
Abstract
Psychological accounts of symptom perception put forward that symptom experiences consist of sensory-perceptual and affective-motivational components. This division is also suggested by psychometric studies investigating the latent structure of symptom reporting. To corroborate the view that the general and symptom-specific factors of a bifactor model represent affective and sensory components, respectively, we performed bifactor models applying confirmatory factor analytic approaches to the Patient Health Questionnaire-15 and the Checklist for Symptoms in Daily Life completed by 1053 undergraduate students. Additionally, we explored the association of latent factors with negative affectivity (NA). For both questionnaires, a bifactor model with one general and several symptom-specific factors revealed the best fit to the data. NA yielded large associations with the general factor, but smaller ones with somatic symptom-specific factors in both questionnaires. The observed latent structure supports a distinction between sensory-perceptual and affective-motivational components, and the association between the NA and the general factor confirms the affective tone of the latter.
Keywords
Introduction
Symptom perception relies on a complex and constructive integration of multiple sources of information whereby interoceptive (bottom-up) information from within the body interacts with cognitive-affective (top-down) processes, such as attention, expectations, memory, and beliefs (R. J. Brown, 2004; Rief & Broadbent, 2007; Van den Bergh, Witthöft, Petersen, & Brown, 2017). Neurobiological models of interoception (Craig, 2003) have suggested that different structures in the brain process sensory-perceptual and affective-motivational components of a somatic experience. The first component conveys the distinct details about the intensity and spatiotemporal characteristics of internal sensations, whereas the latter component includes the feelings associated with the sensations, reflecting a behavioral drive to adjust (to) the stimulus. Bodily symptoms can therefore be seen as “homeostatic emotions” necessary to maintain the integrity of the body (Craig, 2003), in which the affective evaluation that is associated with sensory information depends on the state and the needs of the organism. For example, drinking may be associated with different levels of pleasantness depending on the degree of thirst.
The importance of the sensory-perceptual and the affective-motivational components of a somatic experience may also be reflected in psychometric research, which explores the latent structure of somatic symptom reports. The latent structure can be specified by various measurement models, which include: (a) a one-factor model, in which all items load on one factor; (b) a correlated group-factor model comprising correlated symptom-specific factors (e.g., a pain factor, a cardiorespiratory factor); (c) a hierarchical model, in which the associations between the lower-order symptom-specific factors are accounted for by a higher-order general factor; and (d) a bifactor model, which consists of a general symptom factor and several symptom-specific factors. The bifactor model was recently shown to yield the best model fit for the latent structure of somatic symptoms assessed by the Patient Health Questionnaire-15 (PHQ-15) (Kroenke, Spitzer, & Williams, 2002) in various samples, including college students (Witthöft, Fischer, Jasper, Rist, & Nater, 2016), the general population, and primary care patients (Witthöft, Hiller, Loch, & Jasper, 2013). Also the latent structures underlying symptoms of the irritable bowel syndrome (Jasper, Egloff, Roalfe, & Witthöft, 2015) and functional dyspepsia (Van Oudenhove et al., 2016) yielded a bifactor model with a general somatization factor and three symptom-specific factors, outperforming other models.
In the bifactor model, each symptom shares both general and specific components of systematic variance (Reise, 2012). In other words, each symptom is explained by two latent factors: a general factor and orthogonal symptom-specific factors. The abovementioned studies not only showed that the bifactor model outperforms other models, but also suggested a possible meaning of those latent (general and symptom-specific) factors. In particular, the general factor may refer to the affective component of symptom experience, whereas the symptom-specific factors are related to the sensory-perceptual features. This is suggested by a strong relationship between the general factor and psychological constructs, such as health anxiety, somatosensory amplification, and somatoform dissociation (Jasper et al., 2015; Witthöft et al., 2016); symptom-specific factors, on the other hand, do not show such a relationship.
One of the important individual differences associated with a propensity to report frequent occurrences of physical symptoms is negative affectivity (NA). NA is a tendency to experience negative mood or affect and to perceive situations as threatening (Watson & Pennebaker, 1989). A robust association of trait NA and symptom reporting is typically observed, varying around r = .50 in both clinical (Kroenke, 2003; Wessely, Nimnuan, & Sharpe, 1999) and non-clinical populations (Van Diest et al., 2005). However, differences in strength of the association with NA exist among symptoms: stronger associations are observed with vague, systemic complaints and with symptoms that are more severe and distressing (Van Diest et al., 2005). The different strengths of the relationship between NA and individual symptoms suggest that investigating its association with the latent factors in the somatic symptom bifactor model may provide more evidence for the construct validity of this model and help clarifying the meaning of the factors. Because previous findings showed associations between the general factor and psychological constructs (Jasper et al., 2015; Witthöft et al., 2016), a strong relationship would also be expected between this factor and NA as a broad trait overarching specific symptom-related concerns and worries. However, the association of the latent structure underlying symptom reports with NA has hitherto not been formally tested.
The primary goals of this study were to replicate the latent structure of symptom reporting as previously found, and to explore the construct validity of the proposed latent variables by examining their association with trait NA. To this end, the latent structure of symptom reporting was first investigated with two symptom questionnaires: the previously used PHQ-15 (Kroenke et al., 2002) and the Checklist for Symptoms in Daily Life (CSD). The CSD is a self-report symptom inventory measuring habitual symptom reporting. It assesses the frequency of a broad range of everyday complaints and comprises a number of symptoms not included in the PHQ-15, such as respiratory, neurological, and psychological symptoms. Four different models were compared: a one-factor model, a correlated group-factor model, a hierarchical model, and a bifactor model. The best fit was expected for the bifactor model consisting of both the general symptom reporting factor, which is related to every symptom, and the orthogonal symptom-specific (e.g., cardiopulmonary, gastrointestinal) factors representing the unique variance components of the extracted subscales of the questionnaires. Second, the association between the general and symptom-specific factors of both questionnaires and the trait NA was explored to investigate the construct validity of the proposed latent structure. Following the assumption that the general factor represents the affective component of symptom reporting, we proposed that NA would show a stronger association with the general factor of both the CSD and the PHQ-15, compared to the symptom-specific factors.
Method
Participants and procedure
Data were collected during three collective sessions among three cohorts of first-year undergraduate psychology students (N = 1053; 83% women; mean age = 18.69, SD = 2.61) from the University of Leuven, Belgium. Students completed online a battery of questionnaires in return for course credit. Questionnaires included in the present study were displayed at the beginning of the session. The collective sessions took place at the start of each academic year and included only the freshmen of that year. Data used in this study are from the collective sessions of 2013 (n = 313), 2014 (n = 370), and 2015 (n = 370). All group testing sessions were approved by the Multidisciplinary Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Leuven.
Measures
Patient Health Questionnaire-15 (PHQ-15)
The PHQ-15 (Kroenke et al., 2002) is a widely used self-report questionnaire measuring the distress related to 15 somatic symptoms over the previous 4 weeks. The 3-point scale ranges from 0 (not bothered at all) to 2 (bothered a lot). The Dutch version was used (van Ravesteijn et al., 2009). Cronbach’s α in the present sample was .72.
Checklist for Symptom in Daily Life (CSD)
The CSD is a self-report measure of habitual symptom reporting based on the Psychosomatic Symptom Checklist (Wientjes & Grossman, 1994). It comprises a broad range of everyday complaints from various modalities (e.g., breathlessness, nausea, headache; see Table S1 in Supplementary Materials for the full list of symptoms). Four items (stuffy nose, low back pain, join pain, burning feeling in the eyes) were added to the original checklist. The frequency of 39 symptoms in the past year is assessed on a 5-point scale (1 = never, 2 = seldom, 3 = sometimes, 4 = often, 5 = very often). This scale was previously used to screen for habitual symptom reporting in daily life (Bogaerts et al., 2015; Bogaerts, Janssens, De Peuter, Van Diest, & Van den Bergh, 2010; Constantinou, Bogaerts, Van Diest, & Van den Bergh, 2013; Constantinou, Van Den Houte, Bogaerts, Van Diest, & Van den Bergh, 2014; Walentynowicz et al., 2018; Walentynowicz, Bogaerts, Van Diest, Raes, & Van den Bergh, 2015; Walentynowicz, Van Diest, Raes, & Van den Bergh, 2017). In the present sample Cronbach’s α was .92.
Positive and Negative Affect Schedule (PANAS)
The Dutch version (Engelen, De Peuter, Victoir, Van Diest, & Van den Bergh, 2006) of the PANAS (Watson, Clark, & Tellegen, 1988) was used. This instrument assesses to what extent 10 positive and 10 negative adjectives apply to participants’ feelings in general on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much). For the present study, only scores on Negative Affectivity scale (NA; 10 items) were investigated. Cronbach’s α in the present sample was .88.
Data analysis
Analyses were performed with Mplus 7 software (Muthén & Muthén, 2012). For the PHQ-15 dataset, confirmatory factor analyses (CFA) were performed to test four models (Witthöft et al., 2016; Witthöft, Hiller, et al., 2013) (Figure 1): a one-factor model (Model 1); a correlated group-factor model (Model 2) comprising four first-order factors; a hierarchical model (Model 3), which included a second-order factor in addition to the four first-order factors; and a bifactor model (Model 4). In the bifactor model, the items’ loadings on the general factor and on one of the four specific factors are estimated, while other loadings are constrained to be zero. In addition, the bifactor model requires that all factors are set to be orthogonal, that is, the correlations between the specific factors and between the specific factors and the general factor are fixed to zero (Reise, Moore, & Haviland, 2010). As in the previous CFA analyses of the PHQ-15 (Witthöft et al., 2016; Witthöft, Hiller, et al., 2013), two items were excluded from the analyses because of a very low base rate (fainting spells) and a gender-specific content (menstrual problems).

Graphical representation of the models considered in this study. Models 1-4 were tested for both the Patient Heath Questionnaire-15 (PHQ-15) and the Checklist for Symptoms in Daily Life (CSD). Model 5 was tested only for the CSD. ESEM = exploratory structure equation model; G = general factor; A1-A3, B1-B3, C1-C3, and D1-D3 = items; F1-F4 = factors. Squares represent observed variables and ovals represent latent factors. Full unidirectional arrows represent the main factor loadings; dotted unidirectional arrows represent cross-loadings in a bifactor ESEM.
Due to the fact that the factor structure of the CSD has not been previously explored, the analytic strategy for this dataset followed a different path. First, the items showing content overlap with negative affectivity (tenseness, feeling anxious, feeling of panic, feeling confused, and fits of crying) were removed from the analysis. Second, the parallel analysis method (Hayton, Allen, & Scarpello, 2004; Horn, 1965) was used to determine the number of meaningful factors to be extracted from the exploratory factor analysis (EFA). In this procedure, random data sets with the same number of variables and observations as the real data set are generated. The eigenvalues extracted from those random data sets are averaged and compared to the empirically-observed eigenvalues. In this study, the random eigenvalues were averaged across 1000 random data sets. The factors were retained when their eigenvalues from the raw data were greater than those from the random data. Parallel analysis favored a four factor solution with eigenvalues of 8.89, 2.15, 2.08, and 1.36 exceeding the eigenvalues of the random data, which were 1.35, 1.31, 1.28, and 1.25, respectively. Third, an exploratory factor analysis was conducted with MPlus 7 (Muthén & Muthén, 2012). The model was estimated with a robust mean- and variance-adjusted weighted least squares (WLSMV) procedure and GEOMIN oblique factor rotation. Items with a primary factor loading >.40 were retained for the CFA. Fourth, the CFA was used on the same sample to test and compare the same four models as in the PHQ-15. None of the proposed models reached a satisfactory model fit, possibly due to a large number of single items and resulting cross-loadings. Consequently, we used an alternative approach which could account for the substantial cross-loadings present in the solution, namely an exploratory structural equation modeling (ESEM) (Asparouhov & Muthén, 2009; T. A. Brown, 2015; Marsh et al., 2010; Marsh, Morin, Parker, & Kaur, 2014). The ESEM approach combines the EFA and CFA measurement models within the same solution. Important for the current analyses, in the ESEM solutions, items of one factor are allowed to cross-load on other factors. Within this approach, we tested a bifactor ESEM model (Model 5) with one general and four specific factors using an orthogonal bifactor target rotation, in which the main loadings are freely estimated, whereas all cross-loadings are modeled to be close to zero (Figure 1). Using a typical bifactor assumption, the orthogonality of factors (Reise, 2012), allowed for a comparison with a bifactor CFA model (Model 4) (Morin, Arens, & Marsh, 2016). Nevertheless, given the exploratory nature of the ESEM, the group factors established with this analysis should be viewed as preliminary until replicated using CFA.
The models were estimated with the WLSMV procedure, which is based on the matrix of tetrachoric correlations. As such correlations can be biased by low cell frequencies (M. B. Brown & Benedetti, 1977), rarely used response categories were collapsed to reach the frequencies of minimum 5% in each cell. The PHQ-15 dataset contained a small amount of missing data, with 951 participants (90%) responding to all 15 items, 77 (7%) responding to 14 items, and 22 (2%) responding to 13 items. One participant did not complete the PHQ-15. The CSD dataset did not contain missing data. A minimal amount of missing data in the PHQ-15 dataset was handled with pairwise deletion. Due to the sensitivity of χ 2 test to the complexity of the model and the sample size, the model fit was evaluated with other descriptive fit measures, such as the root mean square error of approximation (RMSEA) and the comparative fit index (CFI). Following the recommendations of Hu and Bentler (1999), RMSEA values below .05 and CFI values higher than or close to .95 are treated as the indices of a good model fit. However, as CFI cutoff of .95 is sometimes perceived as too restrictive, the models with CFI values larger than .90 may be accepted, especially in research concerning psychological traits (Beauducel & Wittmann, 2005). For model comparison, we applied the DIFFTEST procedure available for the WLSMV estimation in MPlus. This functionality accounts for the fact that the distribution of the WLSMV based χ 2 differences is not distributed as χ 2.
Internal consistency of the general and specific factors was evaluated by computing coefficient omega and coefficient omega hierarchical (Brunner, Nagy, & Wilhelm, 2012; Rodriguez, Reise, & Haviland, 2016a, 2016b). Coefficient omega (ω) reflects the proportion of variance in the factor score that can be attributed to all sources of variance, whereas coefficient omega hierarchical (ωh) refers to the proportion of systematic variance in unit-weighted total scores attributable to a general factor (Reise, Scheines, Widaman, & Haviland, 2013; Rodriguez et al., 2016b). The strength of the general factor was investigated with explained common variance (ECV), which reflects the proportion of all common variance explained by the general factor. The indices were computed using the Bifactor Indices Calculator (Dueber, 2017). All coefficients are reported in the standardized form.
Results
Table 1 presents descriptive statistics and correlations between study variables. Although the sample consisted of undergraduate students, the average score of the PHQ-15 was similar to the one observed in the primary care setting (Körber, Frieser, Steinbrecher, & Hiller, 2011).
Descriptive statistics and Pearson correlations between study variables.
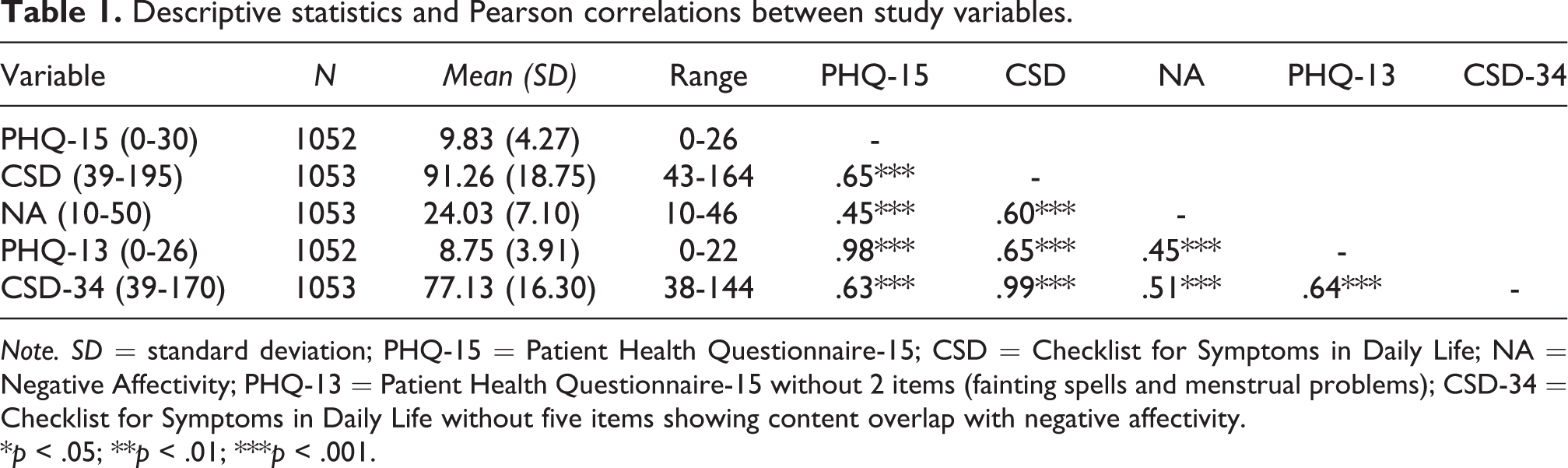
Note. SD = standard deviation; PHQ-15 = Patient Health Questionnaire-15; CSD = Checklist for Symptoms in Daily Life; NA = Negative Affectivity; PHQ-13 = Patient Health Questionnaire-15 without 2 items (fainting spells and menstrual problems); CSD-34 = Checklist for Symptoms in Daily Life without five items showing content overlap with negative affectivity.
*p < .05; **p < .01; ***p < .001.
The Latent Structure of Somatic Symptoms in the PHQ-15
The latent structure of somatic symptoms in the PHQ-15 was tested with four CFA models. A one-factor factor model included 13 symptoms and resulted in the poor fit (Table 2). A correlated group-factor model was specified with four correlated latent factors (pain-, gastrointestinal-, cardiopulmonary-, and fatigue-related symptoms), which showed medium to large correlations with rs ranging from .46 to .67, all ps < .001. The model fit indices were good and comparable to the fit obtained for the hierarchical model with four lower-order and one higher-order factor. Finally, the bifactor model including four orthogonal symptoms-specific factors and one general factor showed not only an excellent fit (CFI = .991; RMSEA = .019; 90% CI [.007, .029]), but also fitted the data significantly better than the hierarchical model, χ 2(5) = 52.07, p < .001, as revealed by the χ 2 difference tests. Standardized parameter estimates of the bifactor model, omega coefficients, and ECV are displayed in Table 3. Both ECV and omega hierarchical indicate the presence of multidimensionality.
Goodness-of-fit statistics for the measurement models of the Patient Heath Questionnaire-15 (PHQ-15) and the Checklist for Symptoms in Daily Life (CSD).
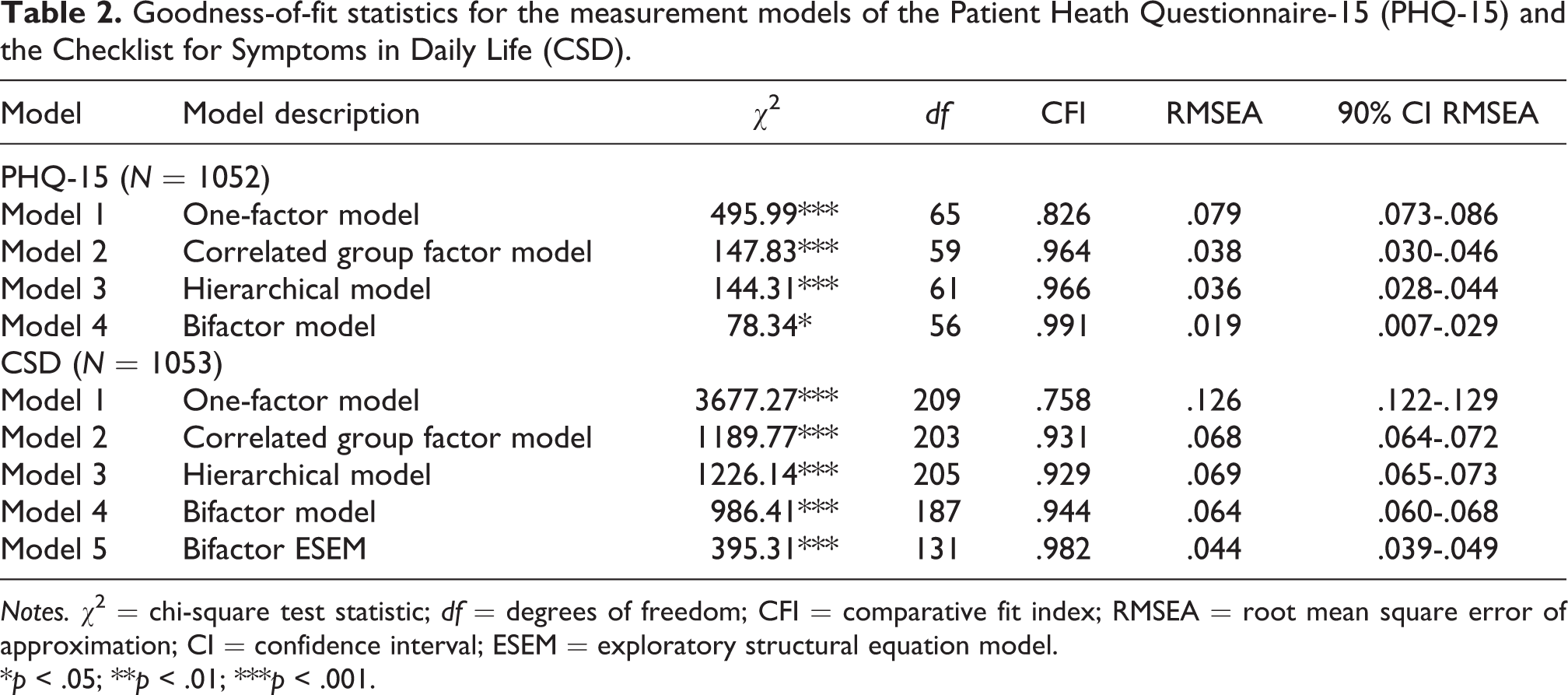
Notes. χ 2 = chi-square test statistic; df = degrees of freedom; CFI = comparative fit index; RMSEA = root mean square error of approximation; CI = confidence interval; ESEM = exploratory structural equation model.
*p < .05; **p < .01; ***p < .001.
Standardized factor loadings of the bifactor model (Model 4) of the Patient Health Questionnaire-15 (PHQ-15) with explained common variance (ECV) and model-based reliability estimates.

Notes. Factor loading coefficients printed in bold are significant at p < .05. ω/ωs are the omega coefficients for the general and specific factors, respectively. ωh/ωhs are the omega hierarchical coefficients for the general and specific factors, respectively. G-SOM = general factor.
The Latent Structure of Somatic Symptoms in the CSD
First, a one-factor model was tested. This model consisted of 22 symptoms loading on one latent factor (G-SOM). The model yielded poor fit indices (Table 2). Second, a correlated group-factor model was examined. The model was specified with four correlated latent factors previously determined by the EFA (see Table S2 in Supplementary Materials for factor structure), that is, a respiratory factor (F1), a cold/flu factor (F2), a neurological factor (F3), and a cardiovascular factor (F4). The correlations between all factors were significant and medium to large, with rs ranging from .50 to .76, all ps < .001. The model fit indices were suboptimal. A similar fit was obtained by the hierarchical model, specified by four symptom-specific lower-order factors and one general higher-order factor. Although the bifactor model, which allowed every item to load on a general factor as well as on one of the four orthogonal symptom-specific factors, showed a better fit than the other models, the values of the fit indices did not reach the cut-off values. The only model that adequately fitted the data was the bifactor ESEM model (Model 5), which allowed for cross-loadings (CFI = .982; RMSEA = .044; 90% CI [.039, .049]). This model resulted in a significantly better fit than the bifactor model (Model 4), χ 2(56) = 482.56, p < .001. Standardized parameter estimates of this model, omega coefficients, and ECV are displayed in Table 4. The general factor was well defined with the majority of target loadings > .40. With the exception of eight items, all items loaded above .40 on their specific factors. The inspection of both ECV and omega hierarchical suggested the presence of multidimensionality.
Standardized factor loadings of the bifactor ESEM model (Model 5) of the Checklist for Symptoms in Daily Life (CSD) with explained common variance (ECV) and model-based reliability estimates.

Notes. Target loadings are highlighted in bold. ESEM = exploratory structural equation model; G-SOM = general factor; F1 – respiratory symptoms; F2 – cold/flu symptoms; F3 = neurological symptoms; F4 = cardiovascular symptoms. ω/ωs are the omega coefficients for the general and specific factors, respectively. ωh/ωhs are the omega hierarchical coefficients for the general and specific factors, respectively.
*p < .05; **p < .01; ***p < .001.
Association between the Bifactor Models (PHQ-15 and CSD) and NA
The strength of the association between NA and different factors in the bifactor model was tested separately for the PHQ-15 and the CSD. In the PHQ-15 bifactor model, NA was associated with the PHQ-15 general symptom factor, r = .53, p < .001 (Figure 2). A significant but small correlation with fatigue symptoms was observed, r = .14, p = .045. No significant correlations were observed between NA and the other symptom-specific factors (all rs < .09, ps > .05). The model fit was good, χ2(64) = 85.38, p = .038; CFI = .993; RMSEA = .018; 90% CI [.004, .027].

Bifactor model of somatic symptoms in the PHQ-15 with negative affectivity (NA). Single headed arrows represent factor loadings; double-headed arrows represent latent correlation coefficients; error terms of manifest variables not shown. G-SOM = general factor; Gastrointest = gastrointestinal; Cardio-pulmon = cardiopulmonary. *p < .05; **p < .01; ***p < .001.
In the CSD bifactor ESEM model, NA was strongly associated with the CSD general symptom factor, r = .51, p < .001 (Figure 3). Significant but smaller correlations between NA and the other CSD symptom-specific factors were observed for flu symptoms, r = .25, p < .001, cardiovascular symptoms, r = .11, p = .001, and neurological symptoms, r = -.08, p = .02 . The model fit was good: χ2(148) = 440.02, p < .001; CFI = .980; RMSEA = .043; 90% CI [.039, .048].

Bifactor ESEM model of somatic symptoms in the CSD with with negative affectivity (NA). Full unidirectional arrows represent the main factor loadings; dotted unidirectional arrows represent cross-loadings; double-headed arrows represent latent correlation coefficients; error terms of manifest variables not shown. G-SOM = general factor; Resp = respiratory; Neurolog = neurological; Cardio = cardiovascular. *p < .05; **p < .01; ***p < .001.
Discussion
This psychometric study aimed to empirically test the view that symptom perception involves a sensory-perceptual and affective-motivational component. The specific aims were twofold: First, to replicate the previously reported finding regarding the latent structure of somatic symptoms in a different population and with two symptom questionnaires, differing in scope and content. Second, to further investigate the construct validity of the observed factors by examining their associations with trait NA. Compared to the alternative models, the bifactor model with one general symptom factor and several symptom-specific factors revealed the best fit for symptom reporting measured by the two self-report instruments. Whereas previous studies investigating this issue analyzed symptom distress as assessed by the PHQ-15 (Kroenke et al., 2002), we added a questionnaire (the CSD) consisting of a largely different sample of symptoms including a broad range of cardiovascular, respiratory, neurological, and common cold symptoms. This questionnaire covers more respiratory-related items than the PHQ-15, and it uses a different time frame (the last year vs. the last 4 weeks). Moreover, it collects frequency ratings of symptoms in the daily life, whereas the PHQ-15 assesses the distress related to the symptoms. In the current study, a large proportion of symptoms included in both bifactor models showed loadings greater than .40 on both the general factor and one of the symptom-specific factors, indicating that nearly each symptom was simultaneously determined by two sources of systematic variance. With the bifactor model outperforming alternative structural models in the analyses based on both the PHQ and the CSD, our results are consistent with earlier findings and add to the growing psychometric evidence in favor of the bifactor model approach adopted in structural modeling of symptom reporting (Jasper et al., 2015; Porsius et al., 2015; Thomas & Locke, 2010; Witthöft et al., 2016; Witthöft, Hiller, et al., 2013).
The findings of this study also provide additional support to the interpretation of the latent factors of this model. Strong associations have been previously observed between the general factor (but not symptom-specific factors) on the one hand and psychological traits such as health anxiety, somatosensory amplification, depressive symptoms (Witthöft et al., 2016), and somatoform dissociation on the other hand (Jasper et al., 2015). Moreover, the general factor was also related to emotion regulation strategies, including a negative association with cognitive reappraisal and a positive correlation with symptom focused rumination (Witthöft, Loch, & Jasper, 2013). These findings suggest that the general symptom factor is closely related to the affective processes and represents the affective-motivational component of symptom perception. The observed strong association of trait NA with the general factor, and the much smaller association with symptom-specific factors corroborates that conclusion. Because NA is a general vulnerability factor to report symptoms unrelated to physiological dysfunction (Bogaerts et al., 2015), understanding the mechanisms underlying the close association between this personality trait and elevated symptom reporting is crucial. Two perspectives on this link were advanced. One of these perspectives, a more biological one, focuses on the role of sympathetic and parasympathetic activity (Jarrett et al., 2003; but see also Houtveen & van Doornen, 2007). The other perspective suggests that NA is associated with chronically active somatic memory schemata leading to a biased symptom processing through modulation of the way incoming bodily signals are perceived and interpreted (Bogaerts et al., 2010; R. J. Brown, 2004; Constantinou et al., 2013; Van den Bergh, Stegen, & Van De Woestijne, 1998). A significant and high correlation between trait NA and the general symptom factor but not with the symptom-specific factors seems to favor the latter perspective. Indeed, this fits with recent studies showing that simply inducing a negative affect state through picture viewing followed by a symptom questionnaire induces elevated symptom reports in high NA persons, independent of physiological arousal (Constantinou et al., 2013). Interestingly, this effect is particularly strong in high trait NA persons who have difficulties to identify feelings and tend to become absorbed in experiences (Bogaerts et al., 2015; Van Den Houte et al., 2017). Within a predictive coding framework, this pattern of results suggests that symptom questionnaires prime symptom-related priors prompting the experience of symptoms in persons who are little able to perceive sensory-perceptual details of a somatic experience and to distinguish somatic and affective states (Van den Bergh et al., 2017).
The distinction supported by our results between sensory-perceptual, physical aspects of somatic experiences and affective-motivational processes involved in the evaluation of bodily sensations is compatible with recent changes included in the DSM-5 (American Psychiatric Association, 2013) regarding the criteria for somatic symptom disorder. The new classification emphasizes the distress caused by persistent somatic symptoms, and includes excessive feelings, thoughts, and behaviors in response to those symptoms. It is important to realize that this recent conceptualization does not require, as the DSM-IV somatoform disorder, a lack of organic explanation for the presented symptoms. Instead, it focuses on the preponderant affective-motivational responses to those symptoms. In this respect, the bifactor model psychometrically endorses this approach by showing that symptom perception is influenced by both a general symptom factor representing the affective-motivational aspects of symptom perception, but also by several symptom-specific factors. The latter may reflect sensory-perceptual component and are likely disorder-specific. For example, the irritable bowel syndome (IBS) diagnosis will show stronger association with the gastrointestinal than with respiratory symptoms (Witthöft, Hiller, et al., 2013).
The growing evidence for the bifactor structure of symptom reporting could have important implications for future research in terms of scoring questionnaires and measuring changes in symptoms related to illness or intervention. For example, Porsius et al. (2015) recently applied a bifactor model approach to investigate the effect of an environmental change (introduction of a new high-voltage power line) on the development of somatic complaints. The change in the total symptom score observed in this study was driven predominantly by the changes in symptom-specific factors. The authors also proposed that a temporary illness episode or treatment has greater chances of influencing symptom specific factors (Porsius et al., 2015). Conversely, the results of the present study may suggest that interventions that are directed towards NA or negative feelings in response to somatic complaints (e.g., interoceptive exposure, reattribution of somatic sensations, decreasing intolerance of uncertainty regarding somatic sensations; Van den Bergh et al., 2017) could reduce symptom reporting through changes in the general factor, but less so in symptoms specific factors. The sensory component of symptom distress might be effectively targeted and reduced by techniques that increase the perception of benign somatic sensations (Schaefer, Egloff, Gerlach, & Witthöft, 2014) and help to distinguish between different kinds of somatic sensations (i.e., “interoceptive differentiation training”, Van den Bergh et al., 2017, p. 199).
A limitation of the current work is the sample, which consisted of young, healthy, and predominantly female students. Although a bifactor model was previously supported in studies involving primary care patients (Witthöft, Hiller, et al., 2013) and patients with epilepsy (Thomas & Locke, 2010), further studies are needed to replicate and extend the construct validity of the latent factors in the bifactor model found in the homogenous samples of university students (Jasper et al., 2015; Witthöft et al., 2016) to clinical samples. For IBS, both the general and the disorder-specific (gastrointestinal symptoms) factors of the bifactor model were found to predict the diagnosis of IBS in primary care (Witthöft, Hiller, et al., 2013). Other clinical samples among which the bifactor model could be investigated are patients with fibromyalgia and chronic fatigue syndrome. Those two disorders display similar symptoms, which poses difficulties for clinicians and researchers to differentiate them. Investigating the associations between these disorders and the general as well as disorder-specific factors (i.e., pain and fatigue) of symptom distress could be informative to disentangle which symptom factors contribute to the diagnosis of these disorders. Concerning the bifactor model of the PHQ-15, it has to be acknowledged that the item-factor ratio is suboptimal and that the model cannot be considered very parsimonious. Particularly the fact that the fatigue symptom factor is determined by only two indicator variables is problematic (although no problems with model identification were observable). Future studies should therefore aim at replicating the proposed bifactor model by using extended versions of the PHQ-15.
Another limitation of this study pertains to a gender balance of our sample. Gender is a well-established factor associated with differences in symptom reporting, with women reporting more frequent, numerous, and intense symptoms than man (Barsky, Peekna, & Borus, 2001; Gijsbers van Wijk, Huisman, & Kolk, 1999). In addition, gender differences were found in the pattern of associations between the NA and different types of symptoms (Van Diest et al., 2005). Unfortunately, the unequal distribution of gender with a small sample size for men (n = 184) compared to women (n = 869) precluded the multiple-group analyses of these data. Future studies should explore whether the correlations between NA and latent factors could be influenced by gender differences.
In summary, the current study replicates and extends findings that psychometrically support a distinction between sensory-perceptual and affective-motivational components of self-reported symptoms. The substantial correlation between trait NA and the general symptom factor provides further evidence that the latter mainly represents the affective-motivational component or distress associated with somatic symptoms.
Supplemental material
Supplemental Material, JEP059716_supplement - Sensory and affective components of symptom perception: A psychometric approach
Supplemental Material, JEP059716_supplement for Sensory and affective components of symptom perception: A psychometric approach by Marta Walentynowicz, Michael Witthöft, Filip Raes, Ilse Van Diest, and Omer Van den Bergh in Journal of Experimental Psychopathology
Footnotes
Acknowledgments
We wish to thank David Dueber for statistical consultation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Grant OT/10/027 from the University Research Council of University of Leuven.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.