
Abstract
There is growing appreciation among health and social care providers, especially those working in community-based programs with women or young people with substance use problems and/or who have experienced violence, maltreatment, or trauma, that a high number of their program participants may have been prenatally exposed to alcohol or have fetal alcohol spectrum disorder (FASD). This article provides a conceptualization of the key components of an FASD-informed approach. Drawing on the emerging literature and the author's research identifying the support needs and promising approaches in working with women, young adults, and adults with FASD, as well as evaluations of FASD-related programs, the article discusses what an FASD-informed approach is, why it is centrally important in working with women, adults, and young people who may have FASD, underlying principles of an FASD-informed approach, and examples of FASD-informed adaptations to practice, programming, and the physical environment. In this discussion, the benefits of using an FASD-informed approach for service providers and women living with FASD and their families, as well as conceptualization of FASD-informed policy and systems are highlighted.
Introduction
There is growing appreciation among health and social care providers, especially those working in community-based programs with women or young people with substance use problems and/or who have experienced violence, maltreatment, or trauma, that a high number of their program participants may have been prenatally exposed to alcohol or have fetal alcohol spectrum disorder (FASD). 1 Similarly, educators and child welfare researchers and practitioners are increasingly recognizing that a diagnosis of FASD in children or youth represents both an opportunity to identify and implement FASD-informed adaptations and shifts in practices to support the young person and as an opportunity to better understand and address the complex needs of the mother and family in recognition of the multiplicity of issues associated with FASD.2,3
Fetal Alcohol Spectrum Disorder
FASD is an umbrella term used to describe several diagnoses emerging from prenatal exposure to alcohol, including fetal alcohol syndrome (FAS), partial FAS, and alcohol-related neurodevelopmental disorder.
The effects of FASD can include physical anomalies, characteristic facial features, and central nervous system damage. While physiological effects may be present, there is growing consensus that FASD needs to be primarily understood as a brain-based disability, giving rise to a range of behavioral symptoms and cognitive and social difficulties. 4 Moreover, because FASD is primarily about brain difference, it is an invisible disability; the invisibility of FASD contributes to the numerous social and systemic challenges that people living with it face in daily life. 5
The effects of FASD vary considerably, and there is tremendous heterogeneity among people with FASD in terms of their strengths and difficulties. Factors affecting the range and severity of the effects include the amount, frequency, and timing of the alcohol consumed by the pregnant woman; her overall health, wellness, and nutritional status during and prior to her pregnancy; her genetic make up; other possible teratogens affecting the fetus; and a host of environmental factors.1,4 Nevertheless, the majority of people who have FASD live with significant cognitive, behavioral, health, and learning difficulties, including problems with memory, attention, cause and effect reasoning, impulsivity, and receptive language and adaptive functioning difficulties. ∗ 4,6,7 And while there are strategies and approaches that can be put into place to mitigate the effects of FASD, as an irreversible neurodevelopmental disability, the implications of FASD are lifelong.
Prevalence
FASD is the leading known cause of congenital brain damage and developmental disability in North America.8,9 Until several years ago, the estimated prevalence in North America was one in 1000 live births for FAS and one in 100 live births for FASD. More recently, however, research indicates that the prevalence is markedly higher than what had been thought, with the rate of FASD now being reported as 2%–5% of the population in US and some Western European countries. 10
Why FASD-Informed Practice
The majority of those living with FASD, particularly adults, will not have been diagnosed; assessment of FASD is rare among the general population, and adult assessment/diagnosis of FASD is almost nonexistent. ∗∗ Moreover, there are a number of reasons why many adults with FASD will not disclose that they may have FASD, including the stigmatizing nature of FASD, the person's memory difficulties, and/or lack of appreciation of the relevance of FASD in relation to services.
This is due to a variety of factors, including the lack of diagnostic clinics and trained professionals able to make an adult diagnosis, the lack of reliable resources – beyond self-reporting – to gather the adult's personal and family history, and the lack of access to financial resources to cover the significant costs of the assessment. 5
Nevertheless, FASD researchers, program developers, and staff have noted that “whether they know it or not, community service providers are often working with people who have FASD.” 11 This observation is grounded in a hallmark study that explored the life circumstances of 80 birth mothers whose children had been assessed as having FASD. The research found that 50% of the women had FASD themselves, moreover, 95% of the women had experienced physical, emotional, or sexual abuse, 80% of the women had a major unaddressed mental illness, over 75% of the women had post-traumatic stress disorder, and the majority of the women lived in deep poverty. 12 Similarly, program managers in Canada have observed parallels in the lived experiences of many participants in their services for high-risk pregnant/parenting women and the secondary effects of FASD (to use terminology coined by Streissguth et al. 13 ) experienced by adults with FASD. These experiences/effects include low education, unemployment, housing instability and/or dependent living, mental health problems, alcohol or drug issues, childhood or current experience of abuse, maltreatment, violence or trauma, and involvement with the criminal legal system.1,14
Yet, despite the reality that some – if not many – program participants may have FASD, nearly all health, social, justice-related, employment, and education programs have been designed in ways that present challenges for people with FASD.4,15 Indeed, research and practice evidence demonstrates that people with FASD do not generally experience success in typical programs, given that most programs are based on the behavioral learning models that assume that individuals have the memory, cognitive, and receptive language skills to understand, remember, and carry out what is being asked of them.1,4,6,16 Consequently, an individual's failure in programs is often attributed to the person herself rather than to the lack of fit between the person and the program. 4 In this vein, adolescents and adults with FASD are often erroneously perceived as being unmotivated, uncooperative, noncompliant, stupid, lazy, or bad.6,15–18
In addition, as has been noted by West and Antrobus, Dubovsky, and others, of serious concern is that individuals' experience of stress in attempting to meet program demands and not succeeding can result in chronic distress, an internalized sense of personal failure and loss of self-esteem. Compounding this are the real and potentially dire risks to health and well-being for adults with FASD due to the impacts of repeated failure in programs or failure as a parent or caregiver (eg, homelessness, unemployment, poverty, incarceration, child removal, substance-exposed pregnancies, lack of care due to being fired by health or social service providers, and even death).6,18
In view of these realities, it is imperative that programs are designed and delivered in ways that are FASD-informed that take into consideration the needs and challenges of those living with FASD. FASD-informed services promote health and wellness for individuals, families, and communities; FASD-informed services also make economic sense in that individuals participating in these programs will be more likely to succeed in and not require care/involvement from more expensive and intrusive systems (such as emergency services, corrections, and child welfare).
To this end, this article offers a conceptualization of the key components and underlying principles of an FASD-informed approach. This discussion is grounded in the author's previous research identifying the support needs and promising approaches in working with women, young adults, and adults living with FASD,5,19,20 and in the author's involvement in the evaluations of FASD prevention or FASD support programs or initiatives aimed at training community-based service providers to improve knowledge and practice in FASD-informed approaches. In view of the centrality of the one of these projects to operationally defining and developing markers of an FASD-informed approach, a brief description of the latter project and its methodology follows.
Toward an Evaluation Framework for Community-Based FASD Prevention Programs
The three-year Toward an Evaluation Framework for Community-based FASD Prevention Programs project aimed to bring program staff, evaluators, and funders together to create common evaluation frameworks and tools for FASD prevention programs serving pregnant women and mothers and for FASD support programs serving youth and adults living with FASD. Development of a common evaluation framework was seen as a way to promote ongoing learning within community-based agencies and to recognize the social, cultural, and geographic diversities that exist within FASD programs. Additionally, the project aimed to enhance community-based evaluation capacity by providing evaluation-related mentoring to several community agencies in Canada.
This project's methodology involved a number of integrated and iterative data collection activities. The research team began by contacting program providers, researchers, and evaluators across Canada and internationally in order to gather the evaluations of FASD prevention and FASD support programs, including programs focusing on addressing social determinants of health for pregnant and parenting women, and FASD-related programs within Aboriginal communities. The team then undertook a comprehensive review of these evaluations and related literature and teased out programs' theoretical underpinnings, activities, and approaches and participant/client and community outcomes. The team also received input via phone and e-mail discussions from the program providers and evaluators who had been contacted on respectful, effective approaches for working with women who may have FASD.
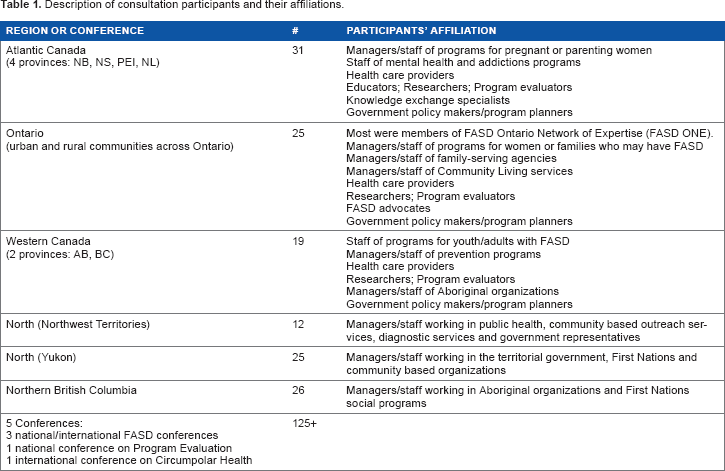
To visually display the information, the project team created three maps that depict FASD prevention programs, FASD support programs, and FASD programs in Aboriginal communities. Six regional consultations were then convened across Canada that enabled the researchers to receive feedback on the evaluation maps. A total of approximately 250 people from all regions in Canada and from a variety of professional disciplines and/or from different types of programming participated in the consultations related to this project. Table 1 provides additional description about the consultations and participants' affiliations.
Description of consultation participants and their affiliations.
During the second half of this project, the team further developed the maps. As a part of these activities, the team developed the operational definitions for the philosophical/ theoretical approaches used in the FASD prevention and support programs, including an FASD-informed lens and approach, along with outcomes, indicators, and relevant, publicly available measurement tools used in the evaluation of FASD-related programs. As the culmination of this project, the team launched a website (www.fasd-evaluation.ca) that provides the information and tools developed and/or compiled through the project.21,22
What is an Fasd-Informed Approach?
An FASD-informed approach starts with the understanding that FASD is a brain-based permanent disability that has wide ranging effects. 4 An FASD-informed approach uses knowledge about how FASD may affect a person in various and likely multiple facets of life, including physically behaviourally cognitively socially emotionally and spiritually. As importantly an FASD-informed approach recognizes that for people with FASD, past or current experiences of abuse, violence, victimization, or trauma may be present.18,23
An FASD-informed approach recognizes that as a result of the brain-based disability, children, youth, and adults may have difficulty following certain program rules or behaving in line with service/care providers' (or teachers', justice professionals', etc.) expectations, unless environmental adaptations or accommodations are made to fit with individuals' particular needs. An FASD-informed approach, thus, recognizes that to achieve positive outcomes, it is the system, program, and/or service providers who need to make modifications rather than the person with FASD.1,4,6,15,23,24
In addition, an FASD-informed approach recognizes that a person living with FASD also is likely to experience many social determinants of health risks (eg, poverty, homelessness or housing instability, unemployment or difficulties maintaining employment, low education, lack of social supports or social exclusion, racism, poor access to health services, early life adversity, vulnerability to violence, or victimization). Thus, in working with adults living with FASD, attention to the social determinants of health is essential.
Principles of an FASD-Informed Approach
As a starting point to considering what comprises FASD-informed practice and programming, it is important to identify the key principles that underpin the approach. Drawing on the emerging literature on FASD-informed practice1,4,6,19,23 and the more well-developed literature on trauma-informed practice, the author proposes that, as depicted in Figure 1, principles of an FASD-informed approach include:
Having awareness of FASD,
Making person-centered accommodations, and
Being strengths-based.

Principles of an FASD-informed approach.
Moreover, at the center of these are the principles of safety and being relationship based. Brief discussion of these principles within the context of becoming FASD-informed follows.
Having Awareness of FASD
Central to the principle of having awareness of FASD is recognizing that there is tremendous variability in the capabilities and challenges of those with FASD; equally importantly, due to the brain-based effects of FASD, the concept of developmental age is more useful than chronological age in providing a sense of a young person's or adult's functioning. 4 Consequently, it is those around the person with FASD – all of us, including policy makers, program developers, service providers, and support people – who will need to shift our expectations, rather than the person herself, to align with the individual's developmental level.
In addition, having awareness of FASD means taking a wholistic approach to programming and appreciating the multifaceted ways in which social determinants of health factors may affect the person's well-being or needs for support. The principle of awareness also includes the idea that FASD-related programs and services need not require service recipients to disclose having FASD or having had an assessment/ diagnosis of FASD. This is important given the reality that many if not most women/adults living with FASD will not have had access to a formal diagnosis, for reasons previously identified in this article.
Making Person-Centered Accommodations
The principle of making person-centered accommodations combines the following two key concepts: (a) being person-centered (or client-centered) and thus recognizing individuals' uniqueness and the heterogeneity that exists among people with FASD along with the value of an individualized approach; and (b) the need to make accommodations or modifications to programming in order to respond to FASD as a brain-based disability. 4
Being Strengths-Based
The third key principle underpinning an FASD-informed approach is being strengths-based. As discussed previously, young people and adults with FASD very often encounter challenges in school, employment, and daily living – to the extent that failure experiences and internalization of failure are common.4,18 Highlighting individuals' strengths and gifts is a pivotal means of countering service systems' predominant focus on problems and deficits and also counteracts our systems' standard approach of penalizing individuals for their difficulties. Being strengths-based may involve assisting young people and adults to identify their own strengths and abilities, since doing so may be an unfamiliar experience1,15; it may also mean recognizing and reframing problem behaviors as being understandable responses or coping mechanisms to stress, fatigue or trauma and then honoring these behaviors as reflective of resiliency.
Lastly, the principles of safety and being relationship-based are at the heart of this framework of FASD-informed principles. Placing safety and being relationship based at the center reflects appreciation that an FASD-informed approach begins by developing trusting, positive relationships, and creating environments in which the person feels safe physically and emotionally to share what is going on in her world. 27 The importance of the creation of safety also reflects recognition that many people with FASD may have experienced past, current, and/or intergenerational trauma, abuse, or violence, and thus, integrating FASD-informed and trauma-informed approaches is extremely important when working with women who may have FASD.1,25
FASD-Informed Accommodations in Practice, Programming, and Physical Environment
Moving from principles to practice, the following discussion is based on a synthesis of the selected research and practice wisdom related to FASD-informed approaches.14–16 For the purpose of this discussion, the FASD-informed accommodations have been organized into broad categories (practice, programming, and physical environment), although this categorization is not as important as appreciation that the areas of accommodations are interconnected, and all areas need to be put into place in order to provide effective and informed approaches to service delivery. In addition, it is important to note that the set of accommodations discussed in this article is not intended to be exhaustive; for additional discussion about these accommodations and others, perusal of the research and practice literature cited earlier is recommended.
Practice-Related FASD-Informed Accommodations
Programming-Related FASD-Informed Accommodations
Physical Environment-Related FASD-Informed Accommodations
In addition to practice and programming accommodations, research drawing on the wisdom of adults with FASD and service providers who regularly work with women with FASD has identified a number of accommodations or modifications to the physical environment that work well for adults with FASD.20,23,31 These include:
Paying attention to lighting and avoiding fluorescent lights or bright colors;
De-cluttering of noise/auditory stimuli (such as that related to electronics or the humming of lights and fans);
De-cluttering visual distractions;
Using visual aids, such as photographs of program staff on the office door;
Having calm, quiet space for interviews or meetings; and
Ensuring that the physical space is non-confining (for example, keeping the door slightly open) and that the person sees a clear way out. 31
Promising Programs for Women who may have FASD
While including a description of program(s) using an FASD-informed approach may be helpful to illustrate FASD-informed principles and practices ‘in action’, the author is aware that doing so may be problematic because of the frequently time-limited and/or fluid nature of social- or health-related programs (typically due to shifts or declines in program funding). Nevertheless, drawing from the literature on good practice in working with women with FASD, 20 two promising FASD-informed programs are summarized. These programs were identified through an environmental scan involving service providers in Western Canada who worked with women who had (behaviors and characteristics of) FASD. 20 The programs illustrate the FASD-informed principles and approaches described in this article.
Supportive Optimistic Advocacy Restorative (SOAR) mentor program: The SOAR mentor program provides mentoring, support, and assistance to women and their families with an aim of maintaining women's health and preventing alcohol-exploded pregnancies/births. The program is modeled after the Parent-Child Assistance Program developed in Seattle and was adapted for Indigenous women either who have used alcohol during pregnancy, who have given birth to a child who may have FASD, or who may have FASD themselves. The program was developed using an FASD lens and also emphasizes traditional cultural practices. SOAR uses a relational approach wherein the development of a trusting relationship between staff/mentors and women participants is central to the success of mentoring activities, advocacy, and personal growth and change. The program provides women with practical support (eg, transportation), case coordination, and access/advocacy relating to other services. An additional primary program activity is to help educate community and other service providers about FASD. Cultural involvement is a key: mentors connect women to their cultural identity using existing supports, elders and family. Caseloads for staff are reduced relative to other home visiting or mentoring programs (eg, caseload = 10–12 women).
Crabtree Corner FASD Peer Support program (offered through the YWCA, Vancouver): Crabtree Corner's FASD prevention program provides multifaceted support to pregnant and/or parenting women who are at high risk of having a child with prenatal alcohol exposure. Key features of this program include an emphasis on ensuring that staff have strong understanding of FASD, use of a relational approach, use of a strengths-based, wholistic and collaborative team approach in order to create a community of support in all aspects of the woman's life, and use of a trauma-informed approach.
Discussion
This article has emphasized that becoming FASD-informed is of critical importance to service providers, educators, program planners, policy makers, and researchers and of course to families living with FASD themselves. In considering what is involved becoming FASD-informed, the article has identified key principles underpinning an FASD-informed approach and discussed key elements of FASD-informed service delivery, including FASD-informed practice, programming, and adaptations to the physical environment.
As discussed in the emerging literature on FASD-informed practice, benefits of using an FASD-informed approach for service providers include better understanding of the challenges experienced by adults with FASD, stronger relationships with program participants and their families, avoidance of judgment and ascription of negative intent to behavioral issues that are actually brain-based (eg, lateness), reduced frustration, more constructive and effective problem solving, and higher job satisfaction. 1 For women living with FASD and their families, benefits are multifold, including trusting relationships with providers and support people, reduced stigmatization, a sense of being understood and accepted, trust that there is someone in their corner, improved self-esteem, self-confidence and hope, and better program success and retention.18–20
Taking the principles and elements of an FASD-informed approach beyond the level of individual service providers and programs, it is important to reflect on what an FASD-informed approach would look like at the community, policy, and/or systems levels. Clearly, knowledge on FASD and its ramifications, including its relationship to social determinants of health factors, is critical at a community level; similarly, community-wide professional development opportunities to deepen understanding about FASD-informed practice and trauma-informed practice and their interconnections would be important. At a policy and systems' levels, a true FASD-informed approach would reflect understanding of FASD as a lifelong issue; program funding, thus, would be in keeping with individuals' ongoing needs for support, and access to supportive interventions would be geared to developmental age and adaptive level rather than psychometric measures (such as IQ) that are not useful indicators of functioning for people with FASD. Furthermore, program funding would need to adequately provide for individuals' needs for outreach and one-to-one support, as well as group-based programming. Lastly, FASD-informed policies and systems would prioritize and strengthen the development, implementation, and evaluation of wholistic and integrated programs, including supportive housing and family foster care for women with FASD and their families. These elements of an FASD-informed approach would not only improve programs' efficacy and outcomes for women, families, and providers but also be pivotal to our endeavors in the prevention of FASD in future generations.
Author Contributions
Conceived and designed the experiments: DR. Analyzed the data: DR. Wrote the first draft of the manuscript: DR. Contributed to the writing of the manuscript: DR. Agree with manuscript results and conclusions: DR. Jointly developed the structure and arguments for the paper: DR. Made critical revisions and approved final version: DR. The author reviewed and approved of the final manuscript.
Footnotes
Acknowledgement
The author gives thanks to team members on the Toward an Evaluation Framework for FASD Prevention Programs project: Nancy Poole, Carol Hubberstey, Marilyn Van Bibber and Sharon Hume.