardy-Weinberg equilibrium. The frequencies of the AA, CA, and CC genotypes were respectively 46.59%, 43.18%, and 1.023% in patients, and 64.16%, 31.25%, and 4.56% in healthy controls. Genotype frequencies and allelic distribution were different between GC cases and controls. The patients that were C-carriers (AC+CC genotypes) and the C allele were over-represented among the GC cases (respectively p=0.0027 and p=0.001) (Tab. II).
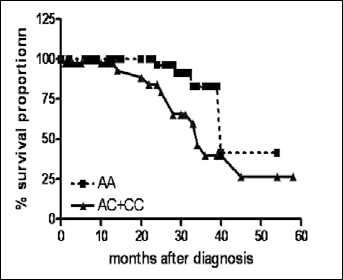
Kaplan-Meier survival curves for GC patients stratified by E-selectin S128R genotypes.
DISTRIBUTION OF E-SELECTIN GENOTYPES AND ALLELES IN PATIENTS AND CONTROLS
Concerning the tumor characteristics, no statistically significant association was observed between E-selectin polymorphism and any parameter investigated (metastasis, TNM stage and Lauren classification).
Follow-up information regarding survival was available for all patients (Tab. III). The median duration of the follow-up was 36.27 months (range 1-60 months). Among GC patients we recorded a total of 17 cancer-related deaths during the follow-up period. The hazard ratios for patients with the E-selectin S128R genotype for overall specific survival are presented in Table III. Carrying the C allele (AC+CC genotypes) seemed to be associated with poor survival (Fig. 2).
E-SELECTIN S128R GENOTYPES IN ASSOCIATION WITH GC OVERALL SURVIVAL
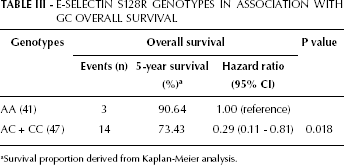
Survival proportion derived from Kaplan-Meier analysis.
Representative gel of RFLP-PCR for E-selectin S128R variants. Lanes 2, 7-9 represent heterozygous patients and lanes 3-6 represent homozygous AA patients.
Discussion
The E-selectin S128R polymorphism has been demonstrated to have functional implications in terms of adhesiveness to endothelial cells. In a recent study, S128R E-selectin-transfected endothelial cells supported increased adhesion and cellular signaling of T84 colon cancer cells (20). The most compelling evidence for the role of E-selectin polymorphism in malignancies comes from previous studies showing that this specific polymorphism is associated with susceptibility to pancreatic cancer (18) and metastasis formation in colon cancer (17, 20). In the current study, we attempted to determine whether an association exists between this E-selectin gene S128R polymorphism and GC. Our data showed that the AC and CC genotypes were significantly associated with GC risk. Our results are in agreement with recent a study by Xia et al (19) that suggest that E-selectin C-variant, as well as FCGR2A variant rs1801274, were both significantly associated with GC risk in a sample of the Chinese population. Patients with the C allele are at risk of having higher tumoral adhesiveness to endothelial cells and are more likely to develop metastases. In our study, only 25% of the patients developed distant metastases. However, no significant effect was observed between the studied polymorphism and the metastatic potential of the GC cases. E-selectin is an adhesion molecule expressed by vascular endothelial cells that are involved in adhesion and in Helicobacter pylori-based gastric lesions (21).
Even if the role of E-selectin in GC remains controversial (22), recent data suggested that elevated serum concentrations of E-selectin would be proportional to poorer prognosis in GC (23), colorectal cancer (24), as well as papillary thyroid cancer (25) and could reflect the therapeutic outcome of GC (26). Our results indicate that the carriers of the C allele had a poor prognosis, however the number of events in our cohort was very small. From our study, no clear indication exists of whether this allele relates to E-selectin expression levels. Three are the potential mechanisms by which E-selectin can be associated with progression and invasion of GC: (i) the ligands sialyl-Lewis A or sialyl-Lewis X that enable crucial interactions in the occurrence of distant metastases; (ii) the carcinoembryonic antigen (CEA) that has been identified as an E-selectin ligand; (iii) the induction of angiogenesis mediated by the Src-PI3K pathway (19). The influence of the E-selectin gene polymorphism in GC carcinogenesis may have different effects among the malignant cases in terms of mediation of tumor progression, angiogenesis, metastasis, and leukocyte migration. Besides the imbalance in regulatory pathways due to the activation of oncogenes or loss of tumor suppressor genes, cancer progression and clinical outcomes may be greatly modulated by the functional alteration of key proteins often determined by genetic polymorphisms (27). The issue concerning the influence of the E-selectin genotype and allele on GC development and progression remains open as long as the functional importance of the minor allele in the expression of the E-selectin transcript and protein are largely obscure. Like most human cancers, GC must be viewed as a disease with a polygenic background where oncogenes, tumor suppressor genes, and signaling pathways all play a role.
In conclusion, in the present study, we report that E-selectin S128R C allele may confer an increased susceptibility to GC development and may correlate with a poor prognosis. Further investigations in larger cohorts of the molecular mechanisms associated with the E-selectin polymorphism may provide a better understanding of the development of GC and contribute to the identification of novel predictors and prognostic factors for GC.