
Abstract
Background
Globally, workplaces have introduced non-smokers-only hiring policies to avoid hiring people who smoke since they cost thousands of dollars more annually to employ compared to non-smokers. Tobacco industry efforts gave rise to state smoker protection laws in the United States (U.S.), which protect people who smoke from employment discrimination.
Objectives
This study examined the association between living in a state with a smoker protection law and smoking status among U.S. adults and employment status and attempting to quit smoking in the past 12 months among those who currently smoke.
Design and Methods
Cross-sectional, nationally representative data from the 2015 – 2018 Behavioral Risk Factor Surveillance System were analyzed. Participants were U.S. adults who reported being unemployed or employed for wages. Unadjusted and adjusted logistic regression models controlling for race/ethnicity, income, education, health insurance, state, and sex assessed associations between living in a state with a smoker protection law and smoking status (n = 678,203) and employment status and attempting to quit smoking in the past 12 months among people who currently smoke (n = 110,630). Interactions for income were assessed.
Results
Smoker protection laws were not associated with smoking status in the overall sample (ORadj = 0.99, 95% CI: 0.89, 1.11) or employment among those who smoke (ORadj = 1.23, 95% CI: 0.92, 1.65). They were associated with a significantly higher odds of being employed (ORadj = 1.30, 95% CI: 1.06, 1.60) among those who smoke earning <$35,000. They were associated with a significantly lower odds of attempting to quit smoking among people who smoke (ORadj = 0.80, 95% CI: 0.66, 0.97), especially those earning <$35,000 (ORadj = 0.71, 95% CI: 0.53, 0.96) and $35,000-<$50,000 (ORadj. = 0.52, 95% CI: 0.32, 0.84).
Conclusions
While smoker protection laws may promote employment among low-income individuals who smoke, they may reduce quit attempts. Policies should promote evidence-based smoking cessation treatments to support quit attempts among people who smoke.
Introduction
Cigarette smoking is the leading cause of preventable death in the United States (U.S.) and globally.1,2 Despite an overall decrease in cigarette smoking in the last 50 years, 11.5% of adults in the U.S. and 22.5% of the global population still currently smoke.2,3 Smoking rates are highest among individuals of lower socioeconomic status.2,3
Globally and within the U.S., many workplaces have introduced non-smokers-only hiring policies to avoid hiring people who smoke since they cost thousands of dollars more per year to employ compared to non-smokers. 4 The first U.S. non-smokers-only hiring policies date back to the 1980s. Massachusetts was the first state to prohibit hiring public safety employees who smoked either on or off the job in an effort to reduce government related costs. 5 Non-smokers-only hiring policies have continued to gain popularity in the U.S. where legal. They have also spread globally beyond the governmental sector and can be found especially in healthcare organizations. 6 For example, the World Health Organization implemented a non-smokers-only hiring policy in 2005 to align their hiring practices with their public health efforts to reduce tobacco use. 7
In response to non-smokers-only hiring policies and concerns about potential decreases in tobacco use, the tobacco industry partnered with groups at the local level in the U.S. and launched a nationwide lobbying campaign to protect “smokers’ rights”, including protection from employment discrimination among people who smoke as an issue of right to privacy. 8 These tobacco industry efforts gave rise to state smoker protection laws, which protect people who smoke from employment discrimination. In New Jersey for example, Phillip Morris drafted the state’s original smoker protection law bill, which used civil rights language to completely prohibit any kind of employment discrimination among people who smoke. 9 We hypothesize that making it illegal to avoid employing people who smoke could be associated with increased smoking prevalence as well as increased employment and decreased quit attempts among people who smoke. The first smoker protection law was passed in Illinois in 1987 and the latest one was passed in Oklahoma in 2013. 10 Twenty nine states and the District of Columbia currently have smoker protection laws protecting people who smoke from employment discrimination, most of which were passed in the 1990s. 10 The exact wording of smoker protection laws has some slight variation across states. Smoker protections laws prohibit employers from refusing to hire or fire employees for using either “lawful products” or “tobacco products”. 11 Protecting people who smoke from employment discrimination has wide support in the U.S. A 2014 survey found that 86% of Americans disapprove of employer bans on hiring smokers. 12
With employment discrimination being legal in about half of U.S. states, previous research has debated the ethics of such practices. Arguments that support not hiring people who smoke include “denormalizing” and reducing tobacco use to support a culture of health, especially in healthcare organizations, and taking responsibility for behaviors that financially affect employers and fellow employees.13,14 Opponents of non-smokers-only hiring policies argue that such policies do not reduce tobacco use and are unfair to those who are more vulnerable to the burden of tobacco (eg, lower socioeconomic status, lower educational attainment, gay/lesbian, etc.), thus reducing job opportunities for these populations who already face barriers to employment.15,16 Experts have questioned whether non-smokers-only hiring policies reduce smoking as a population health goal or bolster institutional financial goals by blocking people who smoke from employment.15,16 Upon initial investigation, it appears that smoking prevalence rates are higher in states with smoker protection laws compared to states without smoker protection laws. 17 For example, the lowest smoking prevalence in states with smoker protection laws was California at 11.2% while the lowest smoking prevalence in states without smoker protection laws was Utah at 9.0% as of 2018. Similarly, the highest smoking prevalence in states with smoker protection laws was West Virginia at 25.3% while the highest smoking prevalence in states without smoker protection laws was Arkansas at 22.7%.
Despite such ethical discussions, no studies have examined the effects of smoker protection laws (protecting people who smoke from employment discrimination) on smoking rates at a population level and employment and cessation behaviors among people who currently smoke. Given that people who smoke are typically from a lower socioeconomic status, it is important to understand the impact of such policies on economic opportunities and smoking behaviors. The primary purpose of this paper is to test the hypothesis that living in a state with a smoker protection law is associated with a higher likelihood of smoking. The secondary purpose is to examine the association between living in a state with smoker protection law and employment status and attempting to quit smoking among people who currently smoke. We hypothesized that people who currently smoke who live in a state with a smoker protection law are more likely to be employed but less likely to have attempted to quit smoking.
Methods
A cross-sectional study was conducted using data from the Center for Disease Control and Prevention’s (CDC) Behavioral Risk Factor Surveillance System (BRFSS), RRID:SCR_012974. 17 BRFSS is an annual telephone-based survey that uses both cellphone and landline random digit dialing to collect health related information from U.S. residents over 18 years of age across all 50 states. BRFSS data from survey years 2015 – 2018 were analyzed and included respondents from all 50 states. Data beyond 2018 were excluded to remove the effects of the COVID-19 pandemic, which influenced smoking behaviors and employment.18,19 Among the 1,815,211 respondents, 830,310 individuals who were self-employed, a homemaker, student, retired, or unable to work were excluded since smoker protection laws only apply to employed positions. Since there were no meaningful differences found when using chi-square tests to assess for patterns of missingness, missing values were excluded (n = 306,698). The final sample size for the main analysis was n = 678,203. For the sub-analyses of people who currently smoke, n = 110,630 participants were included who indicated that they currently smoke. This publicly available, de-identified data from the CDC were exempt from IRB review.
Measures
The dependent variable for the main analysis was smoking status and measured by the question “Do you now smoke cigarettes every day, some days, or not at all?” Respondents were coded as a person who currently smokes if they answered every day or some days and non-smoker if they answered not at all. For the sub-analyses of people who currently smoke only, the dependent variables were attempting to quit smoking in the past 12 months and employment status. For quit attempt, participants were asked “During the past 12 months, have you stopped smoking for one day or longer because you were trying to quit smoking?” Responses were yes or no. For employment, participants were asked “Are you currently employed for wages, self-employed, out of work for one year or more, out of work less than one year, a homemaker, a student, retired, or unable to work. Those who indicated that they were employed for wages were coded as employed and those who indicated that they were out of work for one year or more or out of work less than one year were coded as unemployed. Those who indicated they were self-employed, a homemaker, student, retired, or unable to work were excluded from the final sample as stated previously.
States With a Smoker Protection Law

Information as of 2018.
Demographic covariates included race/ethnicity (White, non-Hispanic, Black, non-Hispanic, American Indian and Alaskan Native, non-Hispanic, Asian, non-Hispanic, Native Hawaiian, non-Hispanic, Native Hawaiian or Pacific Islander, non-Hispanic, Other, non-Hispanic, Multiracial, non-Hispanic, and Hispanic), household income (<$35,000, $35,000 - < $50,000, $50,000 - <$74,999, ≥ $75,000), education (did not graduate high school, graduated high school, attended college or technical school, graduated from college or technical school), health insurance (insured, uninsured), age, (18-29, 30-49, 50-64, 65+), and sex (male, female). These variables were examined as potential confounders because previous studies have found that they are associated with employment, smoking status, and attempting to quit smoking.20-22
Statistical Analyses
STATA Version 17 (StataCorp LP, College Station, TX) was used for all analyses. Survey weights using the STATA SVY command were applied to adjust for noncoverage and nonresponse and reflect regional and national population estimates. Descriptive statistics (weighted percentages and unweighted counts) were summarized overall and across those living and not living in a smoker protection law state. Chi-square tests were used to assess for demographic differences between respondents living and not living in a state with a smoker protection law. Logistic regression was used to generate odds ratios and 95% confidence intervals for the main analysis (association between living in a state with a smoker protection law and smoking status) and sub analyses of people who currently smoke (association between living in a state with a smoker protection law and attempting to quit smoking in the past 12 months and employment). For each logistic regression analysis, an unadjusted model and an adjusted model controlling for race/ethnicity, household income, education, health insurance, state, and sex were run. These covariates were selected since they demonstrated a statistically significant relationship with living in a state with a smoker protection law. We also assessed for statistical interaction using the STATA testparm command see if these associations differed by household income since these policies may affect lower income individuals disproportionately.
Results
Weighted Percentages and Unweighted Counts of Respondent Demographics Overall and by Smoker Protection Law Residence (n = 678,203)
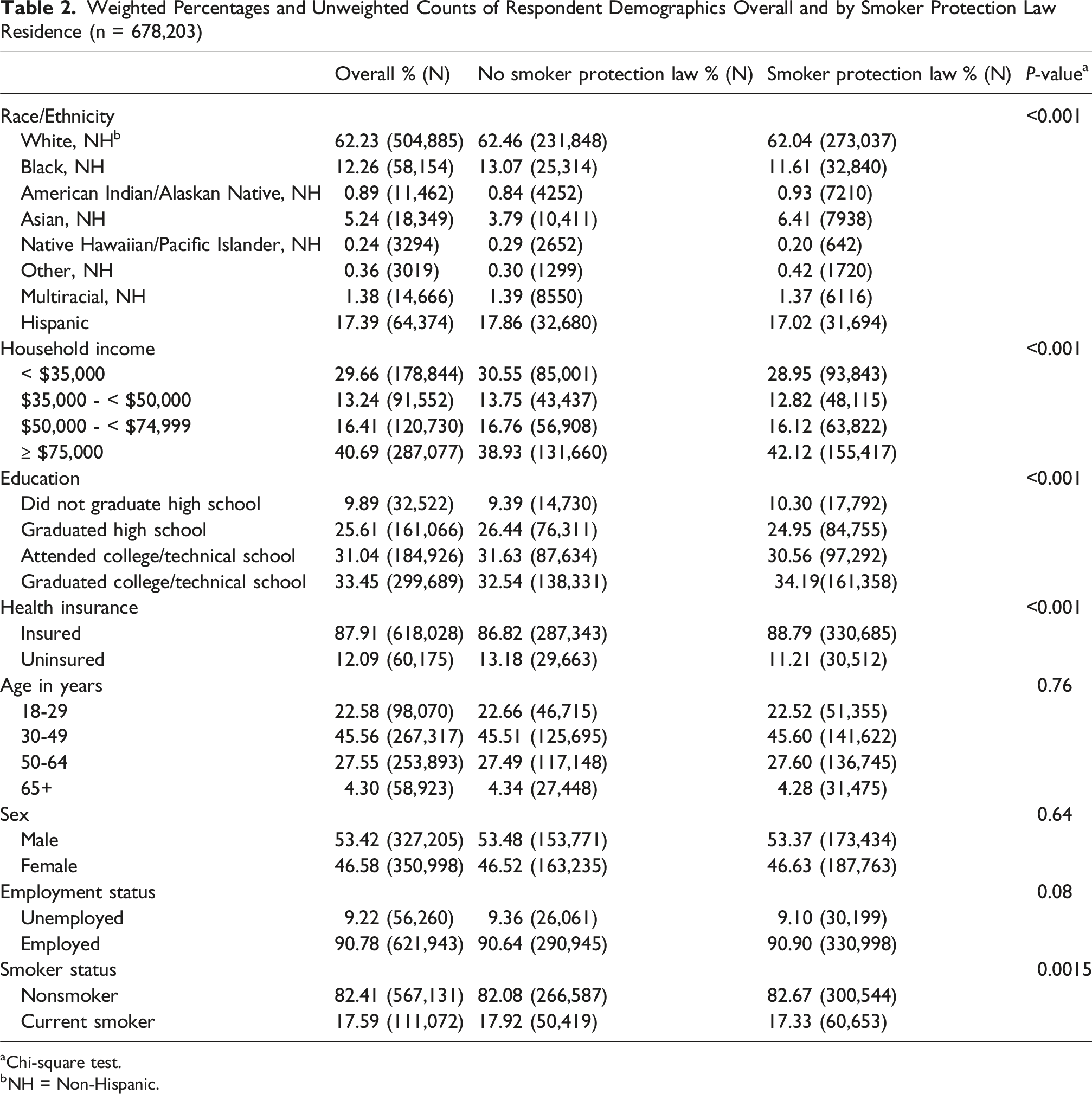
aChi-square test.
bNH = Non-Hispanic.
Logistic Regression Results for the Association Between Smoker Protection Laws With Smoking Status, Attempting to Quit Smoking in the Past 12 Months, and Employment Status

CI = confidence interval.
aAdjusted for race/ethnicity, household income, education, health insurance, state, and sex.
A statistically significant interaction with household income was found for the association between smoking status and living in a state with a smoker protection law (P-value <0.001) in the overall sample. When stratified by income group, a statistically significant association was not found among households earning <$35,000 (adj. OR = 1.06, 95% CI: 0.88, 1.27), $35,000 - <$50,000 (adj. OR = 1.03, 95% CI: 0.79, 1.36), $50,000 - <$74,999 (adj. OR = 0.89, 95% CI: 0.69, 1.15), and ≥$75,000 (adj. OR = 0.93, 95% CI: 0.75, 1.16). Results not shown in tables.
Adjusted Logistic Regression Results for the Association Between Smoker Protection Laws With Attempting to Quit Smoking in the Past 12 Months and Employment Status Among Current Smokers Stratified by Household Income
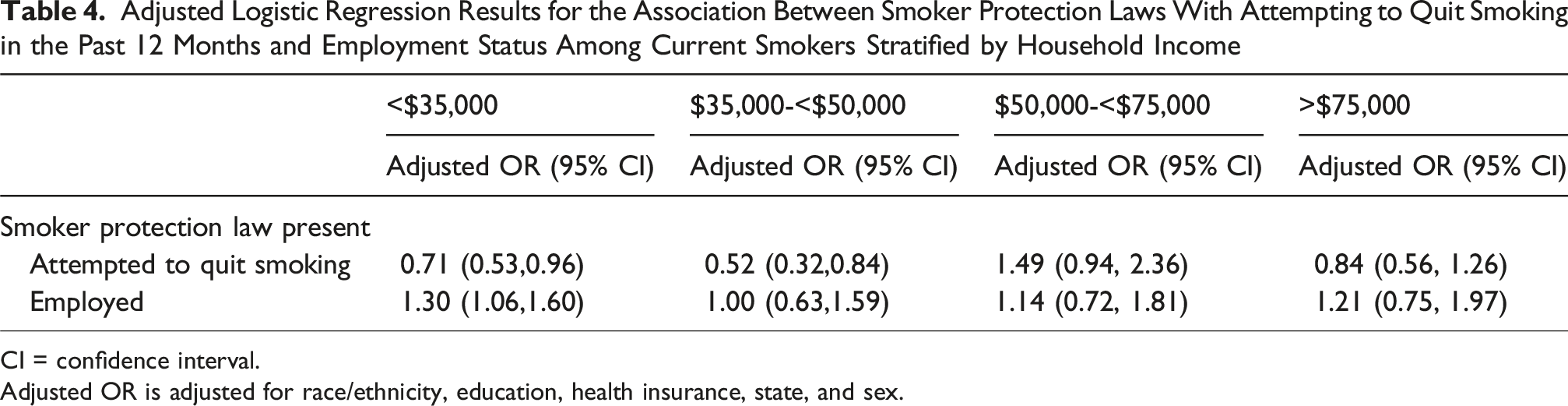
CI = confidence interval.
Adjusted OR is adjusted for race/ethnicity, education, health insurance, state, and sex.
Discussion
This study looked at the association between living in a state with a smoker protection law and smoking status in the overall sample and attempting to quit smoking and employment among people who currently smoke. Smoker protection laws weren’t associated with smoking status. While they weren’t associated with employment overall among people who currently smoke, they were associated with a higher odds of being employed among the lowest income group earning >$35,000 who currently smoke. Smoker protection laws were also associated with a lower odds of attempting to quit smoking, especially among the two lowest income groups.
This study did not find differences in smoking status across residents of states with and without a smoker protection law. Conversely, refusing to hire people who smoke may reduce smoking rates, although evidence is limited. 23 The Cleveland Clinic, located in Cuyahoga County, Ohio stopped hiring people who smoke in 2007. Smoking rates in Cuyahoga County dropped more than five percent between 2005 and 2009, which was much greater than the state’s overall decline in smoking rates during that same period of about two percent. 23 Based on this analysis, it’s unclear as to whether this greater decline in smoking was due to a change in hiring practices or other factors. For example, there are in person smoking cessation resources available through the Cleveland Clinic that could have contributed to the observed declines within Cuyahoga County compared to the rest of the state. 24 Furthermore, smoker protection laws are state-level laws and there is no federal law that protects people who smoke from employment discrimination in the workplace. Therefore, it’s up to states to enforce these laws. It’s possible states with smoker protection laws are not enforcing them, resulting in employers in both states with and without smoker protection laws refusing to hire people who smoke. This could explain why differences in smoking were not observed across states with and without smoker protection laws. It’s also possible that these laws do not affect smoking rates and that the tobacco industry’s concerns were invalid. A systematic review found that health concerns were the primary reason why people who smoked quit, not concerns around employment. 25 Lastly, it’s also possible that smoker protection laws may be associated with shifts in smoking patterns rather than smoking rates. One study found that workplace smoking bans do not affect the amount of cigarettes that people smoke, but rather influence their smoking behaviors and makes it so that they compensate for such bans by smoking off of work-site properties. 26
Surprisingly, we did not find differences in employment among those who lived in a state with or without a smoker protection law in the overall sample of people who currently smoke. Previous research has found that people who smoke are less likely to be employed and reemployed compared to non-smokers. 27 It’s possible that employers in states with smoker protection laws are still discriminating against hiring people who currently smoke due to a lack of oversight, thus diminishing any potential differences in employment among people who currently smoke in states with and without these laws. For example, California has had a smoker protection law since 2005. 10 A 2020 qualitative study of people who currently smoke recruited from San Francisco’s Employment Development Department reported that their employers had written language in the employee handbook saying that they could be terminated due to their smoking status. 28 It’s possible states with smoker protection laws are not enforcing them, resulting in employers in both states with and without smoker protection laws refusing to hire people who currently smoke either intentionally or unintentionally. This could explain why differences in employment were not observed across states with and without smoker protection laws in the overall sample of smokers. Previous research using national samples in the U.S. have found that people who currently smoke are often perceived as less qualified and have worse impressions during the hiring process compared to non-smokers.29-31 Hiring discrimination among people who currently smoke may be related to smoking-related stigma and unintentional practices stemming from implicit bias among employers rather than formal workplace hiring policies.
While an association was not found in the overall sample of people who currently smoke, smoker protection laws were associated with an increased odds of employment only among people who currently smoke only in the lowest household income group earning less than $35,000. This indicates that these laws may provide employment protection specifically for individuals with low socioeconomic status who smoke. In general, people who smoke tend to earn lower wages and work in industries such as food service, construction, and mining. 32 It’s important to note that service and construction industries are less likely to offer health insurance compared to other industries in the U.S., which is a predictor of smoking cessation.33,34
Interestingly, this study found that people who currently smoke who lived in a state with a smoker protection law were less likely to report attempting to quit smoking in the past 12 months compared to those who live in a state without a smoker protection law. When stratified by income, this finding applied to the lowest two household income groups (those earning less than $50,000) but was not seen in higher earners. Given that this is the first study to look at the association between smoker protection laws and smoking behaviors, it’s possible that smoker protection laws disincentivize people who currently smoke from trying to quit since they are protected from employment discrimination, especially among those with lower incomes who face unique barriers across the different phases of smoking cessation. 35 Other studies have focused on the effects of workplace smoking bans rather than policies around hiring smokers. Workplace smoking bans may support smoking cessation and are recommended by the U.S. Task Force on Community Preventive Services. 36 A systematic review found that work sites with smoke-free policies are associated with a 3.8% reduction in tobacco use, or 1.3 fewer cigarettes per day. 37 Another study found that people who smoke who work in a place with a strong workplace ordinance against smoking are more likely to report quitting smoking within 6 months. 38 A systematic review found that smoking bans in workplaces or public did not have differential effects across socioeconomic status. 39 However, it’s important to note that workers with a high school education or less and those with low income earning <$35,000 per year are less likely to be covered by a smoke-free policy in the workplace. 40
Strengths and Limitations
This study had several strengths. The study sample was obtained through random digit dialing, thus reducing sampling bias. The study sample was also nationally representative, making these results generalizable to U.S. adults. Despite these strengths, there are some limitations. An a priori power analysis was not conducted for this study. However, this study should have adequate statistical power given the large overall sample size. BRFSS data is cross-sectional, thus limiting the ability of the study to establish causal relationships. The independent variable was defined as living in a state with or without a smoker protection law, which assumes that all states apply these laws equally. We were unable to measure actual employment discrimination faced by people who smoke and whether these laws are being enforced across all states. Furthermore, smoker protection laws are not homogenous across all states. For example, only seven states explicitly apply smoker protections to all workers while the others include or carve out specific workers and industries (eg, public employees, healthcare workers, etc.). Given sample size limitations for a sub analysis and the inability to identify each participant’s specific occupation, the heterogeneity of smoker protection laws is a limitation to this analysis. Residual confounding may be an issue given that this is an observational, cross-sectional study. We were unable to measure employer specific smoking policies, which could vary greatly. While we found that living in a smoker protection law state was associated with a reduced odds of attempting to quit smoking, it’s possible that these results could be explained by confounders that were not accounted for in this study. For example, there could be differences in smoking cessation insurance coverage across states with and without smoker protection laws. Lastly, these policies were passed well before the 2015 – 2018 data included in this study, many of them in the 1990s. Thus, this limits our ability to fully decipher the effect of the passage of these policies on smoking behaviors and employment. While conducting a pre and post policy analysis of the data would be ideal, the BRFSS weighting and sampling methodology changed in 2011 and therefore should not be compared with previous years of BRFSS data.
Conclusions
This is the first study that has examined the potential impacts of smoker protection laws (protecting people who smoke from employment discrimination). These findings provide initial evidence that smoker protection laws may reduce quit attempts among people who currently smoke, especially among those with low income but may also support employment among low-income people who currently smoke. While these laws may have beneficial results on employment for people who smoke, the potential negative effects of smoker protection laws on cessation should be addressed in the greater context of health policy, especially given the Healthy People 2030 goal of increasing quit attempts among adults who currently smoke. 41 Alternative and/or additional policies should be considered in conjunction with smoker protection laws that promote cessation and access to evidence-based smoking cessation programs, especially among those who are low-income. For example, employers should be required to provide health insurance to all employees to increase access to evidence-based cessation treatments for people who smoke, especially in states with smoker protection laws, since health insurance has been shown to be a predictor of smoking cessation. 34 State officials, especially those in states with smoker protection laws, could consider increasing cigarette taxes since increasing the price of cigarettes has been shown to increase cessation with the greatest effect on those with low socioeconomic status. 39 Future research should use longitudinal study designs to establish temporal effects of smoker protection laws that take their heterogeneity into account.
Footnotes
Ethical Considerations
This publicly available, de-identified data from the Centers for Disease Control and Preventions is exempt from IRB review.
Author contributions
Moges R contributed to the formal analysis, drafted the original manuscript, and contributed to manuscript review and editing; Iaria R drafted the original manuscript and contributed to manuscript review and editing; Lent AB secured funding, supervised the project, conceptualized the study, supervised the formal analysis, drafted the original manuscript, and contributed to manuscript review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BEACoN Research Scholars Program at California Polytechnic State University San Luis Obispo and National Institute of General Medical Sciences, URISE program (URISE at Cal Poly, grant number: 5T34GM149492).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.