
Abstract
Metacognitive beliefs implicated in the Self-Regulatory Executive Function (S-REF) model (Wells & Matthews, 1994, 1996) have demonstrated significant positive relationships with experiences of psychosis. This study aimed to investigate the effect of manipulating metacognitive beliefs relating to the uncontrollability and danger of thoughts on paranoia frequency and negative affect in a non-clinical sample. Seventy-six students participated in a randomised experiment. All participants were falsely informed they were taking part in an EEG study about thought processes in paranoia. Following a paranoia induction, participants in the experimental condition were told that the EEG could detect paranoid thoughts and may make a loud noise in response to detecting them; participants in the control condition were told the EEG could detect paranoid thoughts and may make a loud noise at random. Validity checks confirmed the paranoia prime was effective and there was a significant change in metacognitive beliefs following the manipulation. Overall no significant differences between the two groups on measures of intrusions or anxiety emerged following the manipulation. However, changes in physiological anxiety approached significance. The results demonstrate it is feasible to manipulate metacognitive beliefs and induce paranoia. A recommendation for further research to use a refined paradigm with a clinical sample is discussed.
Introduction
Metacognitive beliefs refer to beliefs about thought processes. They affect the way particular cognitive processes are appraised and utilised (Wells, 2000, pp. 6-7). A specific set of metacognitive beliefs have been linked to unhelpful thinking patterns associated with emotional dysregulation. These beliefs form the basis of the Self-Regulatory Executive Function (S-REF) model (Wells & Matthews, 1994, 1996); an information processing approach to psychological disorder. Within this model, the prolongation of psychological distress is related to the use of maladaptive coping strategies (such as worry, rumination, threat monitoring and thought control) that are underpinned by a combination of positive and negative metacognitive beliefs (Wells, 2000, p. 25). Positive metacognitive beliefs reflect the usefulness of worry, rumination, threat monitoring, and thought control (e.g. “focussing on danger will keep me safe” or “if I worry I will be prepared”), and are thought to initiate and support their continued use. Negative metacognitive beliefs reflect beliefs concerning the danger or uncontrollability of particular thoughts (e.g. “my thoughts are uncontrollable” or “my thoughts could make a bad thing happen”), and are thought to increase distress and prolong unhelpful thinking patterns.
Research has supported a relationship between unhelpful metacognitive beliefs and paranoia in both non-clinical and clinical samples. In particular, negative metacognitive beliefs relating to the uncontrollability and danger of thoughts appear to be particularly influential (e.g. Valiente, Prados, Gomez, & Fuentenebro, 2012). However, this association is reduced when negative affect (i.e. anxiety), and alternate psychotic phenomena (i.e. auditory hallucinations) are controlled (Garcia-Montes, Cangas, Perez-Alvarez, Hidalgo, & Gutierrez, 2005; Goldstone, Farhall, Thomas, & Ong, 2013). The emerging view is that metacognitive beliefs do not have a causal role in specific symptoms, but may rather be associated with higher levels of distress (Varese & Bentall, 2011). Consistent with this, a recent meta-analysis found that people with a diagnosis of psychosis are significantly elevated in all sub-types of metacognitive beliefs compared to non-psychiatric controls, and have similar patterns to people with a diagnosis of emotional disorder (Sellers, Varese, Wells, & Morrison, 2016). Moreover, at risk mental state (Morrison et al., 2006), and transition to first-episode psychosis is associated with elevated levels of negative metacognitive beliefs (Barbato et al., 2013; Morrison et al., 2002); whilst clinical samples with more negative beliefs appear to experience greater distress (e.g. van Oosterhout, Krabbendam, Smeets, & van der Gaag, 2013). This pattern of results supports the prediction that metacognitive beliefs may be associated with emotional dysregulation and negative affect, which may affect symptoms.
Negative affect appears to have an influential role in positive symptoms of psychosis, such as hallucinations and delusional beliefs. Studies have noted an increase in anxiety and depression during the psychosis prodrome (Yung & McGorry, 1996) and an association between negative emotional states and the severity and content of symptoms (Freeman & Garety, 2003; Hartley, Barrowclough, & Haddock, 2013). It has recently been suggested that treating emotional dysregulation in people with experiences of psychosis may lead to reductions in symptoms (Freeman et al., 2013). Therefore, if metacognitive beliefs are a determinant of negative affect, they may be an important target for therapeutic intervention in people with psychosis.
Consistent with this, a recent study found that negative metacognitive beliefs, in particular those relating to the uncontrollability and danger of thoughts, are a stronger predictor of negative affect than positive symptoms themselves (Sellers, Gawęda, Wells, & Morrison, 2016). A similar pattern has emerged concerning metacognitive beliefs specific to paranoia, such as those measured using the beliefs about paranoia scale (Gumley, Gillan, Morrison, & Schwannauer, 2011; Morrison et al., 2005). Studies have indicated that positive beliefs about paranoia as a survival strategy are associated with the frequency of paranoid ideation in both non-clinical and clinical samples (Morrison et al., 2005; Murphy et al., 2017), whilst negative beliefs about paranoia appear to predict higher levels of anxiety and depression, as well as clinical status (Gumley et al., 2011; Morrison et al., 2011).
This study aims to manipulate metacognitive beliefs in a non-clinical sample. Previous experimental studies have manipulated response styles associated with metacognitive beliefs, but have not directly manipulated metacognitive beliefs. These studies have demonstrated that coping strategies associated with suppression, distraction and rumination may increase intrusive experiences due to rebound effects (Garcia-Montes, Perez-Alvarez, & Fidalgo, 2004; Hartley, Bucci, & Morrison, 2017; Martinelli, Cavanagh, & Dudley, 2013). This study will test the effect of an experimental manipulation of metacognitive beliefs on paranoid intrusions and state anxiety in students. Paranoia has been selected as the dependent variable because there is a strong argument that paranoid ideation lies on a continuum of severity that can be measured in the general population (Freeman et al., 2005; Johns et al., 2004), and may precede more severe persecutory belief formation (Kaymaz et al., 2012; Poulton et al., 2000). Therefore, understanding the mechanisms involved in non-clinical paranoid intrusions and distress may have relevance to understanding clinical persecutory ideas.
The present study set out to manipulate metacognitive beliefs relating to uncontrollability and danger using a fake EEG paradigm. Paranoid ideation will be primed using three short video clips produced by Greater Manchester Police that relate to student safety, and uncontrollability and danger beliefs will be manipulated with the suggestion that subsequent detection of paranoid thoughts by the EEG may lead to a loud noise. The following hypotheses based on the S-REF model are tested: 1) Participants allocated to the belief manipulation condition will experience a higher number of intrusive threat-related thoughts as a result of unhelpful attempts to control them (i.e. rebound effects); 2) Participants allocated to the belief manipulation condition will experience greater discomfort in response to threatening thoughts assessed using a measure designed to capture participant experiences of intrusions and distress during the EGG; 3) Participants allocated to the belief manipulation condition will experience higher levels of state anxiety.
Method
Design
The experiment was conducted as a randomised group comparison. Participants were allocated to either the experimental condition (group 1;
Participants
Seventy-six students from the University of Manchester took part in the study. The sample consisted of 11 males and 65 females with a mean age of 19 years (
Sample demographic information.
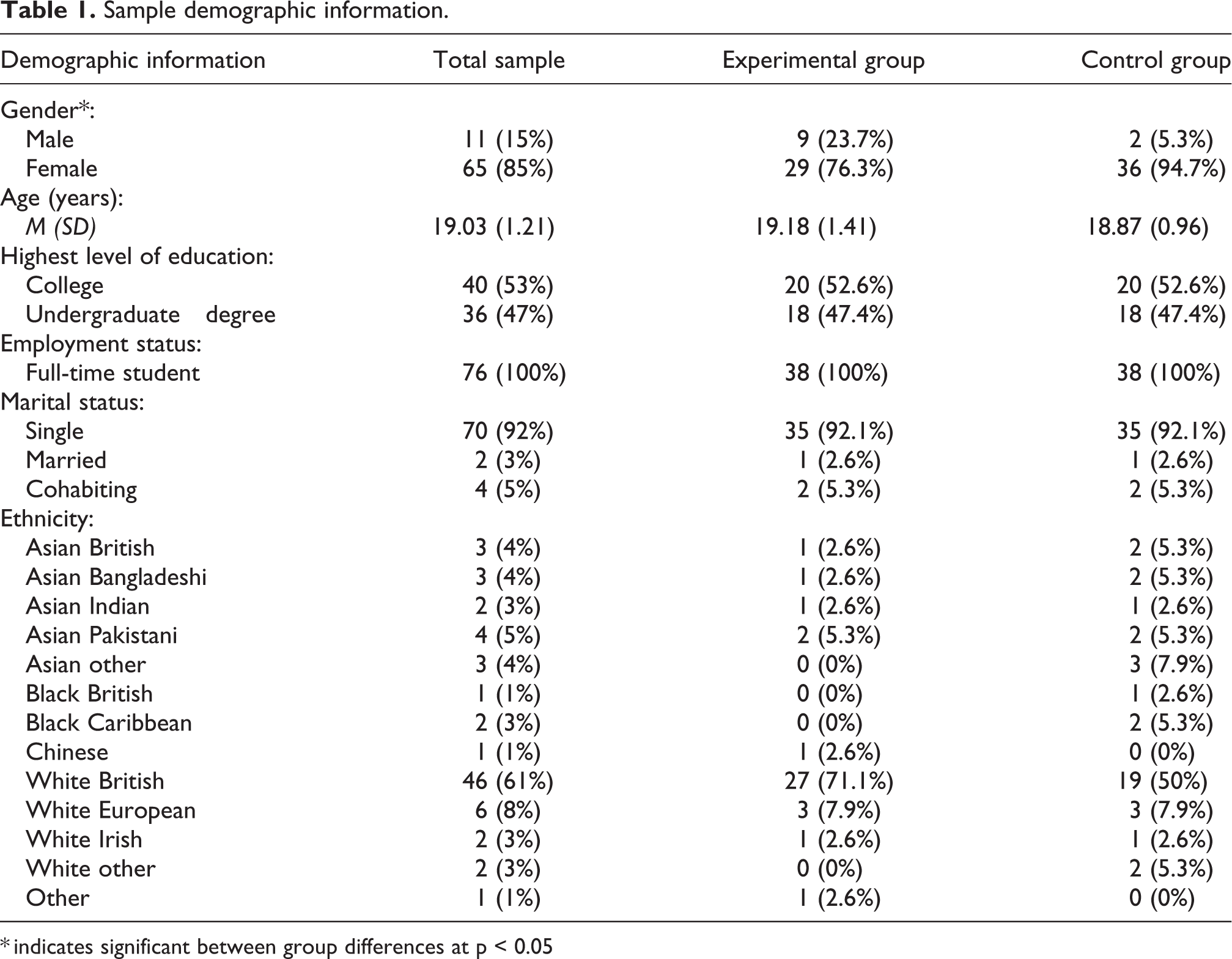
* indicates significant between group differences at p < 0.05
Participants were eligible to take part if they reported paranoid ideation in the past week. This was operationalised as a rating of “sometimes” in response to at least one item on the Paranoia Checklist (Freeman et al., 2005). Participants were not eligible for the study if they have a history of severe mental health problems (e.g., schizophrenia, bipolar disorder, affective psychosis); currently use secondary mental health services (e.g., community mental health teams or early intervention services); currently take psychiatric medication; or have a sight or hearing impairment that would prevent engagement with video stimuli.
Measures
Video stimuli
Paranoia was manipulated using three video clips produced by Greater Manchester Police; each clip was 60 seconds long. Participants watched the videos after completing baseline questionnaire measures. The first video was about staying safe online and discussed themes relating to social media posts, fake profiles and online bullying. The second video clip was about personal safety and discussed themes relating to situational awareness, spotting suspicious behaviour and personal attack alarms. The third video clip was about student burglaries and depicted scenes of open windows, unlocked doors and valuables on display. These video clips were selected to be relevant to the student sample.
Procedure
Ethical approval was granted from the University of Manchester Research Ethics Committee 1 (UREC-1; reference: 15455). The fake EEG procedure utilised in this study was adapted from Myers and Wells (2013). Prior to taking part, participants were provided with a copy of the participant information sheet and asked to complete the screening questions. Those that were eligible were invited to meet with the researcher and complete the experiment.
The experiment was conducted in a temperature controlled room. After receiving a verbal overview of the study participants completed a consent form, a demographics form and self-report questionnaires (the STAI and a manipulation check). They were then connected to the GSR and a four minute baseline was commenced.
After the four minute baseline, participants received the following instruction: “We are interested in thought processes and how these affect our reaction to different stimuli. I’m going to connect you to an EEG that will pick up signals from a part of your brain that is related to threat. It is very sensitive and studies have shown that it can often be triggered just by having thoughts relating to threatening themes and this activity is picked up by the EEG. In the first part of the experiment I’ll check this by showing you three short video clips from Greater Manchester Police”.
The researcher then assisted the participant in fitting the EEG cap and attached the electrodes. The electrodes were connected to a genuine EEG but participants were unaware that no actual EEG readings were being taken. As actual recordings were not taken, no gel was applied. When the EEG was set-up, participant’s watched three short video clips produced by Greater Manchester Police relating to student safety. The purpose of the video clips was to induce paranoid thoughts. After the three videos had finished, the researcher showed participants a 30 second EEG wave to increase the authenticity of the experience. Following this, the experimental group were told “Okay that is detecting the activity well. For the next four minutes I would like you to think about anything you want. If you have any threat related thoughts or thoughts about the video clips the EEG will detect this and I’m going to set it up so that each time it does you may hear a burst of white noise. The noise is high pitched and makes people jump. However, even though people find it unpleasant it is not harmful: having paranoid thoughts may lead you to hear this loud noise”. This instruction was intended to manipulate the metacognitive belief that some thoughts may cause negative outcomes and must be controlled.
The control group were given a variation of this instruction: “Okay that is detecting the activity well. For the next four minutes I would like you to think about anything you want. If you have threat related thoughts or thoughts about the video clips the EEG will detect this and I’m going to set it up so that unrelated to the thoughts you have, you may randomly hear a burst of white noise. The noise is high pitched and makes people jump. However, even though people find it unpleasant it is not harmful: unrelated to the thoughts you have, you may randomly hear this loud noise”.
After four minutes, the GSR was terminated and the EEG cap and electrodes were removed. None of the participants, in the experimental or control group, were subject to a burst of white noise. Participants then completed the second battery of self-report questionnaires (a measure of their experiences, the STAI, the manipulation check and an experimental validity check).
Data analysis plan
Power calculation
A power calculation utilising http://www.sealedenvelope.com was conducted to advise sampling. Seventy-six participants were required to have a 90% chance of detecting, as significant at the 5% level, an increase in the primary outcome measure from 15 in the control group to 30 in the experimental group. This calculation was advised using data from (Myers & Wells, 2013).
Statistical analysis
Data were screened for missing values, outliers and normality prior to analysis. The two groups (experimental and control) were then screened to test that the randomisation procedure resulted in equality between the two groups on demographic variables (i.e. age and gender), baseline anxiety (i.e. STAI scores and GSR readings), baseline paranoia and baseline metacognitive beliefs (i.e. the manipulation check).
Following this, a number of validity and manipulation checks were conducted. The validity of the fake EEG paradigm was tested using between subjects analysis of variance (ANOVA). The dependent variables were ratings of the three beliefs that constitute the experimental validity measure. The paranoia manipulation was tested using repeated measures ANOVA. The within subjects factor was time (pre- and post-video stimuli) and the dependent variable was the belief “I need to be on my guard against other’s”. The metacognitive belief manipulation was tested using a mixed factor ANOVA. The dependent variable was negative beliefs relating to uncontrollability and danger with a between subjects factor of group (experimental vs control) and a within subjects factor of time (pre- and post-manipulation).
The primary outcomes were tested using a series of one-way ANCOVA’s where the independent variable was group (experimental vs. control) and the dependent variables were items on the measures of experiences questionnaire. The secondary outcomes (i.e. STAI scores and GSR readings) were tested using one-way ANCOVA where the covariates were baseline anxiety. As above, the between subjects factor was group (experimental vs control) and the within subjects factor was time (pre- and post-manipulation).
Results
Data screening
There were no missing values in the data set. One univariate outlier was detected and amended using the next extreme score plus one. There were no multivariate outliers. One dependent variable (number of intrusions) demonstrated positive kurtosis and this was corrected using bootstrapping.
Baseline characteristics and descriptive statistics
Baseline characteristics and descriptive statistics for the two groups are presented in table 2. Independent samples t-tests revealed there were no significant differences between the experimental and control groups on age (
Sample characteristics on baseline measures for the experimental group and control group.
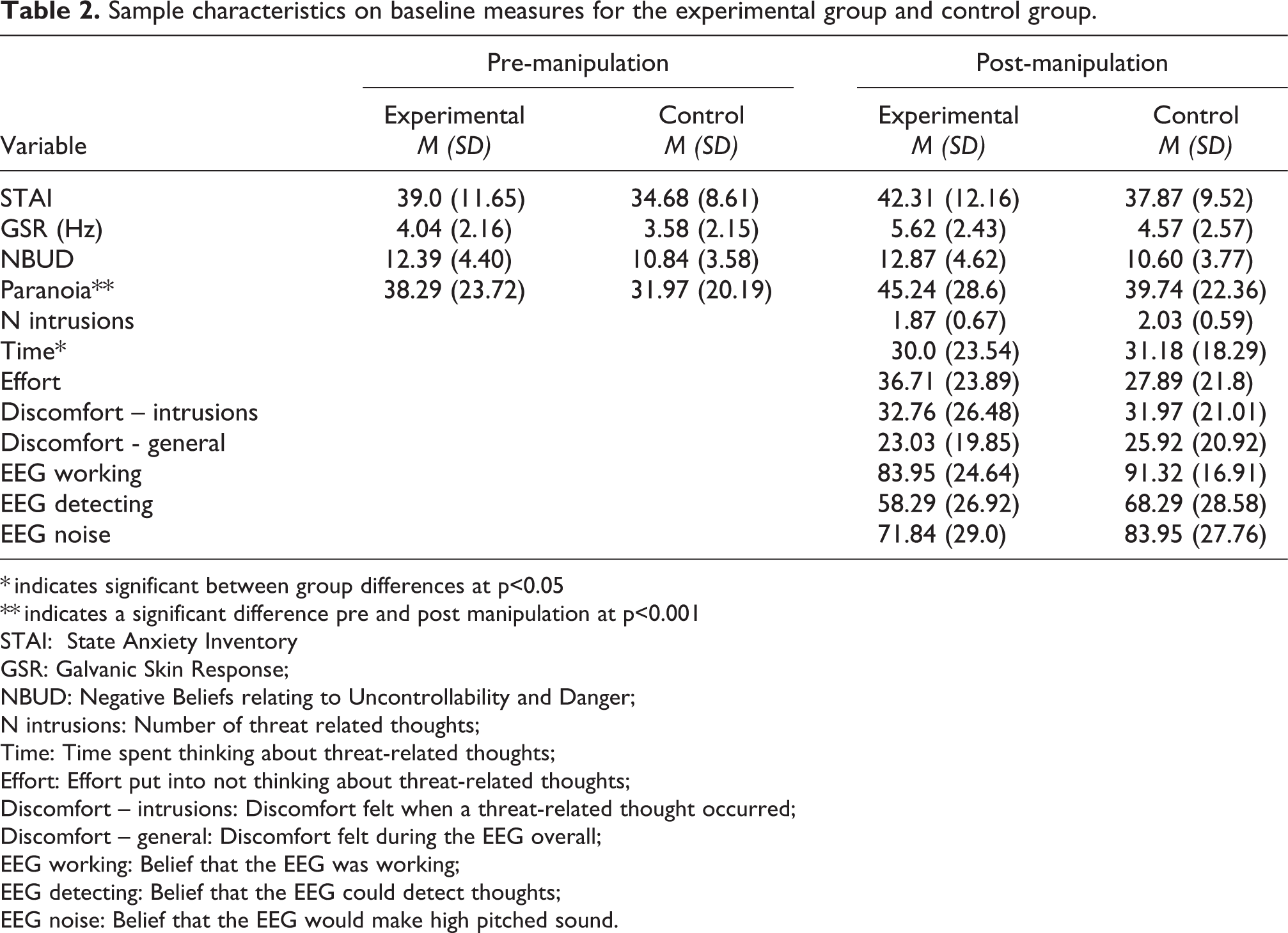
* indicates significant between group differences at p<0.05
** indicates a significant difference pre and post manipulation at p<0.001
STAI: State Anxiety Inventory
GSR: Galvanic Skin Response;
NBUD: Negative Beliefs relating to Uncontrollability and Danger;
N intrusions: Number of threat related thoughts;
Time: Time spent thinking about threat-related thoughts;
Effort: Effort put into not thinking about threat-related thoughts;
Discomfort – intrusions: Discomfort felt when a threat-related thought occurred;
Discomfort – general: Discomfort felt during the EEG overall;
EEG working: Belief that the EEG was working;
EEG detecting: Belief that the EEG could detect thoughts;
EEG noise: Belief that the EEG would make high pitched sound.
Experimental validity check
Analysis of co-variance revealed a marginally non-significant difference between the two groups in their belief that the EEG was working (
Manipulation check
A repeated measures ANOVA indicated a statistically significant change in ratings of paranoia (
A mixed factor ANCOVA revealed a significant time by group interaction for metacognitive beliefs (

Estimated marginal means for uncontrollability and danger beliefs in the experimental and control group before and after the metacognitive belief manipulation with gender as a covariate.
Primary outcome variables
A series of one-way ANCOVA’s indicated there were no significant differences between the experimental and control group on the items that constitute the measure of experiences during the EEG: number of threat-related thoughts (
Secondary outcome variables
Analysis of covariance revealed no significant differences in post-manipulation self-reported anxiety scores between the two groups when co-varying for gender, baseline anxiety scores and belief the EEG was working (
Discussion
This study aimed to manipulate negative metacognitive beliefs relating to the uncontrollability and danger of thoughts, using a fake EEG paradigm adapted from Myers and Wells (2013). The sample consisted of undergraduate students that had experienced paranoid thoughts in the past seven days. Paranoia was primed using three short video clips from Greater Manchester Police relating to student safety. Metacognitive beliefs were manipulated with the suggestion that the EEG could detect paranoid thoughts and may make a loud noise in response to detecting them.
First, the validity of the experimental paradigm was tested. The paranoia prime was effective as demonstrated by a significant increase in endorsement of the belief “I need to be on my guard against other’s” measured before and after the video stimuli. The manipulation of metacognitive beliefs was also effective as indicated by a significant interaction between group (experimental vs. control) and time point (pre- and post-manipulation). Following the manipulation instruction, uncontrollability and danger beliefs increased in the experimental group and decreased in the control group. This is an important finding, which indicates that metacognitive beliefs are amenable to experimental manipulation. Moreover, the mean belief the EEG was working was 88%, and belief it would emit a loud noise was 78%. However, belief that the EEG could detect thoughts was less (63%). Overall, these analyses are proof of concept that metacognitive beliefs can be experimentally manipulated in the context of paranoia.
The results of the primary analyses were not significant. Contrary to the hypotheses, there were no significant differences between the experimental and control group on self-reported intrusion frequency, effort put into controlling intrusions or general discomfort during the EEG. One possibility for this finding is the measure may have lacked sensitivity. The majority of participants gave the same answer for the item that captured the number of intrusive thoughts experienced during the EEG. It is therefore possible this question did not capture variability. The majority of participants responded they had experienced “a couple of thoughts (1-5)”. However, the subsequent items utilised 0-100 visual analogue scales which allowed for greater variability in response, and there were no significant differences between the two groups on these items.
In terms of the secondary outcomes, self-reported levels of anxiety at time two did not differ significantly between the experimental and control group when controlling for self-reported anxiety at time one. Between group differences in physiological ratings of anxiety using the GSR approached significance at time 2 when controlling for baseline GSR readings. Consistent with predictions, physiological anxiety was higher in the experimental condition. The reason that physiological anxiety approached significance but self-reported anxiety did not, may reflect the sensitivity of these measures to momentary fluctuations in negative affect. Whilst the self-report measure was specifically a state measure of cognitive and body state information, the GSR that measures skin conductance does not rely on the participant’s interpretations of body state information, which may be an important factor. The misinterpretation of cognitive and body state information is an important aspect of cognitive approaches to psychosis (e.g. Morrison, 2001). The GSR may also be better able to detect more subtle changes in arousal.
The S-REF model focuses on metacognitive beliefs and coping strategies that lead to biased information processing of threatening stimuli (Wells & Matthews, 1996). Negative metacognitive beliefs relating to the uncontrollability and danger of thoughts are considered especially important to intrusion frequency and negative emotional responses. The model suggests beliefs that thoughts need to be controlled or can cause negative outcomes lead to unsuccessful attempts to reduce intrusions and increase negative affect in response to them. Several studies have supported this finding in the psychosis and paranoia literature (Gumley et al., 2011; Murphy et al., 2017; Sellers, Gawęda, et al., 2016). The results of this study are partially consistent with this finding as they demonstrated changes in physiological arousal that approached significance in the experimental condition.
The main strength of this study is the proof of concept in the paradigm. However, if this experiment were to be repeated there are ways it could be refined and improved. First, an alternative measure of intrusion frequency may improve sensitivity. The majority of participants responded with the same answer which may indicate a lack of sensitivity to variation in frequency. Second, the null findings and the modest sample size raise the possibility of type-II error. Therefore, a future replication using a larger sample size may provide better statistical power to detect an effect. The power calculation for this study was based on a previous study by Myers and Wells (2013) that used a sample of people who met clinical threshold for obsessive compulsive disorder. An alternative possibility, therefore, might be to use a clinical sample. The threshold of paranoid ideation for inclusion in this study may have been a limitation (i.e. participants were required to endorse just one paranoid thought as occurring “sometimes” in the past week). Changes in metacognitive beliefs may have a more significant impact on people with more frequent or pervasive paranoid ideas.
There are also some general limitations to this study that should be considered when interpreting the results. First, the sample demographic limits the generalizability of the results. The sample was predominantly female and comprised of undergraduate university students. For this reason, the generalizability of this sample to both a wider non-clinical population and people with clinical paranoia is uncertain. Second, when using non-clinical populations it is important to bear in mind there are likely important differences in the nature of paranoid ideas. For example, paranoid ideas in the general population may reflect concerns that might have greater grounding in reality, and may be more likely to reflect social evaluative concerns and lower level ideas of reference (e.g. Freeman et al., 2005).
In terms of implications for theory and clinical practice, this study suggests that metacognitive beliefs relating to the uncontrollability and danger of thoughts are amenable to manipulation. This is consistent with the goals of metacognitive therapy that targets underlying metacognitive beliefs responsible for unhelpful coping strategies and emotional dysregulation. Metacognitive therapy has demonstrated effectiveness in reducing symptoms and psychological distress in emotional disorder (Normann, van Emmerick, & Morina, 2014), and has recently been piloted in psychosis with promising results regarding feasibility and acceptability (Morrison et al., 2014). The identification of unhelpful metacognitive beliefs that can enhance and maintain anxiety and maladaptive coping may help to tailor psychological interventions where emotional responses and avoidance are contributing to a person’s difficulties.
Overall, this paradigm is novel in its application to experiences of psychosis. The key finding is that metacognitive beliefs can be experimentally manipulated, and there is clearly a gap in the psychosis literature for more research to do so. The findings suggest that experimentally heightened metacognitive beliefs may influence anxiety. If replicated, these findings could have important implications for psychological assessment and treatment of paranoia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.