
Abstract
This paper presents a new initiative in the South-Eastern Health Region of Norway to establish a regional resource center focusing on services for children and adolescents aged 2–18 years with prenatal exposure to alcohol or other drugs. In Norway, the prevalence of fetal alcohol spectrum (FAS) is not known but has been estimated to be between 1 and 2 children per 1000 births, while the prevalence of prenatal exposure to illicit drugs is unknown. The resource center is the first of its kind in Scandinavia and will have three main objectives: (1) provide hospital staff, community health and child welfare personnel, and special educators with information, educational courses, and seminars focused on the identification, diagnosis, and treatment of children with a history of prenatal alcohol/drug exposure; (2) provide specialized health services, such as diagnostic services and intervention planning, for children referred from hospitals in the South-Eastern Health Region of Norway; and (3) initiate multicenter studies focusing on the diagnostic process and evaluation of interventions.
Keywords
Background
Fetal alcohol spectrum disorders
Alcohol is a teratogen, and its direct adverse effect on the development of a fetus is greater than any other known psychoactive substance. In addition, alcohol is special compared to other teratogens since it is frequently and widely used by women in most countries of the world. Damage to the central nervous system due to prenatal alcohol exposure is considered the most common known cause of mental retardation worldwide. 1 There is currently no diagnostic code (ICD-10) related to prenatal exposure to drugs other than alcohol.
Fetal alcohol spectrum disorders (FASD) is an umbrella term describing a spectrum of medical, developmental, cognitive, motor, and behavioral disabilities in children with prenatal alcohol exposure. The term includes children with full fetal alcohol syndrome (FAS), fetal alcohol effects (FAEs) or partial FAS, alcohol-related birth defects (ARBDs), and alcohol-related neurodevelopmental disorder (ARND). The link between prenatal alcohol exposure and adverse outcome for the child has been postulated in both the Bible and the Talmud, but the first scientific papers describing common features in children exposed to alcohol in utero were published in 1968 in French 2 and in 1972 in English. 3
The term FAS was introduced in 1973 as a description of children with a common pattern of face deformities and alcohol-dependent mothers. 4 Since then, FAS has achieved a diagnostic code (ie, Q86.0) in the International Statistical Classification of Diseases and Related Health Problems, version 10 (ICD-10, 1994). However, the diagnostic assessment process for FAS/FASD is still debated, and at least four different diagnostic systems are currently in use in Canada and the United States.5–7 Recently, one of the most recognized systems, the 4-Digit Diagnostic Code System, has been extensively validated the FASD diagnostic code. 8 In 2013, German FAS guidelines were published based on literature reviews, 9 but no clinically evaluated guidelines exist from Europe. Each diagnostic system has its advantages and challenges, and no common agreement exists regarding which one to use.
Clinical characteristics of FAS/FASD
Diagnostic systems for evaluating FAS/FASD use a combination of growth retardation, special facial features, structural and functional central nervous system (CNS) deficits, and information about alcohol consumption during pregnancy as the basis for diagnosing FAS, but the exact criteria differ somewhat between the different diagnostic systems. Fetal growth restriction increases the risk for being born small for gestational age (SGA) with reduced head circumference. Postnatal growth may also be delayed or inadequate. Typical facial features in FAS include small eye openings, smooth and wide philtrum, and thin upper lip, and the presence of all these characteristics has a very high specificity for FAS. Many children with FASD will present with developmental delays, and although many children with FASD have intelligence quotient (IQ) within the normal range, attention deficits, working memory problems, hyperactivity, impulsivity, and arrested social development are common and reflect the static brain injury.
Prevalence, risk factors, and cost of FASD
Estimating the prevalence of FASD poses a major challenge since data are largely based on retrospective maternal reports, and the fear of social stigma likely leads to underreporting. 10 In addition, women may have difficulty remembering when they first became aware of their pregnancy and consequently stopped consuming alcohol and how much they may have consumed prior to that point. These methodological challenges could explain the relatively large variance in reported prevalence rates.
Within the United States, the prevalence of FAS and FASD has been estimated to be as high as 6–9 per 1000 live births and 2.4%–4.8%, respectively. 11 Canadian estimates for FASD are 8.2–15.1 per 1000 births. 12 Within the childcare system, the number of children affected maybe as high as 6% with FAS and 16.9% with FASD based on a recent meta-analysis. 13 There are few studies from Europe regarding the prevalence of FASD, but an Italian study 14 reported a prevalence of 3.7–7.4 per 1000 live births for FAS and 2.3%–4.1% for FASD. In a hospital-based study from 1985, the prevalence of FASD in Norway was estimated at 0.5–1 per 1000, 15 but more comprehensive studies are needed as the actual prevalence may be significantly higher. A more recent study reported that 25% of women consume some alcohol during pregnancy in Norway. 16 A white paper (Meld. St. 30; See Me! A comprehensive drug policy. In: Stortingsmelding 2012) estimated the incidence of FAS in Norway to be between 60 and 120 children a year, ie, 1–2 per 1000 live births. In addition, children who are adopted in Norway from countries with a higher prevalence of FASD have increased risk of FASD. This is supported by findings from Sweden, indicating an FASD prevalence of more than 50% among children adopted from Eastern Europe. 17 Increased awareness of FASD can also contribute to higher prevalence estimates. Elgen et al. 18 estimated the prevalence of FASD to be 0.3 per 1000 based on questionnaires completed by Norwegian health professionals, but following an educational course on FASD, the prevalence of diagnosed FASD increased to 1.5 per 1000. Such findings suggest that interventions aimed at enhancing knowledge among health professionals can improve identification of FASD, and thereby increase the number of children diagnosed.
The toxic effects of alcohol in utero are dependent on the amount, frequency, and duration of exposure, although other maternal and environmental risk factors also contribute to child outcomes. In a recent review paper, May and Gossage 19 present a comprehensive overview of maternal risk factors that can modify the outcome in children with FASD. Maternal factors include age, the number of pregnancies and children, previous still births/miscarriage, low education, smoking/drug use, psychological distress, short stature, low body mass index (BMI), low weight, nutritional deficiency, and alcohol dehydrogenase polymorphisms. Environmental risk factors for FASD include low socioeconomic status, cultural acceptance of heavy drinking, maternal partner who drinks heavily, and little parental knowledge about FASD. 19
Children with FASD or other prenatal drug exposure have a high incidence of primary and secondary deficits that demand specialized healthcare and multidisciplinary expertise. In a systematic review on economic costs related to FASD, Popova et al. 20 identified a total of 13 studies, ten from the US and three from Canada. Although no Norwegian cost studies exist, the Canadian studies are likely relevant given the similarities in their public healthcare and education systems. In the most recent Canadian study, Stade et al. 21 estimated an annual cost per FASD child of 21,642 Canadian dollars (95% CI: $19,842–$24,041), while the annual costs for all persons born with FASD (0–53 years of age) were estimated to be about 5.3 billion Canadian dollars based on a conservative FASD prevalence of 0.3%. In addition to the direct costs, FASD also results in indirect costs through the increased burden on the family due to the child's primary and secondary disabilities. Equally hard to quantify in economic terms is the child's burden of living with FASD in terms of reduced health-related quality of life compared to both healthy controls and children born with extremely low birth weight. 22
The Regional Resource Center for Children with Prenatal Alcohol/drug Exposure
In the 2005 report “Alcohol and Pregnancy” by the Norwegian Health and Social Affairs, the establishment of resource centers for children and adolescents with congenital drug exposure was recommended (https://helsedirektoratet.no/Lists/Publikasjoner/Attachments/24/Alkohol-og-graviditet-hva-er-farlig-for-fosteret-hvordan-forebygge-og-behan-dle-IS-1284.pdf). This white paper stated that current specialist health services for children and adolescents with congenital drug injury were not satisfactory and that there was a particular need for multidisciplinary teams of health professionals, with specific competence in the effects of prenatal alcohol and drug exposure, to diagnose FAS and evaluate FASD. In 2008, a Nordic workshop titled “Assessment and diagnosis of children, adolescents and adults who have been exposed to drugs in utero” was conducted, which concluded that key expertise in this field in Norway was required. In 2012, the Department of Child Neurology and Rehabilitation, Sørlandet Hospital, submitted an application to become a regional resource center for children and adolescents with prenatal alcohol/drug exposure, and the application was approved in March 2015. The establishment of a regional resource center, therefore, represents the culmination of a decade of work to bring forth a multidisciplinary service that aims to diagnose, treat, and safeguard these children beyond early childhood to prevent secondary disabilities and improve the long-term prognosis for this rather neglected patient group.
Organization of the Norwegian health system
The Norwegian health system is, with a few exceptions, entirely public and organized into four regional health authorities (Fig. 1; Norwegian: Regionalt helseforetak or RHF).

Map illustrating the four health regions of Norway.
The South-Eastern Health Region is the largest one, providing specialist health services to 2.8 million people (56% of the Norwegian population). The Department of Child Neurology and Rehabilitation at Sørlandet Hospital is one of the eight Health Trusts in the South-Eastern Health Region and has received local patients with prenatal drug exposure, primarily alcohol, since 1996 (total population served by the hospital is 300,000). The Regional Resource Center will serve the entire South-Eastern Norwegian health region (total population: 2.8 million). Prior to the establishment of the Regional Resource Center, our department's services focused primarily on diagnosing FASD, although patients exposed to other drugs have also been offered multidisciplinary assessment and follow-up. In the past, children have been referred by their primary physician, but to ensure a close collaboration between the Regional Resource Center, the family, and their local hospital, referrals to the Regional Resource Center will be required to come from the specialist healthcare system (child psychiatry department, child neurology/rehabilitation department, or pediatric department).
In addition to conducting clinical assessments, professionals from our department have taught under the auspices of the Directorate of Health and KoRus-sør/Borgestadklinikken, which is part of the specialized public health system in Norway and was established in 2008 as a resource center for adults with substance dependence problems. KoRus/Borgestadklinikken serves adult patients and is responsible for the treatment and follow-up of pregnant women with alcohol or drug addiction living in the South-Eastern Health Region.
Courses have been developed by our department for community health professionals, the child welfare system, caregivers, and special educators, and there have been more than 1000 attendees so far. Over the years, the number of medical referrals of children with possible FASD has increased in Norway, probably as a result of several nationwide information campaigns initiated by the Directorate of Health (https://helsedirektoratet.no/english/about-the-norwegian-directorate-of-health) and educational courses for health professionals, which make them more likely to ask about prenatal drug exposure. The increased number of referrals clearly indicates the need for clinical services, teaching, and research focused specifically on this vulnerable clinical group.
Aims and directives of the Regional Resource Center for children with prenatal alcohol or other drug exposure
The primary aim of the Regional Resource Center is to collect, systematize, and share knowledge regarding the diagnostic process, assessments, and interventions for children with FASD or prenatal drug exposure (PDE) in the South-Eastern Health Region of Norway. The following directives have been received from the South-Eastern Regional Health Authority:
Develop and provide educational courses focusing on relevant diagnostic tools for the specialized (secondary) health services and develop guidelines for the diagnostic process, assessment, and follow-up of this patient group.
A major challenge in mapping the incidence of alcohol/drug exposed children has been the lack of a common diagnostic system that includes the whole spectrum of neurological deficits related to prenatal alcohol exposure, as the teratogenic effects exist on a continuum. 23 No specific guidelines exist for Scandinavia or Norway. The Department of Child Neurology and Rehabilitation at Sørlandet Hospital, Arendal, has adopted the 4-Digit Diagnostic Code as our method for diagnosing FASD since this diagnostic system is the only one that has been extensively validated. 8 One of our aims will be to implement the systematic use of this diagnostic system throughout the whole South-East Health Region in Norway.
Evaluate and share relevant intervention and treatment measures and initiate multicenter research projects related to FASD.
Given the estimated prevalence of FASD and prenatal drug exposure, there is an astonishing lack of studies evaluating the special education and medical interventions that are offered to these children after they have been diagnosed, 24 and there are no studies from Norway. The lack of intervention studies was illustrated in a 2009 systematic review, which found only 12 studies that were either randomized controlled trials (RCTs), quasi RCTs, case–control studies, or pre- and post-intervention studies, 25 and a subsequent study has confirmed this finding. 26 Three studies, two of which were RCTs, including a total of 43 children with FASD aged 6–16 years, focused on the pharmacological treatment of symptoms of hyperactivity/impulsivity and inattention. Results indicated significant reduction of hyperactivity/impulsivity as evaluated by parents and teachers but no effect on symptoms of inattention. With regard to educational interventions, Peadon et al. 25 concluded that RCT studies document their positive effects on language function (reading, spelling, and pre-literacy skills) and mathematics. Specific training on attention, cognitive control, social skills, and the use of virtual reality also showed promising results in improving attention, learning, and behavior. The Consortium for Intervention for Children with FASD presented five research projects in 2009 focused on reducing behavioral problems and improving social skills, behavior, mathematics, and executive function. 27 Based on these studies, the inclusion of parental education and training and direct instruction to the child were critical factors for success. Although the number of intervention studies has increased in recent years,28,29 more studies are needed to evaluate the effectiveness of the interventions and confirm which components of the interventions are critical to ensuring positive outcomes.
To address gaps in the research literature, the Regional Resource Center will initiate research focused on children who have been diagnosed with FASD. This will be done by inviting departments of pediatrics, child neurology/rehabilitation, and child psychiatry to participate in multicenter studies to investigate promising intervention methods and to evaluate their applicability and effectiveness for children with FASD.
Establish a network for health professionals who perform clinical assessments of children with prenatal alcohol or drug exposure and develop guidelines for assessment and follow-up of children with FASD to be used within the South-Eastern Health Region.
The lack of objective assessment measures for diagnosing FASD and/or prenatal drug exposure represents a challenge for medical doctors throughout the diagnostic process. By establishing a network, health professionals will be able to share experiences from their clinical work. Establishing regional guidelines will provide a common basis for research collaborations, enabling larger study samples for evaluating the interventions these children are offered within our health region.
Teaching community health workers how to identify, follow up, and provide interventions to children with FASD in collaboration with the specialist health services, and develop educational material that will be used to train local community health workers.
Follow-up studies of children with FASD into adolescence and adulthood in Europe30–32 and in the US 33 clearly indicate a high risk for a variety of negative long-term outcomes. Based on the knowledge that early diagnosis and recognition of primary challenges in children with FASD may improve the long-term outcome by reducing secondary disability,33,34 offering educational courses to healthcare workers will be a priority for the Resource Center. Increasing primary healthcare workers’ knowledge about brain injuries as possible consequences of prenatal alcohol or drug exposure has been shown to increase the number of referrals for diagnostic evaluation. 18 In the western part of Norway, providing basic education regarding FASD to healthcare professionals increased the prevalence of FASD from 0.3 to 1.5 per 1000 based on questionnaires, supporting the view that lack of knowledge regarding FASD contributes to underdiagnosis. 18
Educational courses about FASD diagnostics, assessments, and interventions will be offered to health professionals in hospitals and in primary healthcare settings, and to community social workers, special educators, and caregivers throughout the South-Eastern Health Region.
The Regional Resource Center has developed and will continue to provide four different types of courses:
Educational seminars aimed at community service providers (child welfare personnel, teachers, and special educators) and caregivers (foster parents, adoptive parents, and biological parents). These courses run for one full day and focus on the prevalence of FASD/PDE, clinical characteristics, the diagnostic process and interventions to be used at home and in kindergarten/school. These courses are given by a clinical neuropsychologist and a neuropediatrician, both with expertise in the field.
Diagnostic courses aimed at medical doctors (general practitioners, neurologists, pediatricians, child psychiatrists) and psychologists (clinical and neuropsychologists). This course runs for 2 full days and are taught by the same specialists as for the educational seminars. Day 1 focuses on the clinical characteristics and prevalence of FASD as well as multidisciplinary methods for assessment, common clinical findings, and symptomatology with consequences for intervention and treatment planning. Day 2 focuses on the diagnostic process with practical training in the usage of the 4-Digit Diagnostic Code System 35 and includes discussion of case presentations and exchange of experience.
Individual patient courses are developed and targeted to a specific child with FASD/PDE. These courses usually run for 3–5 hours. The target group includes both personnel who work directly with the child in school (assistants, teachers, special educators) and family (caregivers, grandparents, significant others). Personnel providing educational and psychological services in the community, the family doctor, and others involved with the child are also invited. The content of these courses may vary, but typically includes general information about FASD, followed by presentation and discussion of the multidisciplinary examination results, and suggestions and advice regarding treatment and interventions at home and at school. Participants are encouraged to ask questions and give examples regarding problem behaviors, learning challenges, and interventions. Special educators and clinical neuropsychologists lead these courses.
Intervention seminars aimed at both community and specialist healthcare professionals as well as special educators. This seminar runs for 1–2 full days and is taught by special educators, clinical neuropsychologists, and a pediatric physiotherapist. The seminar focuses on presenting different intervention techniques for children with FASD from infancy through childhood, adolescence, and young adulthood by reviewing existing literature, sharing clinical experience, and discussing intervention options within the Norwegian healthcare and school system.
Educational and diagnostic courses about FASD and intervention seminars will be offered at least twice every year within the South-Eastern Health Region. In addition, courses focused on the needs of specific patients will be offered on an ongoing basis.
Clinical services to be offered at the Regional Resource Center
The model for assessment, diagnosis, and follow-up developed at the Department of Child Neurology and Rehabilitation at Sørlandet Hospital has evolved over the years since 1996. It has been continuously revised based on clinical experience and feedback from the families attending our clinic. The model was primarily aimed at children from 2 to 18 years of age with confirmed prenatal alcohol exposure, but it has also been effective for children with other types of prenatal drug exposure. Our model is similar to that of the Washington State Fetal Alcohol Syndrome Diagnostic & Prevention Network at the University of Washington (http://depts.washington.edu/fasdpn/index.htm), as the core of both models is a multidisciplinary approach throughout the diagnostic process. Our department receives referrals primarily from two local hospitals, but during the last 5 years an increasing number of referrals have come from hospitals across the entire health region as well as from other parts of Norway. Currently, most children are referred in late childhood or adolescence, while a few children are diagnosed at birth or in early childhood. We believe, based on previous experience, 18 that offering educational courses to healthcare professionals will increase the number of referrals and decrease the age at which children are referred, and thereby improve their long-term prognosis. 33
In- and out-patient services at the Regional Resource Center for prenatal alcohol/drug exposure
The newly established Regional Resource Center will accept referrals from the entire southeastern part of Norway. Since some patients will have to travel long distances, both in- and out-patient services are offered. The Department of Pediatrics at Sørlandet Hospital is located in close proximity to our Department of Child Neurology and Rehabilitation, which is an advantage for the referred children who are in need of supplemental medical examinations during their stay. Sørlandet Hospital also offers a patient hotel on the premises. Our department can book rooms for the family to stay at the hospital hotel for the duration of the assessment and diagnostic process. If the family lives within reasonable distance from the hospital, we may offer an outpatient service where the family meets for appointments with our professionals for 2–3 consecutive days. The feedback provided from families who have gone through this diagnostic process is that they prefer the evaluations to be done intensively over several days instead of coming back for further assessment over a longer time period. Duration of the diagnostic process is dependent on what background information is available at the time of assessment.
The Regional Resource Center has an experienced social worker who will establish contact directly with the family (and child welfare services in cases involving foster parents) at the time of referral and coordinate with them to collect relevant information from previous assessments as well as background information. The social worker will function as the family's primary contact throughout the diagnostic process. In our experience, most children with prenatal alcohol or drug exposure who experience behavioral, cognitive, or psychiatric problems have been through several assessments at different agencies and health services before being referred to our department. Collecting results and reports from these assessments provides an important source of information about the child's development and challenges over time. Being able to review this information as a whole often brings forth a new understanding of the child, clarifies what supplementary assessments are needed, and thereby reduces the length of stay. Prior to admission, the social worker prepares a summary of the case to be reviewed by the multidisciplinary team, and then a detailed and individualized assessment plan is created. Referrals for supplementary medical examinations, such as cerebral magnetic resonance imaging (MRI) and electroencephalography (EEG), are also prepared at this time. A point-by-point daily schedule is sent to the family prior to admission, specifying who they will meet at the center, what assessments will be performed at what time, and any planned additional examinations. This enables the caregivers to prepare the child for the stay and the different assessments. If blood samples are needed, the family may be asked to contact their primary physician to perform these prior to admission to our hospital.
Multidisciplinary assessment of children with FASD/ prenatal drug exposure
The multidisciplinary team at the Regional Resource Center includes a clinical neuropsychologist (100% position), a neuropediatrician (50% position), a child psychiatrist (25% position), a pediatric physiotherapist (25% position), and a social worker (50% position). The head of the center is a neuropsychologist. In total, the center has 3.6 positions. The assessments are tailored to the individual patients and are dependent on previous assessments/examinations as well as the age of the patient. On arrival, the patient and their family are met by the social worker they have been in contact with prior to admission. All participating team members then meet the family at the same time to introduce themselves and get to know the patient. Neurological and motor assessments are conducted collaboratively by the neuropediatrician and the pediatric physiotherapist. Cognitive testing is conducted by the psychologist in a separate room, with one of the caregivers accompanying the child if needed.
The role of the different professionals at the Regional Resource Center
The neuropediatrician
Important tasks for the neuropediatrician include the diagnostic process, use of the 4-Digit Diagnostic Code, differential diagnoses, and evaluation of psychomotor development and the need for supplemental medical examinations such as genotyping, sensory examinations (vision and hearing), EEG, and cerebral MRI. Major differential diagnoses that have to be ruled out include congenital and genetic syndromes. Syndrome searches using established syndrome databases such as Pictures Of Standard Syndromes and Undiagnosed Malformations (POSSUM - http://www.biobase-international.com/product/possumweb) and the Winter–Baraitser Dysmorphology Database (WBDD – http://www.lmdatabases.com/about_lmd.html) will be combined with microarray-based comparative genomic hybridization (CGH) and fluorescence in situ hybridization (FISH). The prevalence of seizures is 3%–21% in children with FASD, compared to 0.32%–0.55% in the general population. 36 Due to the higher incidence of seizures and epilepsy in patients with FASD, a higher incidence of pathological findings on EEG is expected. Few studies have systematically examined the EEG records of adolescents and children with FAS/FASD, and EEG features in this patient group are poorly described.37,38 One study reported significant reductions in the mean power of the alpha frequencies (7.5–12 Hz) while doing a spectral analysis. 39 All patients admitted to our resource center will undergo a long-term EEG recording using a standardized EEG protocol. The protocol includes a 2-hour, 20-channel video EEG registration (international 10–20 system). Part of this registration will be a defined period with closed eyes, hyperventilation, and photo-stimulation. A neuropediatrician participating in the multidisciplinary assessment process will be responsible for reading and interpreting the EEG and providing antiepileptic treatment suggestions when indicated. Cerebral MRI is important for identifying structural abnormalities such as malformations, general atrophy, and dilatation of the ventricular system and thinning of the corpus callosum.40,41 However, if general anesthesia is required, a cerebral MRI may be postponed until the child can cooperate in an awakened condition. When more quantitative sequences are implemented in clinical practice, the value of cerebral MRI in the diagnosis of FASD will be increased. In the Regional Resource Center, the indication for doing structural MRI will be individualized.
Child psychiatrist
In patients with FASD, there is a high incidence of secondary disability in the form of psychiatric conditions, which increases with age.42,43 Fagerlund et al. 23 reported that the main risk factor for secondary psychiatric problems in children with FASD was time in residential care as well as the absence of dysmorphic features, supporting the need for assessing the whole spectrum of fetal alcohol disorders, not only FAS. Prevalence of attention deficit hyperactivity disorder (ADHD) is especially high in children with FASD. In a Norwegian study, 86% of children with FASD and 100% of children with prenatal psychotropic drug exposure fulfilled the diagnostic criteria for ADHD. 44 The child psychiatrist participates in the multidisciplinary assessment process and is responsible for the psychiatric evaluation, which includes obtaining a detailed family history as well as assessing the child's mental health. If the diagnostic criteria for ADHD or other mental health conditions are met, the appropriate diagnoses are made and recommendations regarding treatment are outlined.
Clinical neuropsychologist
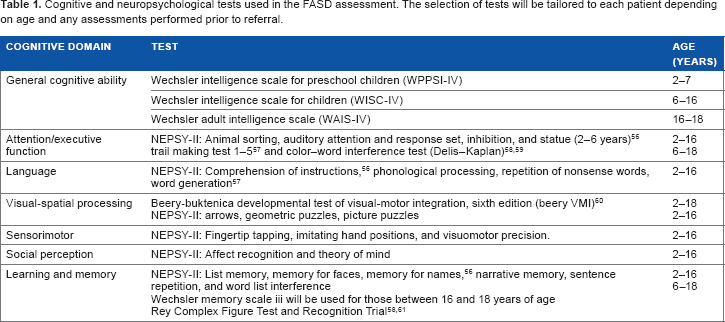
Primary disabilities in children with FASD include intellectual disability and learning disorders.45,46 Even in children with FASD without global cognitive impairment, neuropsychological deficits are still prevalent, 47 indicating the need for comprehensive neuropsychological assessment. Children with FASD have deficits in attention, concentration, and impulse inhibition, 48 which can make the neuropsychological assessments demanding for the child. This is addressed by providing enough time to carry out the assessments at the child's pace with adequate breaks and other alternating activities. Children with FASD are also characterized clinically by high variability in functioning from day to day, as well as within each day. Performing the assessments requires that professionals are experienced so that they can adapt the methods and sequence of examinations to the child's focus and as their motivation changes. To accommodate this, the cognitive testing is usually divided into two daily sessions for 2–3 days. How extensive the neuropsychological testing will be depends on the assessments that have already been done by the referring health services. The neuropsychological test protocol is also adjusted according to the child's age. Standardized, internationally recognized tests that have been validated as sensitive to the cognitive deficits seen in children with FASD will be used. When Scandinavian norms are not available, similar tasks or tasks based on our own clinical experience may be used instead (Table 1). Assessments will always include the child's IQ, as well as tasks assessing the following cognitive domains: attention/executive, language, visual-motor, sensory-motor, learning, and memory.
Cognitive and neuropsychological tests used in the FASD assessment. The selection of tests will be tailored to each patient depending on age and any assessments performed prior to referral.
Pediatric physiotherapist
Children with FASD have increased risk of gross motor deficits 49 and poorer fine motor abilities, 50 which affect handwriting and academic functioning. 51 Our specialist in pediatric physiotherapy will perform the Movement Assessment Battery for Children, second edition (MABC-2), 52 and the Motor Function Neurological Assessment (MFNU), the latter being especially sensitive to subtle motor problems in children with ADHD. 53 If the assessment results indicate motor impairments, suggestions for physiotherapy will be provided and collaboration will be established with the local physiotherapist.
Social worker
In addition to serving as the primary contact for the family prior to admission and throughout the assessment, the social worker plays a key role in assessing the child's daily life functioning in order to address the need for health and community services from a family-centered perspective. Several studies have reported deficits in adaptive behavior among children with FASD.8,33,54 Adaptive behavior may be defined as the effectiveness or degree to which individuals meet the standards of personal independence and social responsibility expected for age and cultural group. 55 A comparison of patients with different degrees of FASD revealed that all had adaptive behavior deficits with scores more than 2 SD (standard deviation) below age-appropriate levels. 8 In our clinic, the social worker is highly experienced in the use of the Scandinavian version of Vineland Adaptive Behavior Scales, second edition (VABS-2). The VABS is administered to the child's caregivers in a semistructured interview, while their teachers are asked to complete the teacher questionnaire. In our experience, the VABS is a useful tool for obtaining extensive information about the child's daily life functioning, including the challenges. The VABS is interpreted by the social worker in collaboration with the clinical neuropsychologist.
Research activities at the Regional Resource Center
The limited number of scientific studies focusing on FASD and prenatal drug exposure in Norway may be related to the lack of collaboration between clinical and research settings. Establishing this resource center will provide an opportunity to bridge this gap by initiating multicenter studies. At least two of those working at the Regional Resource Center will have extensive research competence. In addition, planned clinical research projects will include at least two PhD positions, such as one for a medical doctor and one for a clinical neuropsychologist, provided sufficient funding is obtained. A combination of clinics and research aimed at diagnosis and treatment will generate research results that can benefit patients quickly. It allows for close monitoring and evaluation of measures and systematic testing of treatment interventions in terms of improvement of function and prevention of secondary disabilities. All patients will be potential candidates for this type of research after approval from the ethics committee and informed consent. The Regional Resource Center will also generate a clinical database that will be used in research. Planned research activities include prospective follow-up of children with FASD and PDE, in which multidisciplinary clinical assessments will be related to quantitative MRI and EEG findings in order to reveal brain structure–function relationships. The Regional Resource Center has medical doctors experienced in the use of multimodal MRI in developmental brain research. Longitudinal measurements of brain structure volumes, cortical morphometrics, and white matter connectivity will be performed. Sørlandet Hospital has implemented MRI scanners with hardware and software for automated brain segmentation and diffusion tensor imaging. In addition, the center collaborates with international partners experienced in MRI analysis and long-term follow-up of children with prenatal alcohol/PDE from the University of Hawaii.
Summary
The overall aim of the Regional Resource Center for prenatal alcohol/drug exposure is to ensure that all children with FASD are identified, properly assessed, and provided with appropriate interventions to optimize their development and prevent secondary disabilities. To accomplish this, increasing awareness about this patient group and its extensive needs among health professionals and in the general population will be a priority.
Author Contributions
Conceived and designed the paper: GCCL, JS. Wrote the first draft of the manuscript: GCCL, TG, JS. Contributed to the writing of the manuscript: GCCL, JS, BL, CS, MMF. Agreed with manuscript results and conclusions, jointly developed the structure and arguments for the paper, and made critical revisions and approved the final version: GCCL, JS, BL, CS, MMF, TG. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We thank Professor Susan Astley, Department of Epidemiology in the School of Public Health at University of Washington, Director of the Washington State Fetal Alcohol Syndrome Diagnostic and Prevention Network and her team for sharing their knowledge and for their continuous effort for children with FASD. We would also like to thank the Program Director of Neuroscience and MR Research, Professor Linda Chang, MD, Professor Thomas Ernst and Dr. Vanessa Douet, University of Hawaii, USA, for collaborating and sharing their expertise in MRI and prenatal alcohol/PDE. We would like to thank the Director Jan Roger Olsen and the Assistant Director Per Engstrand, MD, Sørlandet Hospital, as well as the Head of the Department for Clinical Medicine, Nina Iversen, MD, and the Head of the Pediatric Department, Kåre Danielsen, MD, at Sørlandet Hospital for their continued support throughout the application process. We would also like to thank the staff at KoRus/Borgestadklinikken and at the Department of Child Neurology and Rehabilitation at Sørlandet Hospital for their support and collaboration.