
Abstract
Aim
This study aimed to investigate the relationship between sarcopenia and change in bone mineral density (BMD) and functional outcome in hip arthroplasty patients.
Introduction
As aging progress, ongoing changes in body composition lead to bone and muscle loss. 1 Much of this physical impairment is due to the gradual deterioration of bone (osteopenia) and progressive decline in lean tissue. 2 In 1989, Rosenberg defined sarcopenia as the loss of lean body mass, and this term is now broadly used to refer to the involuntary decline of muscle mass and strength, 3 and osteoporosis was defined as a bone mineral density (BMD) of <2.5 standard deviations below the sex-specific young adult mean. 4 The prevalence of sarcopenia has been reported to be between 10% and 40% in a postmenopausal population, depending on which reference method and reference population are being used. 5 Osteoporosis affects approximately 30% of the female population aged >50 years. 6 Decreased muscle mass and BMD are significant changes that occur with aging, which are often associated with the inability to adapt to external stress resulting in falls, trauma, functional disability, increased hospitalization, decreased quality of life, and increased mortality. 7 The aging of the Korean population is expected to result in an increase in the prevalence of hip fractures. 8 Therefore, it is important to predict risk factors for sarcopenia and osteoporosis in patients with hip fractures and screen them early.
In most studies,5,7,9 sarcopenia is negatively correlated with BMD, and sarcopenia and osteoporosis are strongly correlated with the risk of bone fracture. Lima et al 3 noted that fat-free mass is significantly correlated with BMD independently of height and fat mass. However, all studies were cross sectional studies, and no studies were conducted on the change in BMD through follow-up observation.
Juan I et al reported that the association between sarcopenia and worse prognosis at discharge in acute hip fracture patients could not be confirmed. 10 Steinhaug et al demonstrated that sarcopenia did not predict change in mobility in 1 year after hip fracture. 11 However, in other studies,12–14 sarcopenia was independently associated with worse functional outcomes at rehabilitation discharge, with poor recovery after returning home, and increased the risk for5-year mortality in patients with osteoporotic hip fracture. Owing to various surgical methods depending on the type of hip fracture 8 and rehabilitation process, 15 a study is needed for patients who received the same surgery and rehabilitation protocol.
Thus, this study aims to investigate the relationship between sarcopenia and change in BMD, functional outcome in old-aged hip arthroplasty patients. The hypothesis of this study is that sarcopenia would affect BMD and functional outcome after hip arthroplasty.
Material and Methods
Demographics and Clinical Characteristics
All patient data have been collected prospectively and reviewed retrospectively, and the study was approved by the institutional review board of Wonkwang University Hospital.
Demographics between patients in sarcopenia and non-sarcopenia groups/This data is presented as mean ± standard deviation or number (%) ASA: American Society of Anesthesiologists physical status classification, BMI: Body mass index, THR: Total hip arthroplasty, Hemi.: Hemiarthroplasty, 25 (OH)D: 25-hydroxyvitamin D, PTH: Parathyroid hormone, ALP: alkaline phosphatase.

Assessment of Sarcopenia and Osteoporosis
The diagnosis of sarcopenia was defined based on the criteria of the Asian working group for sarcopenia (AWGS), which requires both low muscle mass and low handgrip strength. 16
Muscle mass was measured using dual energy X-ray absorptiometry. Body fat percentage and appendicular skeletal muscle mass (ASM) are normalized to size (total lean muscle mass in the upper and lower limbs divided by the square of the body height). The relative appendicular skeletal muscle mass index identifies low muscle mass with a threshold of 7 kg/m2 for men and 5.4 kg/m2 for women based on the consensus of the AWGS. 16
Muscle strength was evaluated using hand grip strength. 17 Hand grip strength was measured by a hand-held dynamometer (Jamar adjustable dynamometer, Asimow Engineering, Los Angeles, CA, USA) while the patient was sitting in bed or on a chair with the elbow flexed and wrist in the neutral position. Patients were instructed to grip the device 3 times in each hand as possible. The same investigator made measurements for all participants and was blind to the clinical data. For each participant, the best of the 6 measurements was used. Hand grip strength of <26 kg for men and <18 kg for women is the low hand grip strength based on threshold values recommended by the AWGS.
Dual-energy X-ray absorptiometry (Horizon W; Hologic Inc, MA, USA) was used to assess BMD (g/cm2) of the hip (total femur, femur neck) and lumbar spine (L1-L4) at baseline and at 1-year intervals. BMD measurements were performed 1 week after surgery and 1 year after surgery. We calculated the annual percentage of change in BMD for each participant as follows: [(BMD2 − BMD1)/BMD1]*100 between assessments. (BMD1: BMD measured at baseline, BMD2: BMD measured at 1-year follow-up period).18Quality controls for the DXA equipment were undertaken daily according to the manufacturer’s guidelines to verify the stability of the system. No change was observed during the entire study period.19
Functional Outcome Measurement
Functional status was assessed using the modified Barthel index (MBI) total score. This examination was based on preoperative conditions, post-operative conditions, 3 months after surgery, and 1 year after surgery. 13 Barthel index is calculated using 10variables that represent ADL and mobility. A higher value is associated with a greater likelihood of being able to live at home with a degree of independence following discharge from hospital.
Statistical Analysis
To compare the characteristics of sarcopenia and non-sarcopenia groups, a T-test was conducted, and the results are shown as mean ± standard deviations. A Chi-square test was also conducted to assess gender, BMI, and comorbidities. BMD figures and their rate of change were also analyzed by independent sample T-test. Statistical significance was set at P < .001, and all analyses used SPSS version 23.0.
Results
Grip strength *Low relative appendicular skeletal muscle: men,<7 kg/m2; women<5.4 kg/m2.

BMD of patients in sarcopenia and non-sarcopenia groups/Data are shown as mean ± standard deviation. BMD: bone mineral density.

Change in BMD in sarcopenia and non-sarcopenia groups/Data are shown mean ± standard deviation.

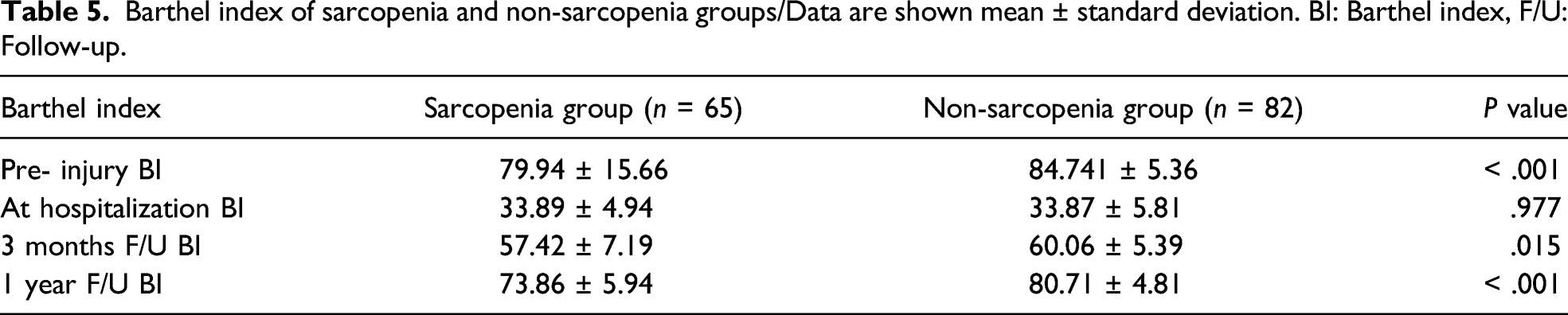
Barthel index of sarcopenia and non-sarcopenia groups/Data are shown mean ± standard deviation. BI: Barthel index, F/U: Follow-up.
Discussion
Based on the results of our study, the sarcopenia group showed lower BMD than the non-sarcopenia group at both times. However, the change rate in BMD was no statistically significant difference between the 2 groups. The functional outcome, expressed in the Barthel index, showed statistically lower results in the sarcopenia group than in the non-sarcopenia group except at the time of hospitalization.
The cross-sectional view, both during hospitalization and at 1-year follow-up after surgery, showed statistically significantly lower BMD in the sarcopenia group. Hunter et al reported that there was no association and between sarcopenia and osteopenia or osteoporosis. 2 Gillette-Guyonnet et al also reported that their study did not show a positive association between sarcopenia and osteoporosis. 18 However, other studies reported that sarcopenia was significantly associated with osteopenia and osteoporosis.3,5,9,19 Our findings also corresponded with existing findings, which could be attributed to the fact that the muscle and bone have common genetic, nutritional, lifestyle, and hormonal determinants operating mainly during growth. 9 In previous studies, it has been assumed that much of the simple weight can increase BMD under the bone-muscle relationship (Wolf’s rule), but this can be offset by bone resorption associated with inflammatory cytokine synthesis rather than increased BMD under the mechanical loading offat. 9 Moreover, some scientific studies reported that cell signals that promote mesenchymal stem cells to differentiate into the adipogenic pathway are associated with the suppression of signaling in the myogenic and osteogenic pathways that are both detrimental to muscle and bone. 20 The effect of a simple increase in weight on bone density must be analyzed from various approaches. Moreover, it can be assumed that muscle mass gain may help improve BMD rather than just weight gain, and further research is needed to verify this.
The rate of change in BMD was not statistically significant between the 2 groups. No studies have been reported to monitor bone density changes between the 2 groups. The reason for these results may be that this study was conducted after the rapid decline in BMD. In other words, in the rapid decline period of BMD, the sarcopenia group decreases more rapidly than the non-sarcopenia group, and after that period, it may decrease to the same level between these 2 groups. 21 Another reason is that since the study was conducted only 1 year after surgery, it is necessary to observe the rate of change in a long-term follow-up period. Further studies are required focusing on the effects of these factors with long term follow-up, including patient groups during their perimenopausal period.
Several studies have reported that sarcopenia is related to poor clinical outcome. Steihaug et al 22 reported that hip fracture with sarcopenia was associated with having lower mobility at 1-year after surgery in a prospective, multicenter observational study. Sanchez-Rodriguez et al found that elderly patients with sarcopenia had worse functional status than those without sarcopenia prior to hospitalization to a subacute geriatric unit and upon discharge. 14 Chen et al 16 reported that sarcopenia may be an independent predictor of poor functional recovery and a decrease in life quality. Yoo et al 23 reported that with patients hip fracture aged ≥60 years with osteosarcopenia have a 1.8-fold higher 1-year mortality rate than patients without osteosarcopenia. Our findings also showed similar results to existing results. This means that the sarcopenia group outperforms the non-sarcopenia group in terms of functional state and postoperative recovery. Various factors, such as age, weight, nutritional status, and hormonal balance, may have affected these results, and it is necessary to identify the exact relationship through a forward-looking study.
To date, no studies have observed and reported changes in bone density in sarcopenia and non-sarcopenia groups. Since we investigated the BMD changes between the 2 groups, this study may contribute to identifying the critical timing or factors that affect bone density reduction. By further clarifying this relationship, risk factors can be identified early, and interventions, such as resisted physical training or nutritional intake, will help improve the prognosis. The adverse effects of aging can be minimized by identifying in advance when interventions are important. In addition, we minimize factors that can cause confusion in outcome analysis by targeting patients with the same surgical and rehabilitation protocols of hip arthroplasty in elderly patients.
There are several limitations in this study. Since this study period is only 1 year, it is likely that long-term postmenopausal studies will be needed, including those in the perimenopausal age group. In addition, whether osteoporosis is treated or not, treatment protocols were not equally controlled. Moreover, since it is a single-centered study, a multicentered research is warranted to add the number of patients.
Conclusion
Among elderly patients undergoing hip arthroplasty, the sarcopenia group showed lower BMD than the non-sarcopenia group, but there was no significant difference in the change in BMD between the 2 groups in a 1-year follow-up period. In addition, the sarcopenia group showed lower functional scores at all points studied except at the time of hospitalization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This research was supported by a grant from Wonkwang University in 2022.