
Abstract
Objectives
Fetal alcohol spectrum disorders (FASD) affect the health and development of people across the lifespan. Adults with FASD experience significant barriers to care. Accessible and scalable solutions are needed. In partnership with members of the International Adult Leadership Collaborative of FASD Changemakers, an international group of adults with FASD, we developed a mobile health (mHealth) application based on self-determination theory (SDT), called “My Health Coach,” to promote self-management and health advocacy.
Methods
This project follows an established user-centered design approach to app development and evaluation, allowing for feedback loops promoting iterative change. Research staff and ALC members co-led online focus groups (n = 26) and an online follow-up survey (n = 26) with adults with FASD to elicit feedback on completed design prototypes. Focus group transcriptions and surveys underwent systemic thematic and theoretical framework analysis.
Results
Analyses show overall positive impressions of the My Health Coach app. Participants were enthusiastic about the proposed features and tools the app will provide. Discussions and free responses revealed SDT constructs (autonomy, competence, relatedness) are a strong fit with participants’ perceived outcomes shared in their evaluation of the prototype. Interesting recommendations were made for additional features that would further promote SDT constructs.
Conclusions
This project demonstrates advantages of community-engaged partnerships in FASD research. Adults with FASD have a strong interest in scalable mHealth tools and described the acceptability of our initial design. App features and tools promoted SDT constructs.
Keywords
Introduction
Prenatal alcohol exposure (PAE) can affect the developing brain and other organ systems, which can result in a set of developmental disabilities termed fetal alcohol spectrum disorders (FASD). 1 FASD are prevalent disabilities, affecting about 1.1% to 5% of children in the United States. 2 Diagnostic criteria for FASD involve details regarding prenatal alcohol exposure, characteristic facial features, growth patterns, neurological differences (e.g. microcephaly, seizures, structural brain differences), and neurobehavioral functioning. 1 Specific diagnoses on the fetal alcohol spectrum, such as fetal alcohol syndrome, partial fetal alcohol syndrome, and alcohol-related neurodevelopmental disorder, depend on which characteristic features are present.
Although FASD have been primarily studied in children, it is well established that they are life-long conditions that impact multiple domains of functioning. 3 Adults with FASD often require a higher level of supports to participate in home, community, occupational, and social settings. 4 Despite the high prevalence, most people with FASD do not receive appropriate diagnoses or services. Research has documented that 80% or more of people with FASD go undiagnosed. 5 Barriers to appropriate services stem in part from sparse research literature and lack of systematic provider training.6,7 Furthermore, there is limited, largely deficit-focused, and stigmatizing information available online.7,8
Despite fetal alcohol syndrome being recognized in the United States since 1973, 9 there remains many unknowns about how PAE affects individuals in adulthood or throughout the aging process. The adult literature on FASD is limited and the average age in most adult studies is 25 years (for a review, see Ref. 3 ). Longitudinal studies document that facial characteristics and growth delays, when present, can diminish over time for some individuals; however, neurobehavioral impairments appear to persist over the life course. This limited body of research 3 documents difficulties with attention, learning and memory, planning, task efficiency, and analyzing social situations. Adults with FASD feel less confident coping with their environment and display higher levels of self-reported behavior problems and mental health conditions. 10 Likely a result of many of these neurobehavioral challenges, adults with FASD have lower adaptive functioning and many require a moderate to high level of supports from others. Emerging research is also documenting important strengths in individuals with FASD including social relationships and prosocial behaviors, specific talents and passions, and resilience.11–13
Adults with FASD have played an active role in adding to this limited body of work and bringing attention to these important issues, especially physical health and quality of life indicators in FASD. Specifically, several leaders in the FASD community have come together, establishing a group called the International Adult Leadership Collaborative (ALC) of the FASD Changemakers. The ALC established a central organizing theme of “Nothing About Us Without Us” for adult programming at the International Conference on FASD held annually in Vancouver, BC. They also developed two surveys about physical health symptoms and quality of life for adults with FASD, respectively. Each survey elicited responses from over 500 of their peers. The first survey's results were presented at the 2017 International FASD Conference in Vancouver 14 and were recently published. 15
The ALC's survey findings revealed that compared to the general population, adults with FASD have elevated rates of autoimmune disorders, cardiovascular disease, diabetes, thyroid disorders, digestive disorders, and mental health problems, among others. 15 The ALC also spoke about the trials and tribulations of managing their health conditions. They described experiences with health providers who did not take reported symptoms seriously and their wide-ranging difficulties in self-advocacy. They also highlighted problems for some adults with FASD in understanding and following a medication regimen and other treatment advice. This arose from a mismatch between how information was presented and the constraints of their individually variable neurobehavioral impairments.
This dearth of research, coupled with FASD often being missed or misdiagnosed, 5 means it is extremely difficult for adults to obtain effective supports and services. 4 Systematic reviews of FASD intervention research 16 have identified only two studies with adults, both involving case management approaches targeting parenting outcomes.17,18 Thus, no research-backed interventions exist for the many physical and mental health challenges reported by the ALC in their seminal research. Further, there are major barriers to accessing existing services and supports in the community including but not limited to: individual- and family-level barriers such as limited financial resources and inability to access childcare; lack of FASD-informed community providers; FASD not being a qualifying diagnosis in existing systems of care; and stigma.6,19 Additional barriers exist for accessing FASD-informed resources online: much of what can be found online about FASD is contradictory, unverifiable, and even frightening. Information is often stigmatizing and not written at an appropriate literacy level. Suggestions and research are deficit-focused rather than strengths-based. 8 Scalable, strengths-based, and evidence-backed solutions are needed.
Increasingly, technology is being harnessed to support or deliver care for physical and mental health problems across the lifespan and has significant potential to increase access to FASD-informed resources and care.20,21 The use of mobile health (mHealth) technologies has bourgeoned since the emergence of app stores in 2008. 22 mHealth has many advantages, including increasing healthcare capacity, providing patient access to tailored and immediate support, reducing stigma in accessing care, and improving cost-effectiveness. 23 Unfortunately, very few apps undergo any type of rigorous evaluation. 24 Additionally, very few studies have examined the efficacy of mHealth interventions for people with developmental disabilities, despite the higher prevalence of co-occurring conditions in this population. 25 Recent studies have shown that people with developmental disabilities have rates of smartphone ownership and usage in line with those of the overall population. 26 Given high rates of health disparities and universal access to smartphones, adults with developmental disabilities are good candidates for mHealth interventions. mHealth apps also have the potential to increase independence in the self-management of important activities of daily living, which is a salient goal for many adults with developmental disabilities.
My Health Coach: a novel mHealth app for adults with FASD
Our mHealth app, My Health Coach, is being developed through a partnership between researchers at the University of Rochester (UR) and the ALC. This app is being designed to offer adults with FASD evidence-based education about their condition and tools to promote their own self-management and health advocacy goals. Members of the ALC have served as an advisory board, co-developed the app prototype, and co-led the conduction of the presented research. Partnering with the ALC to develop and conduct the research is an important strength of this study. Gathering community input is crucial when developing new treatments and supports for a given condition. 27 Additionally, partnering with identified leaders in the community helps to shape the research questions and guides data collection and interpretation, which enriches the quality of the data and ensures the right questions are being asked.
My Health Coach is a just-in-time adaptive intervention (JITAI) for adults with FASD. JITAIs aim to provide the right type and amount of support when the user is most receptive. 28 Receptivity to a given intervention varies by intrinsic (e.g. age, personality characteristics) and contextual (e.g. time of delivery, location, and activity of the person) factors. 29 Tailoring delivery of the intervention to times when a person is most ready to receive it increases engagement and reduces intervention fatigue. 28
My Health Coach is informed by self-determination theory (SDT). SDT highlights the importance of autonomy, competence, and relatedness for an individual's well-being and health. 30 According to SDT, all people have a need to regulate their own experiences, feel able to do things well, and feel socially connected. 31 The degree to which any of these psychological needs are unsupported or thwarted will have a detrimental impact on wellness in that setting. In accordance with the three core psychological needs of SDT, the My Health Coach app aims to help adults with FASD feel more competent, in control, and connected with others.
Following a user-centered design approach, 32 the UR research team and ALC discussed initial design ideas, and an initial design prototype was created in Adobe XD 33 (see Figure 1). Consistent with findings from prior research on mHealth features for people with developmental disabilities,34,35 the prototype was designed to feel familiar and easy to navigate for adults with FASD. After installing the app, users will be able to select and customize their “health coach,” which will be a chatbot they interact with via text or voice messages. Prior mHealth studies using chatbot-driven interventions have evidenced health benefits including reduced psychological stress and promotion of positive health behaviors.24,36 The health coach interface will resemble using a typical messaging app, which is familiar to most adults with developmental disabilities. 26 Interaction can be initiated by the health coach chatbot or the user. By default, the health coach chatbot will initiate a brief “daily check-in” with the user each day (one JITAI decision point used in My Health Coach). This will provide active assessment for tailoring variables, which will determine whether specific intervention options will be deployed. The initial design prototype capitalizes on well-established techniques to promote behavior change when the user is receptive. For example, these techniques may include brief psychoeducation, goal setting, consideration of an alternate reframed interpretation, activity scheduling, and ideas for relaxation and stress reduction, among others. Several specific tools and features to support these techniques can be seen in Figure 1.

My Health Coach app prototype. From left to right: avatar customization, daily check-in, tracker tool, an daily messages.
The current study
The current study represents a critical foundational step of our user-centered design approach. Gathering community member input early and iteratively throughout the development process helps to facilitate the acceptability and utility of the app.27,37 After development of the prototype, we conducted focus groups and surveys to elicit broader feedback from adults with FASD. Our aims for these focus groups and surveys were: solicitate in-depth qualitative feedback on app prototype and recommendations for additional features and ascertain broader quantitative input on key features and themes raised during focus groups, respectively.
Methods
Study design
Qualitative methods are widely accepted as an integral component of the development process of mHealth apps. 27 The current study utilized QUAL + quan sequential mixed methods design. 38 Mixed methods purposes were triangulation, complementarity, development, and initiation. The methodological orientation underpinning this study was content analysis. The qualitative phase of the current study included focus group methods to gather key input from adults with FASD, eliciting in-depth feedback about the design and proposed components of the My Health Coach app. Following review of focus group data, the development team and the ALC developed a survey to gain additional input on key themes and ideas raised during focus groups. The interactive design prototype was shown to focus group and survey participants to help inform refinements to the design and functionalities to the app prior to programming.
Inclusion and exclusion criteria
To be eligible for the study, participants needed to be an adult (18+) with known PAE or diagnosis of FASD (self-report), and have conversational fluency in English. Participation in a focus group was dependent upon eligibility, complete responses to the demographic surveys, and scheduling availability for the planned focus groups. Participation in the follow-up survey was dependent upon eligibility, complete responses to the demographic surveys, and complete responses to the study survey. Those who indicated they were younger than 18-years old, did not have known PAE or an FASD diagnosis, were unable to attend a scheduled focus group or had missing or incomplete survey responses were excluded from the study.
Recruitment
As the app is intended for adults with FASD worldwide, perspectives were elicited from participants in various countries. Adults for both the focus groups and follow-up survey were recruited by leveraging various networks of the UR research team and ALC. Study advertisements were posted to UR research team members and ALC's social media accounts. Recruitment materials were also shared with team members’ networks and other known FASD organizations, who distributed them among their contacts via email, social media, newsletters, or in-person. In general, authors did not have prior existing relationships with participants, however, some ALC members did know a few specific participants through interactions in other settings (e.g. online support forums).
Interested adults were directed to the study's Consent and Screening Module link on REDCap, hosted at the UR.39,40 All participants reviewed the Study Information Sheet, including members of the ALC, to understand the risks and benefits of participating in the study. They also answered questions about the Study Information Sheet to ensure understanding and were given the opportunity to contact study staff with questions. Participants then provided consent. A “Notification of Collection and Use of Personal Data” was also included in the REDCap Screening Modules immediately after the Study Information Sheet to inform all participants from the European Union or the United Kingdom about compliance with General Data Protection Regulation requirements. Written permission was obtained for any participants who had a legal guardian. For those adults who indicated they had a legal guardian, the research team contacted the person to review the permission form and obtain the needed signature through REDCap's eConsent functionalities.
Procedures
Focus groups
The data collection team included six ALC members, a doctoral-level researcher with 20 years of experience with FASD (second author), a project coordinator with 4 years of experience with FASD, two full-time research assistants with 2 years of experience with FASD (first and tenth authors), and an undergraduate research assistant. The majority of the data collection team identified as female, with one member identifying as male. Focus groups were co-led by members of the ALC (fourth, fifth, sixth, seventh, eighth, and nineth authors) and a research team member. Co-leadership by ALC members was crucial, given the project's emphasis on self-advocacy, strengths, and empowerment of adults with FASD. Research team members managed the audio recorder, took notes during discussions, addressed logistical concerns or questions, and helped keep the discussion on topic.
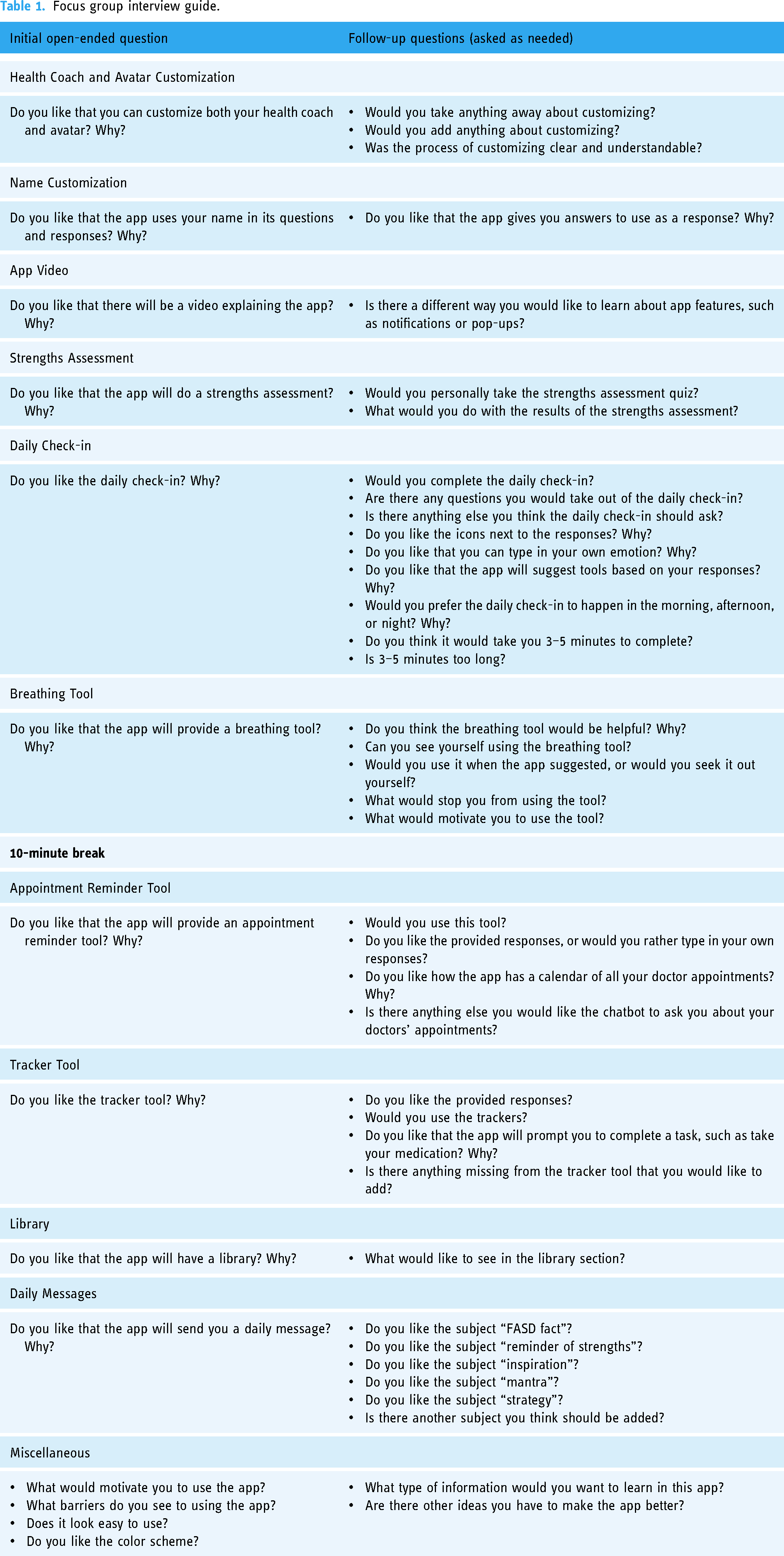
Focus groups were conducted online using a HIPAA-compliant Zoom platform. Seven focus groups were conducted in total and lasted about 90 minutes on average. Each focus group session began with an introduction from the study's principal investigator (second author), a statement about the purpose of the focus group, and a list of group rules and expectations. Participants were explicitly encouraged to share concerns or negative feedback during focus groups to reduce positive response bias. If there were more than four participants present, participants were evenly divided and sent into Zoom breakout rooms to allow for maximum participation. Each breakout room had at least one ALC member and one research staff. Next, the research team showed participants the interactive initial app design prototype using Adobe XD. 33 Following a semi-structured interview guide (see Table 1), ALC members elicited participant discussion feature by feature. The interview guide was co-developed by the ALC and the research team, with careful attention to language. Requests for additional targets for future app development were also solicited. The first author transcribed focus group recordings verbatim which were checked for accuracy by the tenth author. After the seventh focus group was conducted, the team discussed data saturation and decided sufficient input had been gathered through this method.
Focus group interview guide.
Follow-up survey
After completion of the focus groups and initial data analysis, a survey was developed to solicit additional feedback and allow another avenue for participants to give feedback. The survey was administered online using REDCap.39,40 After completing a demographic survey, participants watched a short introduction video of the ALC and research team, which stated the purpose of the survey, showed the initial customization and chatbot features to help orient the participant to the app, and asked participants to continue with the survey to provide feedback and recommendations. Participants were then shown short video walk-throughs of the initial prototype feature by feature using Adobe XD. 33 They were asked if they liked or disliked the feature and why and given space to provide recommendations (see Supplementary materials for questioning route).
Data analysis
Focus groups
The data analysis team was overseen by the second author and qualitative analysis was conducted by the first, tenth, and eleventh authors. The group consisted of two bachelor-level full-time research assistants, with one holding a master's degree (both participated in data collection) and an undergraduate research assistant who did not participate in data collection. Before coding, all had undergone training on qualitative coding administered by the lab principal investigator (second author). Data and codes were managed using Dedoose. 41
Data were analyzed thematically to understand participants’ perspectives on the initial app design and functionalities to identify patterns or themes within the data.42,43 Consistent with the approach advocated by Miles, Huberman, and Saldana, 43 coders first familiarized themselves with the data, iteratively reviewing each transcript and independently assigning initial codes (“first-level” coding). The following a priori coding methods were selected based on similar prior studies: 32 structural, values, and evaluation coding. The team then came together and discussed, operationalized, and refined each code. Transcripts were then re-coded, and codes were refined through further discussion and consensus, as needed.
Follow-up survey
Consistent with the focus group analysis, the first, tenth, and eleventh authors examined and coded free-response sections of the survey. Free-response sections were analyzed thematically using the established codebook from the focus group data. Codes from the focus groups fit well with survey responses. There was a 15% increase in “first-level” codes to capture new ideas from survey respondents. These codes were added to capture topics that focus groups either did not cover or did not cover in-depth due to time restraints, including perceived motivations and barriers to using the app and feedback on the proposed logo.
Integrative analysis
Consistent with our approach in prior studies, 25 the coding team then generated “second-level codes,” which considered categories or deeper meaning among first-level codes of focus group and survey data. 43 During this process, coders examined interrelationships and networks among codes and built a preliminary thematic framework. Participant and group “fit” with the framework were also assessed, with confirmatory and disconfirmatory evidence for the model examined. Although additional codes were added in coding survey data, the overall structure of second-level coding did not generally differ among focus group and survey participants.
After the research team systematically coded the data from focus group and survey responses, the first (UR researcher) and ninth (ALC member) authors created a document and complementary video with preliminary analysis. This document was sent to focus group and survey participants as a member check. Member checking involves sending a summary of findings to participants to review and provide comments if they like.44,45 This gave the participants an opportunity to confirm results and/or give additional feedback via email. Participants who replied indicated results were a good fit with their experience and provided no further feedback or changes.
Lastly, following “second-level” pattern coding, a deeper analysis revealed that SDT constructs (autonomy, competency, relatedness) provided a strong organizing framework to conceptualize the data. The team then applied an SDT lens through which to analyze and interpret participants’ comments and feedback about app features and functionalities, values and beliefs pertaining to mHealth interventions for adults with FASD, and motivations and barriers to using the app. Participant and group “fit” with the constructs were assessed with confirmatory and disconfirmatory evidence for the model examined.
Results
Sample demographics
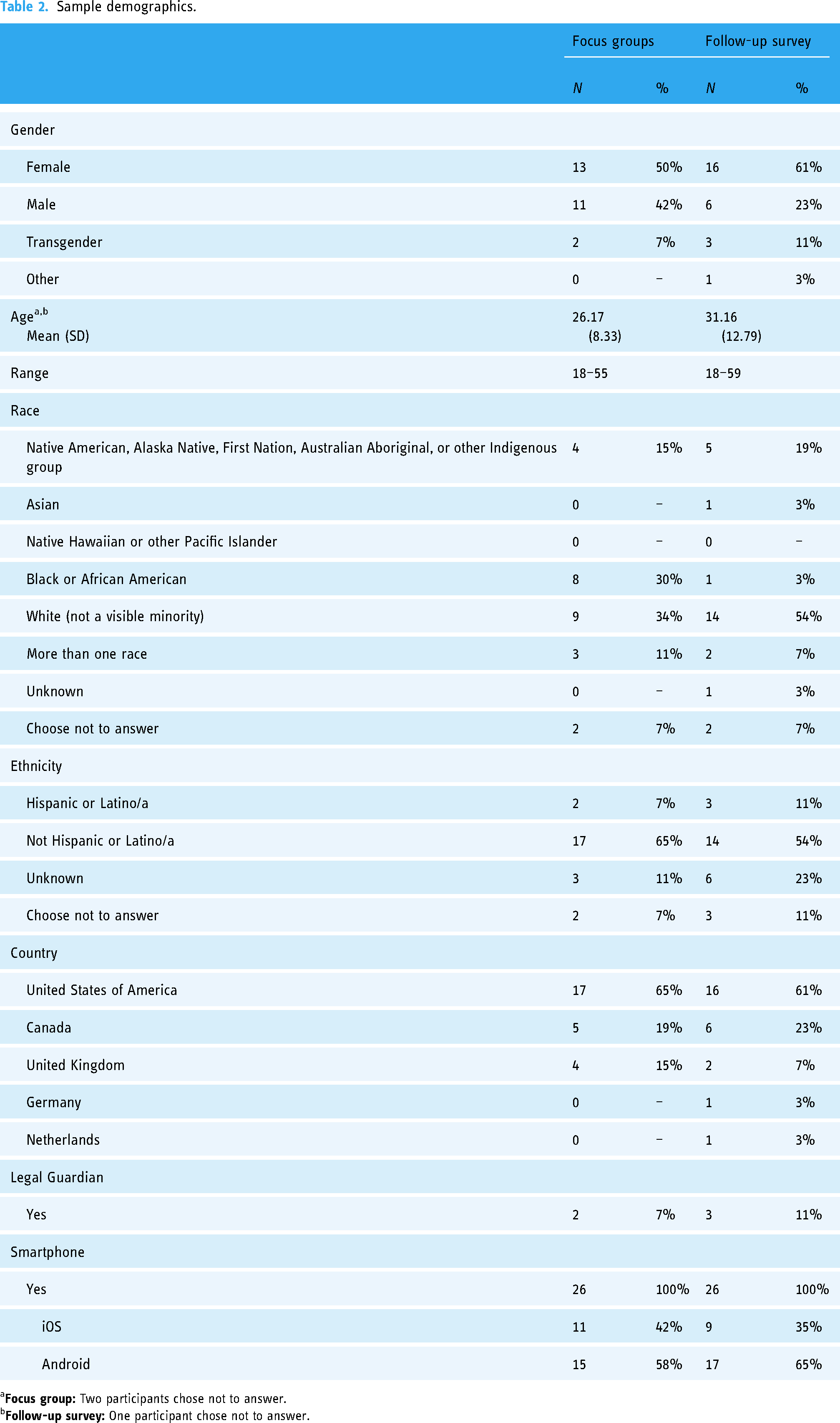
Table 2 provides the participant demographics of the focus groups and the follow-up survey. A total of 26 adults participated in one of the seven offered focus groups (FGP). A total of 26 adults completed the online follow-up survey (SP). Two participants who participated in a focus group also completed a follow-up survey. Due to the online nature of the study, we do not know how many participants decided not to participate in the study.
Sample demographics.
a
b
Global impressions
Overall, focus group and survey participants were enthusiastic about the app design. They often spoke about why they liked certain features, stating they viewed them as meeting a need they have. Participants made majority positive remarks on app features and provided very few negative valence comments about the initial design prototype (see Figures 2 and 3). Negative comments were more frequent from survey participants; comments were often due to misunderstandings or questions that were similarly raised and resolved live during focus groups.

Total positive and negative valence comments from focus groups. aN = 26. bCoded focus group responses and discussions.

Positive and negative responses and valence comments from survey. aN = 26. bResponses from “Do you like {insert feature}?” and coded free response sections.
When applying an SDT lens, participants’ responses to app features and functionalities can be categorized according to the theory's three constructs of competency, autonomy, and relatedness. Comments and feedback about the app pertained to the promotion of these constructs in users’ anticipated experience engaging with the app and perceived outcomes of using the app to meet users’ health and self-advocacy goals.
Global impressions supporting competency
Promotion of competency, or “the basic need to feel effectance and mastery” 31 was seen both with regard to users’ anticipated experience engaging with the app (i.e. the app is easy to use) and with regard to their perceived outcomes from using the app (i.e. the app will help them to effectively manage their condition).
Relating to anticipated user experience, 88% (n = 23) of survey participants answered the app looked easy to use. Participants in both focus groups and survey formats expected the app to fit a wide range of needs, allowing users along the FASD spectrum to engage with the app. They emphasized that every individual with FASD is affected differently and liked how the app provides different levels of support that the user can opt into or out of using. Participants specifically spoke about the provided responses options (i.e. yes; no; ask again later), information presented in different formats (i.e. written, pictorial, auditory), and the “stop-and-come-back” feature. For example, one participant stated: “I think it’s fairly easy to use. Not too much information but enough information to get the point across and to help you out” [FGP052].
Relating to perceived outcomes from using the app, participants were enthusiastic about the app providing supportive tools and information for condition management. Every tool shown received responses from participants about its usefulness in supporting their specific needs. Perceived competency in condition management was the most cited motivation for app use among both focus group and survey participants. For example, I like the appointment tracker because I think it is a really fantastic and useful tool for those people…with fetal alcohol spectrum disorder as we forget things due to our condition. I think it's really helpful that it can remind you of specific things dates and times…The things that would motivate me most, to use [the app] would be that I suffer with fetal alcohol syndrome myself, I also think that it would be beneficial to me as it's like your own health coach sat right in front of you but it's on a screen instead. And I think it's a really fabulous idea [SP033].
Global impressions supporting autonomy
Promotion of autonomy, or “the need to self-regulate one's experiences and actions”, 31 was seen with anticipated user experience engaging with the app (i.e. customization options) and perceived outcomes from using the app (i.e. accurately recording information through provided choices)
Relating to anticipated user experience, many participants were enthusiastic about the personalization features within the app. Participants were positive about the ability to customize their health coach, personal avatar, name, and notification amounts and types (i.e. vibration, noises, text, etc.). They stated the personalization choices made them feel “like [they] own the app” [FGP057], and “at home with [the app]” [FGP056], among others. Personalization options were stated as a key motivation for app engagement.
Relating to perceived outcomes from using the app, participants were enthusiastic about the choices in the provided response options. Not only did they say it made the app seem easy to use (as stated above), but they also liked how they had many different options to choose from to accurately record things such as mood, physical health symptoms, sleep, etc. Additionally, participants also liked that they were able to add their own response if desired: “So, that choice, that option, of typing in what I’m feeling is very useful—I like it” [FGP059].
Global impressions supporting relatedness
Lastly, the promotion of relatedness, or “feeling socially connected,” or a sense of “belonging” 31 was seen with anticipated user experience engaging with the app (i.e. reduce isolation) and perceived outcomes from using the app (providing self-advocacy tools).
Relating to anticipated user experience, participants noted that the app would reduce the feeling of isolation via the chatbot. For example, in one focus group, participants conversed: “Exactly yeah, you feel like you’re actually talking to someone and someone’s actually there to be like, ‘hey how are you this morning?’” [FGP041] “Like they actually care, and they actually want to listen” [FGP030]. Others also felt the chatbot would be a part of their support network: “I think it’s going to be good for a lot of people with disabilities as well because they have that person there and they’re able to offload and tell them anything and they won’t judge you, they won’t be nasty to you, they’re there for you” [FGP045].
Relating to perceived outcomes from using the app, participants were enthusiastic about the self-advocacy tools the app provided, stating they would aid in better connection with their support networks. For example, “The research sources may help to improve your credibility which is something I always seem to lack when talking to physicians” [SP005].
Individual components
Participants’ responses to individual components were positive across both focus groups and the survey (see Table 3) and showcased how the app promoted competency, autonomy, and relatedness. Participants also provided recommendations for app features and future directions.
Recommendations for app features and future capabilities.

Avatar and name customization
Focus group participants were overall positive about the avatar and name customization feature. Both perceived promotion of autonomy and relatedness were present in participants’ responses, emphasizing the personalization opportunities and choices in creating a name and avatar would make them feel comfortable when using the app. Participants also noted that personalization options such as these were a motivation to use the app: “I like [customizing the avatar because] it makes it your own. And it's not just some random avatar that the app picks; you can actually make it your own style and to fit your personality” [FGP009].
While overall acceptable to participants, there were concerns the customization options would be too overwhelming for some people with FASD. One participant recommended having a pre-made avatar option to meet this need. Others recommended adding more customization options, including clothing, hats, eye color, and skin color as pictures (instead of words) to be more inclusive. Lastly, participants wanted the opportunity to name their health coach. There were no negative comments or recommendations about the name customization. Survey participants were not asked about the avatar or name customization features, but one survey participant used the free-response section to say they liked the avatar customization feature.
App video
Participants overall were positive about the app orientation video, stating the video was “great” [FGP057], “a really good idea” [FGP053], and the video “makes the app very user friendly” [FGP058]. Discussions and recommendations showcased perceived promotion of competency through the app being easy to use and meeting a wide range of needs. Participants also liked the use of visuals.
When asked how long they thought the video should be, responses varied; participants suggested 5–10-second demonstrations or anywhere from 30 seconds to 3 minutes in length. All respondents emphasized the need for the video to be short and engaging.
Recommendations for the video included adding captions to the video, as well as providing written instructions, overlays, a demonstration feature, and a “frequently asked questions” page or picture guide. Survey participants were not asked about the app orientation video and no comments were made in the free response sections.
Daily check-in through chatbot
Participants were very enthusiastic about the daily check-in, which garnered the most positive valence across focus groups. Among survey responses, 92% (n = 24) of participants stated they liked the daily check-in. Representative quotes across data collection formats include: “I love it” [FGP044], “[the] daily check-in is awesome” [FGP057], “it will be helpful to start the day” [SP049], and “I like it because it makes you do a body check” [SP024]. Perceived promotion of all three SDT constructs were seen in the participants’ responses to the daily check-in feature.
Relating to competency, participants thought the daily check-in looked easy to use, and liked how it took place in the chatbot. Participants also noted they liked how the app would send prompts to complete the check-in. Next, participants also stated the daily check-in was a supportive tool for condition management. Many liked how the check-in will record and remember answers to which users could reference, for example a survey participant stated in responses to “Why do you like the daily check-in?”: “It will keep track of things for me” [SP039]. They were also enthusiastic about the app recommending other tools based on the user's responses. Participants stated the daily check-in was a tool to help meet their needs. Additionally, participants mentioned they liked the daily check-in's positive activity question: “I loved that it seemed to remember the things that you did…the day before, like to spark that positivity of like you had that awesome thing happen, what are you going to do today? And I love that. I love that so much” [FGP041].
Relating to autonomy, participants stated they liked that the daily check-in not only provided responses to each question in text and picture format but also that there was an option to add their own responses as well, for example, “Being able to, yeah, write out your own responses, compared to just having specific things picked for you, once again, it's personalization like I love, love that aspect of this” [FGP041].
Lastly, regarding relatedness, participants spoke to how the daily check-in would reduce isolation, as it felt like texting with a real person. They also noted it could be used as a tool to help better connect with their support networks by using the recorded answers.
There was only one negative evaluation of the daily check-in, which focused on the ability of the user to add their own response to a question. The participant thought this option may be overwhelming for some users and suggested it be removed.
There were numerous recommendations for the daily check-in. Many of these recommendations pertained to the app's time estimate for how long it would take a user to complete the daily check-in, with some suggesting the time estimate was inaccurate or not necessary. Participants also suggested that users be able to customize when and the number of prompts the user receives to complete the daily check-in. Other recommendations included being able to edit or add to responses throughout the day or being able to pick more than one provided response to each question. Additionally, participants recommended having an overview page of answers or an end-of-the-day recap. Participants also wanted more in-depth responses to answers, such as advice or suggesting tools within the app. Lastly, another participant suggested design changes such as different colors or having more fun or engaging responses such as gifs or pictures.
Daily messages
Participants were overall enthusiastic about the daily message feature, which were once-a-day pop-up notifications. Among survey participants, 88% (n = 23) said they liked the daily message feature. Participants across data collection formats especially liked the messages that were positive affirmations and FASD facts. They felt the daily messages would promote competency as they would include reminders to use the app. This would help with memory challenges.
There were two negative evaluations centered around “the nuisance of receiving messages every day” [FGP059]. Some concerns were raised about discretion, as some participants did not want the daily message notifications to mention FASD in case someone saw their phone's locked home screen (where the messages would appear).
The most common recommendations were having access to past messages, the ability to customize the topic and number of daily messages received and including messages about new FASD research and news.
Tools and assessments
Participants were asked about the tools and assessments available in the app, including the strengths assessment, breathing tool, appointment reminder tool, and tracker tool. Both focus group and survey participants were generally positive and enthusiastic about these tools. Specific evaluations and recommendations are below.
Strengths assessment
Participants spoke about how the strengths assessment would promote competency and relatedness, as they felt it would provide information about themselves and could be used as a self-advocacy tool to help better connect with others. For example, “I think it's a very good idea because some people, well, or myself, don’t know my strengths. And if the ask[ed] me then I’ll know. So, it's good that they have the questions” [FGP038].
Negative feedback on the strengths assessment centered around the volume of questions, with concerns about it being too overwhelming. Recommendations for this feature were to assess for weaknesses as well as strengths. Survey participants were not asked about the strength's assessment and no comments were made in the free response sections.
Breathing tool
Both focus group and survey participants felt the breathing tool would promote competency with their condition management. Among survey participants, 81% (n = 21) stated they liked the breathing tool. Specifically, participants liked that the feature was supportive, relaxing/destressing, and would aid in improving their mental health. For example, “I could always use help breathing. It looks pretty, which will also help calm me” [SP010]. Participants were enthusiastic about the app recommending the breathing tool based on daily check-in responses.
The majority of negative feedback centered around not liking the tool due to personal preference and the frequency of prompts to use the tool.
There were many recommendations for the breathing tool, such as adding music, meditation or mindfulness features, guided breathing exercises rather than just an image, videos, and an LED light component. Participants noted the ability to choose what types of grounding or relaxation tools offered was important, touching on autonomy for the users and meeting different needs.
Appointment reminder tool
Focus group and survey participants felt this tool would increase competency in condition management as it would help them to remember their appointments and promote autonomy through the ability to personalize the tool. Among survey participants, 92% (n = 24) answered they liked the appointment reminder tool. For example, one focus group participant stated: Because I’m a forgetter. I always forget. Someone has to remind me. Like the day of, they’ll be like you have an appointment and I’m shocked I’m like I never knew this, no one ever told me. So basically, it’ll be very helpful to get a notification and let me know because I forget all the time [FGP038].
Recommendations for this feature included the ability to ask for location and link to Google Maps, reminders of what to bring to the appointment, a color-coded calendar for different appointment types, the ability to add appointments manually, confirmation messages, personalization of the number of reminders sent for each appointment, and a pre-check-in before the appointment.
Tracker tool
Participants felt this tool would promote their competency in memory and other challenges, as well as their autonomy in being able to personalize this tool. Among survey participants 96% (n = 25) answered they liked the tracker tool. Participants across both data collection formats liked that the app would have premade trackers, such as a medication tracker, as well as the ability to customize new trackers. For example, Especially when I saw, like, the eating reminder thing, I’m like yes, I have a major problem with that. My brain somehow just can’t link to my gut half the time throughout the day. So, I literally don’t even feel hungry and it's so bad, you know, the time will pass by and by like 7 o’clock I’m like, I didn’t eat anything today. It's really bad…I definitely like that feature, for sure, with the access of tracking stuff and like reminders [FGP012].
Recommendations for the tracker tool included specifying which medication was taken on an overview page and the ability to backlog medications that were taken but not logged. They also suggested the ability to log a task as complete manually rather than just through the chatbot, and an overview page of all trackers. Participants also recommended different types of premade trackers that the app could offer, including a checklist option, walking, mileage for driving, birthdays, menstruation, paying bills, water intake, walking the dog, expenses, drug use, calorie intake, self-time, brushing teeth, and budgeting for medications.
Library
Focus group and survey participants were overall enthusiastic about the library feature, stating perceived promotion of competency by providing information about FASD, and autonomy and relatedness by providing self-advocacy tools to help better connect with their support network. Among survey participants, 92% (n = 24) stated they liked the library feature. They noted it would meet the need for evidence-based information about their condition for themselves and for others. For example, I’m actually weeping while I listened to the video. It's a big deal to have access to information and tools to help me educate my doctors. It's been so frustrating (gaslighting, really) to not have the medical community understand the holistic impact of FASD. THANK YOU!! [SP010]
Recommendations for the library included ways to share PDFs, such as through messaging apps such as WhatsApp, and factsheets geared toward other groups such as law enforcement. Participants also recommended different factsheet topics such as information about healthy foods and medication. They also recommended the app have motivational videos. Lastly, others suggested having a factsheet with the user's daily check-in responses to give to their healthcare providers.
Logo
Participants in the follow-up survey were asked about the logo: 77% (n = 20) of participants indicated they liked the logo. In the free-response section, participants noted that the logo was simple, inclusive, and colorful. They also stated the logo seemed supportive of people with FASD. Six participants stated they did not like the logo, noting it was generic and wanted it to center more around FASD, and felt it should include more colors.
Potential barriers to app use
One common barrier reported was the app sending too many notifications. Participants also identified the app may be overwhelming for some people with FASD, specifically the amount of text and the number of choices and free response sections. Others thought the app may be too time-consuming or they may forget to use it. For example, “It might work but it would just take a lot of work for me to get used to it and everything” [FGP052].
Motivations for app use
The most mentioned motivator was the customization aspect of the app and the number of choices the app provided. For example, If you get to choose your own thing that makes it a little more fun. You know? More like not just, okay this is another thing trying to help me whoop-di-do, it's like oh, I get to create my own thing and it's more exciting and more engaging and maybe make people want to use it more [FGP009].
Additional recommendations
Participants in focus groups and surveys gave in-depth recommendations for app features and future capabilities. These recommendations are organized into four categories: accessibility, accountability, expanding app features, and app design. These recommendations are summarized in Table 3.
Discussion
Consistent with our user-centered design approach, 32 the purpose of this study was to gather community member input to inform the design and development of an mHealth app for adults with FASD. This project is a partnership between the University of Rochester and identified leaders in the FASD community, known as the International Adult Leadership Collaborative (ALC). Focus group and survey results from adults with FASD documented high acceptability of the initial design and proposed functionalities of the My Health Coach app. Participants thought the app would be helpful and beneficial to their health and self-advocacy goals. Data analyses found participants perceived the app to meet important needs that align well with the three basic psychological needs posited by SDT (competency, autonomy, relatedness), which is consistent with the theoretical framework informing app development. Several valuable recommendations for additional features were offered to guide subsequent development of the My Health Coach app.
FASD affect the health and development of people across the lifespan; 3 however, there are minimal services and support for adults with FASD. 46 The current project aims to meet this need in a systematic way. A scoping review by Quan et al. (2019) identified six themes that should be considered when creating community-based interventions for adults with FASD. These themes include functional context, individualized support, education for service providers, structure and routine, utilizing a strengths-based approach, and environmental adaptations. 46 Participants in the current study emphasized many of these same themes in their evaluation of the My Health Coach app. For example, participants felt the app will provide users with functional context. This functional context aids with life skills, such as condition and stress management, as well as accessing healthcare. Participants stated the app will also provide individualized and FASD-informed support. The app is being designed by a team who has a strong understanding of FASD (a clinical psychologist with 20 years’ experience and the ALC who has living experience). The app will provide structure and routine for the users, as they will be prompted to complete tasks at the same time each day. Furthermore, the app will be strengths-based, not only with a strengths assessment but also as the ALC developed and ensured all features and language to be strengths-based. Lastly, environmental adaptations, such as the use of visuals and provided responses, were taken into consideration while creating this app. The format will look familiar for users who have used smartphones and is being created to be easy to navigate.
As is documented in quantitative studies, many adults with FASD face challenges with attention, learning and memory, planning, task efficiency, and analyzing social situations. 3 Participants’ responses to app features and functionalities mentioned the above difficulties as challenges they face in their everyday lives. In doing so, they stated the app could help mitigate or provide support to meet these challenges. Memory specifically was mentioned in all focus groups and in many survey responses as a challenge that the app will help with by providing prompts and reminders, as well as recording different information inputted by users.
Increasingly, technology is being harnessed to support or deliver interventions for physical and mental health problems across the lifespan. 20 Unfortunately, very few mHealth apps undergo any type of rigorous evaluation. A recent meta-analysis completed by Yang et al. (2019) identified 64 studies that evaluated mHealth interventions targeting five main topics including mental health, nutrition and weight status, physical activity, health-related quality of life and well-being, and chronic disease management. Furthermore, very few studies have examined the efficacy of mHealth interventions for people with developmental disabilities, despite the high prevalence of co-occurring conditions in these populations. 47 Recent studies have shown that people with developmental disabilities have similar rates of smartphone ownership and usage as in the general population. 26 Of the 64 mHealth interventions analyzed by Yang et al. (2019), none focused on people with developmental disabilities. The few published studies testing mHealth interventions for people with developmental disabilities either did not meet the rigorous design requirements (randomized control trial; RCT) for the meta-analysis or have been published subsequently. The most well-studied mHealth intervention for people with disabilities is the “interactive mobile health and rehabilitation (iMHere)” app, which was first tested with adults with spina bifida and spinal cord injuries. Results from two small trials documented improved self-management abilities across participants.48,49 This mHealth intervention has been subsequently adapted and expanded to be more broadly appropriate for people with chronic conditions and disabilities. Initial usability and feasibility tests suggested promise and larger tests are under way. 50 These findings suggest promise for future development of mHealth apps for people with developmental disabilities.
Strengths
There are several important strengths of this study. First, partnering with identified community leaders helped determine relevant app functionalities and design features, ensured the questions asked were understandable and strengths-based, and reduced stigma. Co-conducting research with the ALC also enriched the quality of the data collected and increased comfort for our participants. Another strength was the gathering of feedback in multiple formats. By offering participants the opportunity to respond live in focus groups, or more privately in the survey or by email, phone, or private Zoom call during member checking, we broadened accessibility to people along the FASD spectrum. Furthermore, the participant pool was quite diverse. This study gathered input from participants from five countries. Diverse races, ethnicities, and genders were represented (see Table 2). Users with both Android and iOS operating systems participated. Lastly, our development process for the app is a systematic approach that builds on prior experience developing apps for caregivers raising children with FASD.25,32 The current study represents the early and iterative gathering of key community member feedback to inform the development and evaluation process, design of the content, and user interface. Focus group and survey data also facilitated acceptability and utility of the intervention. Building on previous work on the benefits of community-engaged research, involving key community members enhances developers’ understanding of the needs and challenges of adults with FASD and practical strategies to help mitigate them. 51
Limitations
Limitations of our study included data collection methods for the follow-up survey. Feedback from a few participants suggested that the consent documents may have been a barrier due to the amount of text that was necessary to read. In future studies, we plan to include video versions for participants who prefer audio and visual formats opposed to text. Furthermore, while there were efforts made to increase comfort and accessibility to people across the fetal alcohol spectrum (such as working with the advisory board and offering multiple feedback channels), this study is likely missing voices that either were not comfortable with these channels, had scheduling problems, or needed different supports to participate. This was especially salient with the Consent and Screening forms for the study.
Next steps and implications for future research
Consistent with our systematic user-centered design approach, we will use these findings to inform development of an initial app prototype. We will then conduct an initial feasibility pilot study to assess the feasibility and acceptability of the app with users to inform a larger-scale RCT. For example, this feasibility trial will test using video format for consent documents, determining appropriate literacy level for measure items, and understanding ease of installation of the app for adults with FASD. Establishing feasibility on a smaller scale increases likelihood of a successful RCT.
This study has the potential for a significant public health impact in multiple fields. There are limited resources and interventions for adults with FASD. The My Health Coach app has great potential to be a scalable and evidence-based solution to this need. Additionally, relatively few mHealth apps have undergone rigorous evaluation, 52 with even fewer made and tested for people with developmental disabilities. 47
Conclusions
Through focus group and survey methods, our study found the proposed mHealth intervention to be highly acceptable to adults with FASD. Participants made a vast majority of positive valence comments about the proposed features and gave constructive feedback with suggestions on how to continue to refine and improve the app. Participants’ comments aligned with SDT, shown through comments about how the app could help them feel more competent, in control, and connected with others. This project is one of the only studies in the field of mHealth interventions to undergo rigorous evaluation, and to have been made and tested for people with developmental disabilities. Findings from this study may inform app development for other related disabilities and conditions. This project also showcases the value and necessity of partnering with community members throughout the development process.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241261458 - Supplemental material for My Health Coach: Community members’ perspectives on a mobile health tool for adults with fetal alcohol spectrum disorders
Supplemental material, sj-docx-1-dhj-10.1177_20552076241261458 for My Health Coach: Community members’ perspectives on a mobile health tool for adults with fetal alcohol spectrum disorders by Emily L Speybroeck, Christie Petrenko, Cristiano Tapparello, Katrina Griffin, Emily Hargrove, Myles Himmelreich, Anique Lutke, CJ Lutke, Maggie May, Shuo Zhang, Janna Looney and Carson Kautz-Turnbull, Madeline N Rockhold in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241261458 - Supplemental material for My Health Coach: Community members’ perspectives on a mobile health tool for adults with fetal alcohol spectrum disorders
Supplemental material, sj-docx-2-dhj-10.1177_20552076241261458 for My Health Coach: Community members’ perspectives on a mobile health tool for adults with fetal alcohol spectrum disorders by Emily L Speybroeck, Christie Petrenko, Cristiano Tapparello, Katrina Griffin, Emily Hargrove, Myles Himmelreich, Anique Lutke, CJ Lutke, Maggie May, Shuo Zhang, Janna Looney and Carson Kautz-Turnbull, Madeline N Rockhold in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Alicia Roth and Brittany Grund who assisted with the focus groups and additional staff at Mt. Hope Family Center for their support throughout the project. They would also like to thank Jan Lutke for her support of the ALC members. The authors appreciate all the participants and their support networks who made time in their busy schedules to participate in this study. This research would not have been possible without their valuable insights.
Contributorship
All authors contributed to the preparation of this study. CLMP conceived of the study, oversaw the study team, led app content development, obtained necessary approvals, and manuscript revision. ES was involved in content development, created interactive prototype, implemented the study, led recruitment, scheduling, focus group structuring, survey logistics, co-led focus groups, and led coding team, analysis team, and manuscript preparation and revision. CT was involved in the conception of the study, content development, led technological development, and manuscript revision. ALC members (KG, EH, MH, AL, CL, MM) were involved in content development, co-led focus groups, co-developed survey, and manuscript revision. SZ co-led focus groups and was involved in coding and analysis team and manuscript preparation and revision. JL was involved in coding and analysis team and manuscript preparation and revision. CKT and MR were involved in analysis and manuscript revision. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All study procedures were approved by the University Institutional Review Board (Focus Group: STUDY00004616, Survey: STUDY00007156)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute of Health under Award #UH2AA029050. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health. This work was done in conjunction with the Collaborative Initiative on Fetal Alcohol Spectrum Disorders (CIFASD, https://doi.org/10.5967/ntw9-h991), which is funded from the National Institute on Alcohol Abuse and Alcoholism (NIAAA). Additional information about CIFASD, including information describing available data, can be found on ![]() . We also appreciate the help from FASD United. The authors appreciate the CIFASD contributors who assisted in recruitment, as well as FASD United.
. We also appreciate the help from FASD United. The authors appreciate the CIFASD contributors who assisted in recruitment, as well as FASD United.
Guarantor
CLMP.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.