
Abstract
In 2011, the Dutch government reimbursed smoking cessation pharmacotherapy with behavioral therapy for quitting smokers. We investigate whether inequalities in the use of pharmacotherapy change and, if not, whether this is due to a relatively positive injunctive norm in lower socioeconomic status (SES) groups. A total of 75,415 participants aged ≥15 years from the Dutch Continuous Survey of Smoking Habits, 2009–2012, were considered with the following measures: SES (education/income), injunctive norm (mostly acceptable/neutral/mostly unacceptable), period (2011/all other years), and pharmacotherapy use (yes/no). The proportion of low SES smokers compared with high SES smokers making quit attempts with pharmacotherapy did not differ significantly. The injunctive norm of low SES smokers differed significantly from high SES smokers and nonsmokers of all SES levels. Low income smokers with mostly acceptable injunctive norms were significantly less likely to make quit attempts using pharmacotherapy than those with a neutral or less accepting injunctive norm. The significantly lower use of pharmacotherapy in quit attempts in low income smokers with a positive injunctive norm toward smoking may partly underlie the lack of uptake of reimbursed pharmacotherapy in low SES smokers.
Introduction
Smoking is a major contributor to inequalities in health in Western Europe, with people of low socioeconomic status (SES) being more likely to smoke. 1 Inequalities are also seen in making quit attempts2,3 and successfully quitting.4,5 Quit attempts are more successful if proven effective methods are used, 6 one of which is smoking cessation behavioral therapy in combination with pharmacotherapy. 7 In 2011, reimbursed pharmacotherapy, in combination with behavioral therapy, was introduced in the Netherlands as a part of the basic health insurance package. Prior to this, pharmacotherapy was available over the counter (eg, nicotine replacement therapy) or by prescription (eg, bupropion) and was reimbursed in some supplementary health insurance packages. At the start of 2011, the Dutch government introduced this reimbursement of pharmacotherapy, which included nicotine replacement therapy, varenicline (Champix/Chantix), bupropion (Zyban), and nortriptyline. At the end of 2011, after one year, reimbursement was removed with a reversion to the situation prior to 2011. Behavioral therapy was available in the basic health insurance package during the whole study.
There were early indications that this reimbursement policy had been successful in increasing the number of smokers who attempted to quit smoking using pharmacotherapy. The number of prescriptions written by general practitioners and the number of dispensed prescriptions of pharmacotherapy were higher in 2011 than those prior to the subsidy or than those in 2012 after the reimbursement was removed. 8 This positive trend was confirmed by Nagelhout et al., (2014) in a longitudinal study. They found that the implementation of the reimbursement policy was followed by an increase in smoking cessation. They also found, however, that the use of reimbursed pharmaceuticals had not decreased socioeconomic inequalities in quitting smoking. 9 In other words, in that study, smokers in lower socioeconomic groups were not more likely to quit smoking after the introduction of reimbursement than smokers in higher socioeconomic groups.
The fact that the introduction of a reimbursement policy was not followed by decreasing inequalities in quitting smoking seems counterintuitive. As the cost of pharmacotherapy may hinder its uptake in lower socioeconomic groups in particular, 10 it seems reasonable to expect that reimbursement policies promote quit attempts using pharmacotherapy in lower socioeconomic groups 11 and that this might occur more than in higher socioeconomic groups, where price would have been less of a barrier prior to reimbursement. If reasonable, why has the study of Nagelhout et al., (2014) not shown decreasing inequalities in smoking? In this article, we hypothesize that there might also be other barriers for smokers in lower socio-economic groups, which are not removed by reimbursement policies. We specifically focus on social norms. Social norms theory suggests that prevailing social norms may influence the actions of individuals with regard to behaviors, such as alcohol consumption and smoking. 12 Perceptions of what others do can be more influential on the behavior of an individual than the real behavior of others. In the case of smoking, the social norms toward the desirability of quitting smoking might influence the actual chance of quitting.13,14 Lower and higher socioeconomic groups may differ in these norms. 13 More specifically, we hypothesize that the fact that the reimbursement policy in the Dutch case did not particularly promote quitting smoking in lower socioeconomic groups might be due to differences in injunctive norm (whether the smoker considers smoking to be an acceptable behavior in society) between socioeconomic groups.
For example, it has been suggested in a Norwegian study that more positive attitudes toward smoking may account for lower quit rates among smokers of low SES.
15
In this study, we specifically focus on a certain type of social norms, namely injunctive norms. Injunctive norms indicate whether the smoker considers smoking to be an acceptable behavior in society. Van den Putte et al., (2005)
16
found that implicit social influence variables, such as
We examine the effects of the change in the reimbursement of smoking cessation pharmacotherapy in 2011 in the Netherlands on inequalities in quit attempts using pharmacotherapy with repeated cross-sectional data. In line with the previous study of Nagelhout et al., (2014) we do not expect to find a decrease in inequalities in quit attempts using pharmacotherapy after the provision of reimbursed pharmacotherapy. In other words, we do expect the percentage of people that quit smoking using pharmacotherapy
Methods
Design
We used data from the Dutch Continuous Survey of Smoking Habits (DCSSH), which takes continuous cross-sectional web surveys of smoking behaviors of the Dutch population aged 15 years and above. Approximately 300 unique individuals are surveyed weekly with response rates ranging between 67.5% and 70.3% per year. The data are weighted to reflect the Dutch population on the basis of respondents' gender, age, and education level and social class, the province in which they live, and their family size and region. Data from the period 2009 to 2012 were used. The Central Committee on Research Involving Human Subjects in the Netherlands requires no ethical approval for nonmedical survey research.
Measures
Quit attempt using pharmacotherapy
Smoking status was determined by the question: “Do you (sometimes) smoke or not at all?” The possible answers were as follows:
A quit attempt using pharmacotherapy was determined by the question: “You see here a number of aids and methods that you can use to help with stopping smoking. Did you, the last time that you stopped smoking (or, for those still smoking, ‘in your recent quit attempt’), use one of these aids or methods?” (Multiple answers were possible.) A list of answers was given. However, the only answers used for this study were the pharmacological aids that were potentially reimbursed, which were as follows:
Smokers or former smokers who had made their most recent quit attempt using pharmacotherapy were categorized by the year in which they had made the attempt, which was one of 2009 through 2012. The question determining the year was as follows: “How long ago did you stop (was your most recent attempt to stop) smoking?” The possible answers were as follows:
Socioeconomic status
SES was determined separately by income and education
19
and split into three categories. SES by income used the gross income per year, with the middle SES cut points being €32,500–€51,300. SES by education used the following categories: low was
Injunctive norm
Injunctive norm was ascertained by participants' answer to the following question: “Which of the following statements gives the best indication of how people in the Netherlands in general think about smoking in the vicinity of others?” The possible answers were given on a five-point Likert-like scale from (1)
Period
We separated the study period into the following two time periods:
Statistical analyses
Data were weighted, as described previously in the “Methods” section. We took the group of smokers including all current smokers as well as the former smokers who had made their most recent quit attempt during the study period, which we refer to as
We then looked at the percentage of current smokers and nonsmokers (former and never smokers) with a particular injunctive norm stratified by both income and education, in each of the two time periods. Again, we compared the 95% CI of the proportions. Significance was determined by non-overlapping CIs.
We used logistic regression analyses, where the dependent variable was “a quit attempt with the use of pharmacotherapy during the study period.” The independent variables were educational level, income level, and year of quit attempt. We made a distinction between the year 2011, when the reimbursement measure had been implemented, and all other years (2009, 2010, and 2012), when the reimbursement had not been implemented. Year and educational and income levels were analyzed as categorical variables. We also reran this analysis stratified by education and income (Table 4). We considered age as a possible confounder. Gender was also considered but did not change the conclusions (results not presented here).
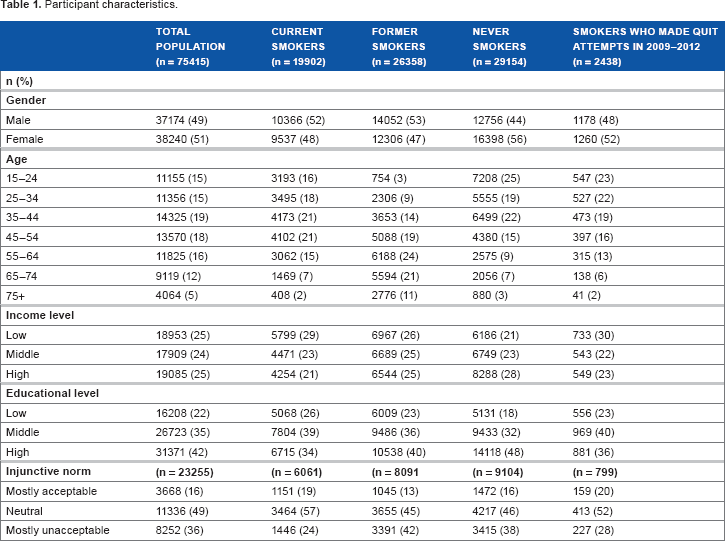
Participant characteristics.
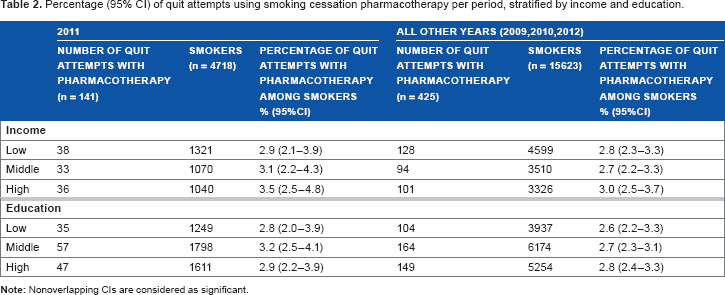
Percentage (95% CI) of quit attempts using smoking cessation pharmacotherapy per period, stratified by income and education.
Percentage (95% CI) of injunctive norm of current smokers and nonsmokers per period, stratified by income and education.

Multivariate models a showing predictors (year/injunctive norm) of quit attempts using pharmacotherapy, stratified by income and education.

All models are controlled for age.
In most variables, missing values made up a small percentage of cases. However, in the case of income level, 25% of participants lacked data. The characteristics of those missing data can be seen in Appendix 1. Most of the characteristics were similar to those in the total population with the exception that more smokers were of low educational level (4%), and, of those missing who had quit in a given year, a lower percentage were of high educational level (7%). We have treated these as missing data at random and performed complete case analyses.
Results
Participant characteristics are seen in Table 1. The characteristics of the current and former smokers are very similar to those of the smokers who made quit attempts between 2009 and 2012, with the exception that there are fewer former smokers in the younger age groups and more in the older age groups. Also, greater proportion of former smokers, never smokers, and the total population find smoking mostly unacceptable in Dutch society than is the case in current smokers or smokers making a quit attempt in 2009–2012.
There was no significant difference in the proportion of smokers of low income or education making quit attempts with pharmacotherapy in 2011 compared with all other years (Table 2). There was also no significant increase in the proportion of smokers of low SES (income and education) making quit attempts with pharmacotherapy in 2011 compared with smokers of middle or high SES in the same year.
Table 3 shows the current smokers' and nonsmokers' injunctive norm by SES level. Approximately a fifth of smokers found smoking to be mostly acceptable in Dutch society. In 2011, significantly lower proportion of low SES (income and education) smokers found smoking to be mostly unacceptable in Dutch society compared with high SES smokers. This is also the case for SES by educational level in all other years but not for income. In 2011, a significantly higher proportion of smokers of low educational level found smoking to be mostly acceptable in Dutch society compared with their peers of high educational level. No significant differences in the injunctive norms of nonsmokers were observed across periods, or income and educational levels, with the exception that in all other years there were significantly fewer high income nonsmokers who found smoking to be mostly acceptable in Dutch society than low income nonsmokers. In general, a small proportion (12%–18%) found smoking to be mostly acceptable in Dutch society, and in comparison a larger proportion (35%–47%) found it to be mostly unacceptable in Dutch society. When smokers are compared with nonsmokers, there are significantly less smokers than nonsmokers who find smoking mostly unacceptable in Dutch society in almost all income and educational levels. This pattern is more pronounced in low income and educational levels than in high income and educational levels. The only exception to this is the high income level in 2011, where a similarly high proportion of smokers found smoking mostly unacceptable in Dutch society compared with nonsmokers.
The results of the multivariate logistic regression models in Table 4 show that when injunctive norm was controlled for within each of the SES strata (in models including age), the odds ratios (ORs) for quitting smoking using pharmacotherapy in 2011 as compared to all other years increased in almost all socioeconomic groups, with the exception of those of low educational level. As expected, smokers of low income who found smoking mostly acceptable in Dutch society were significantly less likely to make a quit attempt using pharmacotherapy than those who found it mostly unacceptable [OR (95% CI): 0.29 (0.10–0.84)], regardless of year. Paradoxically, those of high income who found smoking mostly acceptable in Dutch society were more likely to make a quit attempt using pharmacotherapy [OR (95% CI): 1.95 (0.70–5.43)]; however, this was not significant.
Discussion
A similar proportion of low SES (income and education) participants compared with their middle and high SES peers made quit attempts using pharmacotherapy during the reimbursement period in 2011. This was also the case in all other years studied. The injunctive norm of low SES smokers differed considerably from that of high SES smokers in 2011. Significantly fewer smokers of low SES found smoking to be mostly unacceptable in Dutch society compared with high SES smokers. This was also the case in smokers of high educational level in all other years. Also, in 2011, a significantly larger proportion of smokers of low educational level found smoking to be mostly acceptable in Dutch society compared to their more highly educated peers. With a single exception, no differences were observed in the injunctive norm of nonsmokers across periods or SES levels. Within each SES level, approximately 40% of nonsmokers found smoking to be mostly unacceptable in Dutch society, and in general, less than half of this proportion found smoking to be mostly acceptable. Thus, a smaller proportion of smokers in low SES groups found smoking to be mostly unacceptable in Dutch society as compared to high SES smokers and nonsmokers of all SES levels.
The strength of this study is that while we have similar findings to those of another study 9 with regard to lack of change in inequalities in quit attempts using pharmacotherapy with the introduction of reimbursement, we add to this by looking at injunctive norms. These norms have not been studied frequently as an influence on quitting behavior. 16 We are not aware of any other quantitative studies examining injunctive norm in smokers of different SES levels in the context of quitting smoking.
Some limitations of this study must, however, be considered. We selected cases in such a way that we were certain in which of the four years their most recent quit attempts took place. We did not include participants interviewed in the first four weeks of the year who indicated that they had quit in the past month, because it was not possible in these cases to tell if they had quit in January of the year in which they were interviewed or in December of the previous year. This means that we lost data on January 2012 during which
It is possible that the number of smokers using pharmacotherapy in a given year were under represented because the questionnaire records the
Another possible limitation is that a quarter of participants missed income data. These participants were similar to those with income data in the total group with the exception that 4% more were of low educational level. Of those who had made a most recent quit attempt during the study period, 7% less were of high educational level. It is possible that these differences biased the results; however, our results on the differences in the use of pharmacotherapy in different income groups have also been found elsewhere, 9 and educational level exhibited the same pattern of findings.
It is possible that individuals in lower SES groups had less access to the pharmacotherapy. In 2011, the affordability of proven effective smoking cessation pharmacotherapy was addressed in part by the Dutch government. Because the Dutch government opted for
We found that the introduction of reimbursement of smoking cessation pharmacotherapy does not lead to a greater proportion of low SES smokers compared with high SES smokers using this therapy. This corresponds to the results of the previous study by Nagelhout et al., (2014), 9 which showed that inequalities in the use of smoking cessation pharmacotherapy in quit attempts were unchanged by the introduction of the reimbursement. This was not a result of the differences in the awareness of reimbursement, because, as we see from previous research, the reimbursement was widely known about. For example, a campaign was run from December 2010 to March 2011 to ensure that Dutch smokers, with emphasis on those of low educational level, were aware of the reimbursement. 21 It had the following components: television and radio slots, a campaign website, banners, use of social media, posters and flyers, and messages in newspapers and magazines. Approximately 80% of smokers with a quit intention had seen the campaign, and this was higher in those of low educational level than high educational level. 21 Approximately 60% of smokers intending to quit knew that reimbursement was available after the campaign. 21 There were also no income differences in the awareness of the reimbursement between high, middle, and low income groups in 2010–2012, and ∼40% of participants were aware of the policy in 2011. 9
Those of low income who found smoking to be mostly acceptable in Dutch society were significantly less likely to make a quit attempt using pharmacotherapy than those who found it to be mostly unacceptable. Approximately 20% of the low income group in both periods has a mostly acceptable injunctive norm, with approximately 55% having a neutral injunctive norm. Thus, while those with a mostly acceptable injunctive norm are a minority, it is possible that injunctive norm might explain the lack of uptake of the reimbursement. This could be because they might not feel much social pressure to quit (and thus to seek methods to help with quitting, such as smoking cessation pharmacotherapy) because they have enough others around them with the same accepting norm or a neutral norm. 16 Also, those with a more accepting injunctive norm might be less ready to quit. 16 The injunctive norm of low SES smokers differs significantly from that of low SES nonsmokers who feel that smoking is significantly more unacceptable. Differences in these groups in other SES levels are less pronounced. Thus, low SES smokers have an injunctive norm different from all other subgroups. This is an important finding as other smokers in a smokers' social network are highly influential. Low SES smokers tend to have more smokers in their social networks and are more likely than high SES smokers to gain smoking friends, 22 which could act to maintain injunctive norms. Smokers who lose smoking friends from their social network are more likely to intend to quit, attempt to quit, and succeed in quitting. 23
It is possible that a targeted attempt to influence those smokers in low SES groups with neutral or accepting injunctive norms to adopt unaccepting injunctive norms, prior to or concurrent with the availability of reimbursement, might result in greater use of pharmacotherapy in quit attempts in this group. Such attempts could possibly be made using mass media campaigns.
Conclusion
In the Netherlands, reimbursement of smoking cessation pharmacotherapy did not increase the proportion of low socioeconomic status smokers who attempted to quit using this therapy to a greater extent than the proportion of higher socioeconomic status smokers. A smaller proportion of low SES smokers think that smoking is generally unacceptable in the vicinity of others in Dutch society compared with smokers from high SES groups or nonsmokers of all SES levels. The significantly lower use of smoking cessation pharmacotherapy in quit attempts in low income smokers with a positive injunctive norm toward smoking, and a similar, though nonsignificant pattern, seen in low educational level smokers, might partly underlie this lack of increased uptake of reimbursed smoking cessation pharmacotherapy in low SES smokers. In order to have an equal impact over socioeconomic groups, the introduction of reimbursement should probably be accompanied by measures aimed at changing the injunctive norm toward smoking.
Authors Contributions
Conceived the idea and participated in the design of the study: FEB, VN, MCW, KS. Prepared the data: GEN. Performed the statistical analysis and drafted the article: FEB. All authors were involved in the critical revision of the article and read and approved the final article.
Footnotes
Acknowledgment
The authors would like to thank STIVORO for the use of the DCSSH database.
Appendix
Characteristics of participants’ missing data for income.
ALL (n = 19467) N (%)
SMOKERS DURING (PART OF) THE STUDY PERIOD (n = 5475) N (%)
PARTICIPANTS WHOSE MOST RECENT QUIT ATTEMPT FELL WITHIN THE STUDY PERIOD (n = 613) N (%)
2009
4577 (24)
1433 (26)
194 (32)
2010
5273 (27)
1513 (28)
152 (25)
2011
4837 (25)
1287 (24)
140 (23)
2012
4780 (25)
1242 (23)
127 (21)
Male
8666 (45)
2584 (47)
260 (42)
Female
10802 (56)
2891 (53)
353 (58)
15–24
3579 (18)
1071 (20)
165 (27)
25–34
2949 (15)
951 (17)
138 (23)
35–44
3997 (21)
1198 (22)
111 (18)
45–54
3792 (20)
1185 (22)
97 (16)
55–64
2801 (14)
726 (13)
68 (11)
65–74
1659 (9)
256 (5)
26 (4)
75+
690 (4)
87 (2)
8 (1)
Low
4992 (26)
1678 (31)
156 (25)
Middle
7174 (37)
2212 (41)
255 (42)
High
6447 (33)
1334 (24)
177 (29)