
Abstract
Objective
To investigate the effectiveness and efficiency of inpatient rehabilitation.
Methods
A total of 2,081 patients across 14 hospitals were recruited in this prospective, multicenter cohort study. Data on the diagnoses, types of admission, length of stay (LOS), and functional ability score based on a modified Barthel index (BI) at admission (BIa) and at discharge (BId) were collected. Effectiveness was defined as the difference of BI (ΔBI) and efficiency as ΔBI divided by LOS.
Results
The majority of patients were diagnosed with spinal cord injury and stroke (41.8% and 37.5%, respectively). The mean age was 52.4 ± 18.6 years with a mean LOS of 23.9 ± 19.9 days, BIa of 9.4 ± 6.1, and BId of 12.3 ± 5.7. The overall effectiveness and efficiency were 2.9 ± 3.4 and 0.16 ± 0.30 scores/day, respectively; stroke rehabilitation provided the most effective and efficient BI improvement compared with rehabilitation for other diseases. Most patients (54.5%) received intensive functional rehabilitation, which was the most effective and efficient program (4.4 ± 3.6 and 0.23 ± 0.32 scores/day, respectively); the efficiency of the intensive program was not different among various diseases (P
Conclusion
Stroke rehabilitation had the highest efficiency compared with rehabilitation for other neurological diseases. The most efficient type of admission was intensive rehabilitation, regardless of the disease being treated.
Introduction
Rehabilitation is a process that focuses on reducing disability, decreasing dependency, and increasing the quality of life. 1 During hospitalization, rehabilitation has to maximize the function of patients to maintain the highest possible level of independence. However, the level of independence may be improved or worsened after discharge. Paolucci et al assessed the functional level of stroke patients at one year after discharge from a rehabilitation hospital and found that 43.3% of patients maintained the level they achieved during inpatient rehabilitation treatment, 23.6% improved, and the rest worsened. 2 The duration of the inpatient rehabilitation process has to be balanced between the limitations of hospital resources and the benefits of patients during the hospitalization. 3 A prolonged hospitalization represents a higher expense that becomes an economic burden for both the hospital and the patients. The development of an efficient therapy that can maximize the functional level of patients during a short length of stay (LOS) is warranted.
In Thailand, only a limited number of beds are available for rehabilitation services targeting disabled patients during the subacute disease phase. Patients who can access the rehabilitation services should have maximal functions. Therefore, authors need to find out a national key performance indicator (KPI) for benchmarking among centers and for improving the quality of services in the country. In addition, the proper selection of patients who are likely to benefit from inpatient rehabilitation services is crucial. The present study aimed to determine the effectiveness and efficiency of inpatient rehabilitation services in Thailand and the factors related to effectiveness.
Methods
The present study was a prospective, multicenter cohort study performed in the rehabilitation wards of 14 centers, including six university hospitals, three rehabilitation centers, and five general hospitals in Thailand. The study was conducted in accordance with the ethical principles stated in the most recent version of the Declaration of Helsinki. 4 After receiving approval from the ethics committee of each center, all patients admitted in the rehabilitation wards from January to December 2012 were recruited. The inclusion criteria were patients who were admitted in the rehabilitation wards during that period and willing to participate. Participants gave permission by signing the informed consent, which was prior to their participation in the study.
As most patients previously admitted to our rehabilitation wards suffered from neurological diseases, the diagnoses in this study were categorized into the following four groups according to the most common diseases in our wards: (i) stroke, (ii) spinal cord injury (SCI), (iii) traumatic brain injury (TBI), and (iv) other diseases. At baseline, the demographic data, including age, sex, onset-to-admission interval (OAI), diagnoses, and types of admission, were recorded. Then, the functional assessment was performed using Barthel index (BI). 5 The formal rehabilitation assessment composed of biopsychosocial aspects was performed by a multidisciplinary team, including nurses, physical therapists, occupational therapists, speech therapists, rehabilitation psychologists, and recreational therapists, as required.
After the assessment, rehabilitation doctors determined the types of admission, which were categorized into the following six groups: (i) intensive rehabilitation, aiming for improving functions, for patients who could tolerate a rehabilitation program of at least three hours/day; (ii) less-intensive rehabilitation, for patients who could tolerate a program of one to two hours/day; (iii) investigations, for patients who needed any examination, for example, regular checkup of the urinary system in SCI patients; (iv) caregiver training, for patients whose caregivers needed to be trained in providing proper care for these patients; (v) treatment of complications, for patients who needed hospitalization because of serious complications, including pneumonia, pressure ulcer, or deep vein thrombosis; and (vi) others, for other types of admission than those mentioned above. Functional rehabilitation program could be intensive or less intensive depending on the conditions of patients. Other types of admission, including investigation, caregiver training, and treatment of complications, were nonintensive programs. Patients admitted for functional training underwent a standard rehabilitation program that was composed of therapeutic exercises, self-care training, balancing and ambulation training, counseling, and recreational activities as appropriate. These programs were prescribed by the rehabilitation doctors, and the services were delivered by our multidisciplinary team with the team meeting every week.
The outcomes of inpatient rehabilitation services were functional scores (BI), LOS, effectiveness, and efficiency. The functional abilities of the patients were evaluated twice using a modified BI, BI at admission (BIa) and BI at discharge (BId). BI is a tool to measure the functions of patients undergoing rehabilitation programs in Thailand. It is composed of self-care functions, balancing, and ambulation abilities for 10 activities. 5 The score ranges from 0 to 20; a higher score represents a better function. Regarding the LOS, we measured the time from rehabilitation admission to discharge. The criterion of discharge was patients gaining maximal functions, which was evaluated using BI every week. Patients whose BI was stable for two consecutive weeks were discharged from the rehabilitation wards.
The effectiveness and efficiency of the rehabilitation services were evaluated using BI and LOS data. The effectiveness of rehabilitation services was calculated from the difference between BId and BIa (ΔBI = BId–-BIa). The efficiency was calculated by dividing the effectiveness by LOS (ΔBI/LOS). Additionally, factors related to the improvement in effectiveness were analyzed, including age, sex, OAI, level of care, BIa, LOS, diagnosis of stroke, and types of admission. The improvement in effectiveness was defined as the number of patients with an improved functional score after rehabilitation. In addition, the method was included in the concept of Rehabilitation Treatment Taxonomy. 6
Statistical analysis
Data are presented as mean and standard deviation (±SD), median and range, or number and percentage (%) as appropriate. One-way analysis of variance was used to compare continuous data, including BI and LOS. Multiple logistic regression was used to analyze factors affecting the improvement in effectiveness. Factors included in the analysis were age (≥60 vs. < 60 years), sex (female vs. male), OAI (< 3 vs. ≥3 months), level of care (university hospitals vs. others), BIa (< 10 vs. ≥10), LOS (≥30 vs. < 30 days), diagnosis (stroke vs. nonstroke), and types of admission (intensive vs. nonintensive rehabilitation). A
Results
In 2012, 2,145 patients were admitted to the 14 rehabilitation wards. Of these, 64 patients were excluded from the analysis because they were either transferred to other wards on account of severe medical conditions (52 cases) or their data were incomplete (12 cases), resulting in 2,081 patients for analysis. Of these patients, 42.8% were admitted to university hospitals, 30.2% to rehabilitation centers, and 27.0% to general hospitals. The patients had a mean age of 52.4 ± 18.6 years, and 63.9% were male. The median OAI was 5 months (range 0.03-492 months). The three most frequent diagnoses were SCI (870 cases, 41.8%), stroke (780 cases, 37.5%), and TBI (117 cases, 5.6%). Other diagnoses included other neurological diseases (76 cases, ie, multiple sclerosis, Parkinsonism, polyneuropathy, and Guillain-Barre syndrome), other musculoskeletal diseases (84 cases, ie, fracture, joint replacement, amputation, and arthritis), chronic pain (72 cases, ie, pain in the neck, back, and extremity), and others (82 cases, ie, postcardiac surgery, other pulmonary diseases, and multiple trauma). Regarding the types of admission, the majority of patients (1,134 cases, 54.5%) were admitted for intensive rehabilitation, whereas 7.4% were admitted for less intensive rehabilitation, 18.2% for investigation, 4.8% for caregiver training, 2.6% for treatment of complications, and 12.5% for other objectives (Table 1).
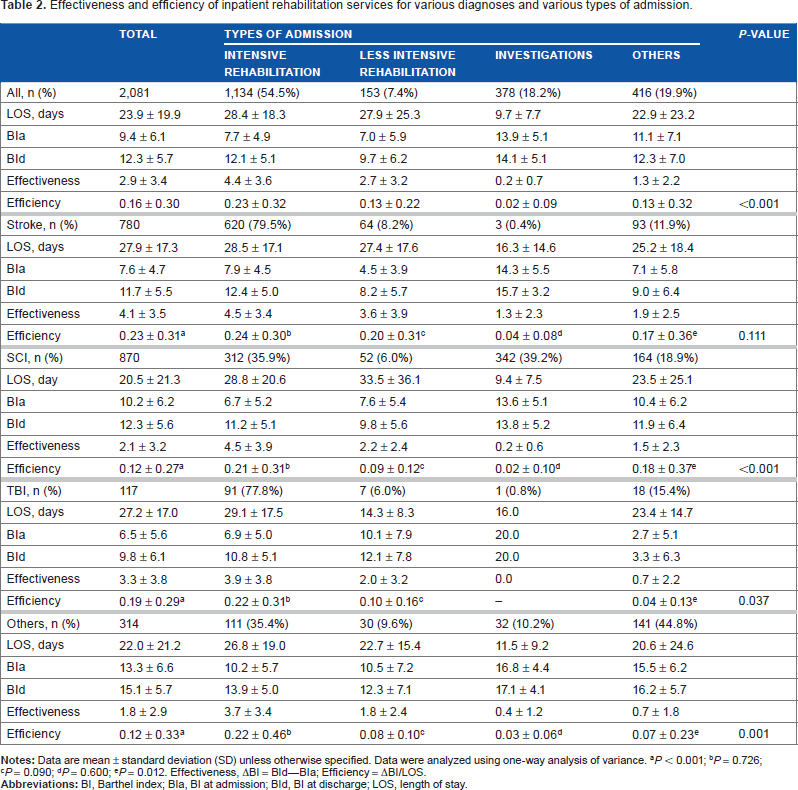
Table 2 presents the effectiveness and efficiency of inpatient rehabilitation programs. The overall LOS was 23.9 ± 19.9 days. The overall BI at admission was 9.4 ± 6.1, which improved to 12.3 ± 5.7 at discharge. This resulted in a mean effectiveness of 2.9 ± 3.4 (BI scores) and a mean efficiency of 0.16 ± 0.30 (BI scores/day). Among the rehabilitation programs for various neurological diseases, those for stroke patients had the highest effectiveness and efficiency (improvement of 4.1 ± 3.5 BI scores and 0.23 ± 0.31 BI scores/day,
Demographic data of 2,081 patients.
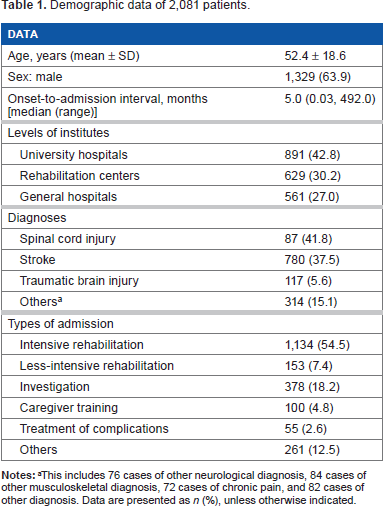
This includes 76 cases of other neurological diagnosis, 84 cases of other musculoskeletal diagnosis, 72 cases of chronic pain, and 82 cases of other diagnosis. Data are presented as
Factors affecting the effectiveness of inpatient rehabilitation programs were disease diagnosis, types of admission, level of care, age, OAI, BIa, and LOS. However, on multivariate analysis, the inpatient rehabilitation program had the highest effectiveness for stroke patients who had OAI < 3 months, BIa < 10, were admitted for an intensive rehabilitation program, and had LOS $30 days (Table 3).
Discussion
Inpatient rehabilitation with a multidisciplinary team approach for various diseases is the main factor for successful rehabilitation outcomes.7,8 However, there is a cost/benefit tradeoff for inpatient rehabilitation related to the cost of admission. Therefore, identification of the most efficient rehabilitation programs is essential for a country with limited resources such as Thailand. This study aimed to determine the effectiveness and efficiency of inpatient rehabilitation services in the context of our country. Although the concepts behind effectiveness and efficiency have diverse meanings across disciplines, the effectiveness and efficiency in this study are indirect or derived from hypothesis-driven proxy data, such as the delta change in BI scores and the delta change in BI scores divided by the duration of rehabilitation stay, respectively.
The most common diagnoses in our rehabilitation wards were stroke and SCI, comprising ~80% of the patients. These conditions cause permanent disability requiring rehabilitation. Karges and Smallfied suggested that the inpatient rehabilitation process for stroke patients improves the functional scores at discharge. 9 Our study showed that the inpatient rehabilitation for stroke patients had the highest efficiency compared with those for other neurological diseases. The reason why we chose stroke as a factor related to the effectiveness was most of stroke patients (~80%) were admitted for intensive functional training compared to SCI patients (35.9%), even though SCI was the most common diagnosis. Although stroke patients had longer LOS than did SCI patients, the rehabilitation for stroke patients was still more efficient (0.23 vs. 0.12 BI scores/ day). This was because a higher proportion of stroke patients were admitted for extensive periods of intensive rehabilitation, which was the most efficient rehabilitation program.
In 2009, we reported the LOS, effectiveness, and efficiency in 327 stroke patients admitted to nine rehabilitation wards. 10 The mean LOS was 27.3 days. Mean and SD of BIa and BId were 7.48 ± 3.96 and 13.27 ± 4.86, respectively (BI: 0-20). The change score was 5.79 ± 3.89, and the functional efficiency score was 0.28 scores/day, which were better than indicators in this study. This may be because the previous study gathered data from tertiary hospitals and recruited only stroke patients with good potential for rehabilitation, whereas subjects in this study had various types of admission and had many different diagnoses not only stroke. However, if we considered only the stroke and intensive types of admission, the efficacy in this study was similar to that in the previous study (0.24 ± 0.30 vs. 0.28 ± 0.30 scores/day, respectively).
Effectiveness and efficiency of inpatient rehabilitation services for various diagnoses and various types of admission.
Additionally, Koh et al reported the trade-offs between effectiveness and efficiency during inpatient subacute stroke rehabilitation, regarding admission functional status and LOS. 11 They suggested that BIa of 30-62 (BI range: 0-100) and LOS of 37-41 days can yield rehabilitation outcomes of optimal effectiveness and efficiency. In the previous study, Shah et al reported that stroke patients, who exhibited the most improvement after rehabilitation, appeared to be the patients with initial BI scores of 40-80. 12 The patients in our study had higher BIa (7.6-7.9; BI range scores of 0-20) and shorter LOS (27.9-28.4 days) compared with those in the study by Koh et al. 11
Factors related to the effectiveness of rehabilitation service.

Number of patients whose functional score increased after rehabilitation.
Multiple logistic regression.
Nonintensive group included less-intensive, investigation, caregiver training, treatment for complications, and other types of admission.
Concerning SCIs, only one-third of our patients with SCI were admitted with the type of intensive therapy. Approximately 40% of patients with SCI were admitted for investigation of their bladder functions. However, the efficiency of rehabilitation for patients with SCI in our study was better than that of the study by Rinkaewkan and Kuptniratsaikul, who performed a retrospective study of patients with SCI admitted to the rehabilitation ward at Siriraj Hospital between 2006 and 2010. 13 When considering the new SCI patients who were admitted for intensive rehabilitation, the average LOS was similar to that of stroke patients (28.8 vs. 28.5 days, respectively). In addition, the effectiveness and efficiency of the intensive rehabilitation for SCI were similar to those of stroke patients (4.5 ± 3.9 vs. 4.5 ± 3.4 BI scores and 0.21 ± 0.31 vs. 0.24 ± 0.30 BI scores/day, respectively).
Although the efficiency of inpatient rehabilitation programs varied among patients with various diseases, the efficiency was comparable if they were admitted with an intensive rehabilitation program. Our findings indicated that patients with neurological diseases would gain greater benefit from rehabilitation if they could tolerate a training program lasting >3 hours/day according to our definition of intensive rehabilitation. The findings of our study were in line with those of other studies that confirmed the benefit of intensive rehabilitation programs, even though the definition of intensity varied among studies.14–16 The intensive program should involve training of at least 3 hours/day for 4-5 days/week. 11 If patients can tolerate higher rehabilitation training intensity, they would gain greater improvements in terms of functional scores.17,18 Moreover, Hu et al reported that the rehabilitation intensity significantly predicted the BId, especially for walking function. 16
Regarding the effectiveness and efficiency of rehabilitation, Chen et al in 2005 performed a retrospective study of 12,506 patients (stroke 40.6%, fracture 30.4%, no SCI) with a mean age of 73.2 ± 11.5 years. 19 They found an average LOS of 31 days, and an efficiency score of 12.9 per 30 days (BI: 0-100). The present study found a higher efficiency than that reported in the study by Chen et al (0.16 vs. 0.09 scores/day, respectively, using a similar range score). The ratio of stroke patients admitted for rehabilitation programs and the average LOS of our study were similar to those reported in the study by Chen et al. However, our subjects were younger than those in their study (52.4 ± 18.6 vs. 73.2 ± 11.5 years).
Concerning the factors affecting the effectiveness of rehabilitation services, besides stroke and intensive types of admission, we found that shorter OAI (< 3 months), lower BIa (< 10), and longer LOS (≥30 days) resulted in better ΔBI. Previous studies showed that various factors can influence the effectiveness and/or efficacy of rehabilitation services. For example, Chow et al reported that the factors associated with poorer rehabilitation effectiveness and efficiency were older age, ethnicity, delayed admission, admission diagnosis of amputation, and comorbidities of dementia and stroke. 20 Pinedo et al found that neurological severity, hemiparetic severity, impairment of deep sensation, and trunk control on admission can influence the rehabilitation efficiency. 21 Moreover, Koh et al showed that older age, race-ethnicity, caregiver availability, ischemic stroke, longer time to admission, dementia, BIa, and LOS were independent predictors of poorer rehabilitation effectiveness. 11
Our study had some limitations. (1) Half of the rehabilitation wards in our study were in university hospitals and three in rehabilitation centers; therefore, the data might not be applicable to secondary or primary care hospitals. (2) Most subjects in this study were diagnosed with a neurological disease; very few patients with orthopedic conditions were recruited. Based on our clinical experience, orthopedic patients usually have shorter LOS and better prognosis compared with neurological patients. Generally, they do not require rehabilitation as intensively as patients with neurological conditions. (3) Lack of attention to severity of participants’ disabilities in the analysis. Patients with different levels of disabilities at baseline gain different effectiveness and efficiency. This study analyzed average BI scores, which could eliminate potential for assessing the effectiveness and efficiency of rehabilitation services. Further studies concerning the level of disabilities at baseline should be performed to definitely confirm the effectiveness and efficiency of rehabilitation services.
Conclusion
Rehabilitation for stroke patients had the highest efficiency compared with that for other neurological diseases. The rehabilitation service for patients with intensive rehabilitation goals had the highest efficiency, regardless of the diseases being treated. Factors related to the effectiveness of inpatient rehabilitation program were stroke patients with an OAI < 3 months, BIa < 10, and LOS of ≥30 days, who were admitted for intensive rehabilitation programs.
Author Contributions
Conceived and designed the experiments: VK, WL, JK. Analyzed the data: VK, PW, UW, PL, KS, KI, PTunwattanapong. Wrote the first draft of the manuscript: VK, PW, UW, KS, PL, KI. Contributed to the writing of the manuscript: VK, PM, JK, SS, PTunwattanapong. Agree with manuscript results and conclusions: VK, JK, SS, PThamronglaohaphan, WL, WW. Jointly developed the structure and arguments for the paper: VK, PW, PL, KI, JK, PThamronglaohaphan, WW. Made critical revisions and approved final version: VK, PW, UW, KS, PL, KI, PTunwattanapong. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors thank Ms. Daranee Prukshyajiva for her assistance with the coordination of data collection, Mr. Suthiphol Udompunturuk and Ms. Julaporn Poolium for statistical analyses, and Professor Manee Rattanachaiyanont for reviewing the manuscript.