
Abstract
Objective
This study evaluated the effectiveness, feasibility, and safety of early rehabilitation for patients after coronary artery bypass graft (CABG) surgery.
Methods
In a three-arm randomized controlled trial, patients who underwent CABG from January 2018 to June 2018 were randomly assigned to one of three groups: (i) usual care (UC group); (ii) UC + single general ward rehabilitation (SGR group); and (iii) UC + general ward rehabilitation and intensive care unit (ICU) rehabilitation (IGR group). The primary outcome was the Barthel Index scores.
Results
The Barthel Index score for UC (75.3 ± 12.1) was significantly lower than that of both SGR (86.2 ± 14.1) and IGR (89.1 ± 15.5). There was no significant difference in the Barthel Index scores between the SGR and IGR groups. Statistically significant differences were found in the length of ICU stay and post-operative hospital stay but not in post-operative pulmonary complications (PPC) or atrial fibrillation between the three groups.
Conclusion
Early rehabilitation implemented during ICU stay and on the general ward resulted in significant improvements in functional independence and could be a safe part of routine care post-CABG.
Keywords
Introduction
Coronary artery disease (CAD) continues to be a major cause of morbidity and mortality around the world 1 and is a growing problem in many countries. Coronary artery bypass grafting (CABG), the standard surgical treatment for CAD, is performed regularly. Patients undergoing CABG tend to be older and are more likely to have functional impairments; therefore, maintaining functional capacity during hospitalization is important. 2
Cardiac rehabilitation (CR) has been recommended for patients undergoing cardiac surgery, such as post-CABG surgery, valve repair or replacement, and cardiac transplantation, and CR has proven to be effective. 3 The timing of CR is divided into phase 1 (acute stage: within 7 days of onset), phase 2 (healing stage: from 1 week to 6 months after onset), and phase 3 (healed stage: >6 months after onset). 4 However, most evidence supports the beneficial effects of phases 2 and 3 CR. Studies regarding phase 1 CR are limited, and the results of the effects of early rehabilitation after CABG are conflicting.4–6 Early rehabilitation may increase the risk of coronary ischemia or inhibit wound healing. 7 Therefore, early CR is still controversial considering the risks 8 associated with intensive care unit (ICU) rehabilitation and the lack of adequate clinical research on its significance and effectiveness.
Functional independence is used to identify disabilities in activities of daily living in rehabilitation. Activities of daily living are considered a primary functional status measure in rehabilitation because of their relative objectivity, simplicity, and relevance to patients. Thus, the purpose of this three-arm randomized controlled trial was to evaluate the effectiveness, feasibility, and safety of early rehabilitation therapy in patients after CABG by evaluating functional independence.
Methods
The reporting of this study conforms to the CONSORT reporting guidelines. 9
Participants
This three-arm randomized controlled trial was conducted at the TEDA International Cardiovascular Hospital. The study protocol was approved by the TEDA International Cardiovascular Hospital Institutional Review Board (reference no.: 2018-0626-4; 24 August 2018), Tianjin, China. Informed written consent was obtained from all participants. The name of the registered trial is “Establishment of Clinical Rehabilitation Systems in the Peri-operative Period of Cardiac Surgery”, and the clinical trial number is ChiCTR1800018465.
Participants (aged ≥50 years) who underwent elective CABG for the first time between January 2018 and June 2018 at the TEDA International Cardiovascular Hospital were recruited. The exclusion criteria were: 1) exercise-induced syncope or ventricular arrhythmias; 2) inability to exercise and walk owing to comorbidities; 3) mechanical ventilation >24 h; 4) fraction of inspired oxygen >55%; and 5) new ischemic electrocardiographic changes. All operations were performed by the same surgical team.
This was a randomized controlled trial. Patients were randomized to one of three treatment groups following assessment of study eligibility and prior to initial physiotherapy assessment. Randomization was performed using cards within sequentially numbered, sealed, opaque envelopes. Group allocation was performed randomly (by shuffling the cards) by a research assistant whose contribution to the study went no further. Randomization was stratified by the patient's sex, age, and history of myocardial infarction before surgery. After applying the inclusion and exclusion criteria, the patients were allocated to a usual care group (UC), UC + single general ward rehabilitation group (SGR), or UC + general ward rehabilitation and intensive care unit group (IGR).
Intervention
UC: The UC group received group education. The main content of the education comprised awareness of the disease, the importance of risk factor management, and encouraging proper and gradual physical activity. Additionally, we distributed an incentive spirometer device to those who did not have contraindications after being admitted to the hospital, but we did not provide one-on-one guidance and supervision regarding the activities or training.
SGR: The SGR group received general ward rehabilitation with routine UC. General ward rehabilitation comprised respiratory exercises and daily walking exercises with increasing distances (Figure 1). Patients received the physiotherapeutic support protocol for 5 consecutive days after transferring to the general ward.

Protocol of the general ward rehabilitation therapy.
IGR: The IGR group received ICU rehabilitation (early CR) with UC + general ward rehabilitation. Early CR began the day after CABG, in the ICU. The specific procedures are shown in Figure 2. After beginning rehabilitation therapy, the patients continued therapy until they were transferred out of the ICU. Rehabilitation therapy was performed under the supervision of a professional CR therapist twice daily. Rehabilitation therapy was stopped if the patient met the termination criteria. The training was restarted from the first step when the patient was able. The rehabilitation training was terminated if the patient met any of the following conditions: 1) mean arterial blood pressure <65 mmHg or >110 mmHg; 2) heart rate <50 beats/minute or >120 beats/minute; 3) respiratory rate <12 breaths/minute or >40 breaths/minute; 4) pulse oximetry <88%; 5) feeling acutely unwell; and 6) the occurrence of adverse events, namely falling to the knees, tracheostomy tube removal, and prolapse of an indwelling catheter (such as an enteral feeding tube, urinary catheter, surgical drain, or an arterial or venous catheter).

Scheme of the intensive care unit rehabilitation therapy in this study.
Outcomes
The primary outcome measure for the study was activities of daily living. Questions pertaining to functional independence were formulated in accordance with the Barthel Index score 10 to ascertain the patients’ abilities to perform activities of daily living. The questions have been used and validated previously in post-cardiac surgery populations.11,12 Barthel Index assessments were performed three times: the day prior to surgery, upon transfer from the ICU to the general ward, and at discharge. All assessments were performed in a standardized order by one of three physiotherapists trained in assessment procedures.
Secondary outcomes were post-operative length of hospital stay, post-operative pulmonary complications (PPC), atrial fibrillation during hospitalization, and complications within 30 days after discharge (i.e., death, need for re-operation, atrial fibrillation, deep sternal infection, stroke, and re-admission to the hospital).13,14 The definition of PPC was in accordance with a study by Kroenke et al., 15 and this definition was also used in our previous study. 16
Statistical analysis
A previous study 17 showed that the mean difference and standard deviation between the Barthel Index score and the post-stroke group were 4.8 and 6.7, respectively. Accordingly, we preliminarily calculated the sample size by assuming an 80% probability to detect a clinically important difference in the Barthel Index score at hospital discharge at a significance level of 0.05 if the recruitment was 30 patients per group. All continuous variables were presented as mean ± standard deviation. Continuous variables in the IGR and SGR groups were compared separately with the UC group using a two-sided independent samples t-test. Frequency data were compared between the groups using the χ2 test. All results were considered significant at p < 0.05, and the statistical analyses were performed using SPSS software V.21.0 (IBM Corp., Armonk, NY, USA).
Results
A flowchart of the progression of patients through the study period is shown as Figure 3. In total, 156 patients who underwent CABG surgery were enrolled. Nine patients discontinued the CR because of pain, and seven patients declined testing at discharge owing to a lack of motivation. Of the remaining 140 patients, 46 patients were randomized to the UC group, 47 to the SGR group, and 47 to the IGR group. The patients’ baseline demographic and clinical characteristics are shown in Table 1. There were no significant differences between the three groups for the demographic and pre-operative variables.
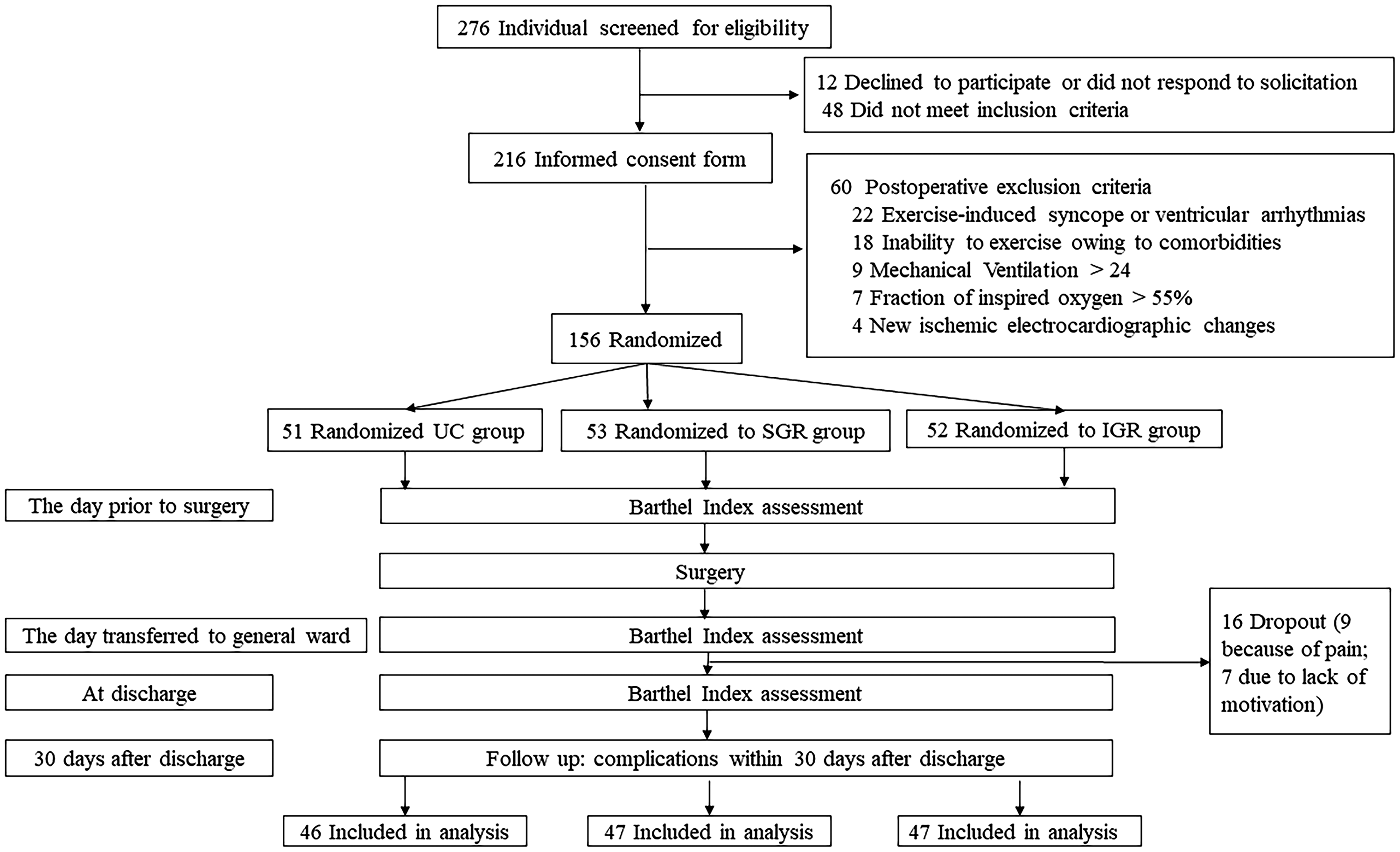
Flow diagram of patient enrollment and follow-up.
Participants’ baseline characteristics in each intervention group.

UC, usual care; SGR, single general ward rehabilitation; IGR, UC plus intensive care unit and general ward rehabilitation; NYHA, New York Heart Association.
No significant difference was found between the three groups for the patients’ basic characteristics.
Table 2 shows the outcomes measurement results in the groups throughout the study. Pairwise comparisons indicated that the Barthel Index scores for the UC group were significantly lower than those for both the SGR group and IGR group at discharge. There was no significant difference in Barthel Index scores between the SGR group and IGR group at discharge. However, the Barthel Index scores for the IGR group were significantly higher than those of the SGR group and the UC group when patients were transferred to the general ward (Figure 4). There were no significant differences between the three groups for PPC and atrial fibrillation in-hospital (Table 2); however, patients in both the SGR group and IGR group experienced significantly fewer complications at 30 days compared with the number of complications in the UC group (p < 0.05). The lengths of ICU stay and post-operative hospital stay for the IGR group were statistically shorter compared with the UC group and SGR group (p < 0.05) (Table 2).
The outcomes measurement results in the three groups.

UC, usual care; SGR, single general ward rehabilitation; IGR, UC plus intensive care unit and general ward rehabilitation.
p1: p-value of the SGR group vs. the UC group; p2: p-value of the IGR group vs. the UC group; p3: p-value of the IGR group vs. the SGR group.

Barthel Index scores at different time points (*p < 0.05, denotes significantly different from the usual care group; #p < 0.05, denotes significantly different from the SGR group).
One patient in the IGR group required intra-operative insertion of an intra-aortic balloon pump to treat poor left ventricular function. Two patients (one in the UC group and one in the IGR group) required sternal re-opening on the first post-operative day for hemostasis. Four patients, two each in the SGR group and IGR group required insertion of an intercostal catheter(s) for the management of pneumothorax and/or pleural effusion. The events in five of the above seven patients occurred before the rehabilitation intervention, and two events occurred after the rehabilitation intervention and consisted of pleural drainage to address pleural effusion 3 to 4 days after the operation. However, the imaging data showed that both patients requiring plural drainage had varying degrees of pleural effusion post-operatively on the day of the operation. Other than occasional and transient high blood pressure and rapid heart rate, the rehabilitation process did not cause other adverse effects, such as the loss of tubing, malignant arrhythmia, or falls. Ten patients re-presented to hospital following discharge, two of whom remained in hospital until the planned follow-up date (specifically, for investigation and management of transient ischemic attack (SGR group) and pericardial effusion (IGR group)). Of the other eight patients, two patients were from the UC group; one with pulmonary emboli and one with a bleeding duodenal ulcer. Four of the 10 patients were from the SGR group; one each presented with chest pain/malaise, radial artery graft site infection, gouty arthritis, and atrial fibrillation. The remaining two patients were from the IGR group; one with collapse/fall of unknown reason and one with gastrointestinal bleeding.
Discussion
The principal finding in the present study is that in a population of patients undergoing first-time, non-emergency CABG, an early CR program performed under direct physiotherapy supervision resulted in higher values for functional independence (as measured by the Barthel Index) before discharge from hospital compared with patients not receiving early CR. Early rehabilitation may explain the higher values; however, a study comparing mean differences between baseline and follow-up measurements is needed for confirmation.
The ability of CR to improve functional capacity in patients has been consistently demonstrated.18,19 Similarly, the results of the current study showed that patients receiving comprehensive CR clearly had better performance of their activities of daily living after discharge. In addition, patients who received early rehabilitation in the ICU had better self-care ability (higher Barthel Index score) immediately after transfer to the general ward, and they were able to reach basic self-care status quickly as the rehabilitation process progressed. It is interesting that the differences in functional independence measured by the Barthel Index scores between the SGR and IGR groups gradually declined over time. This suggests that regardless of whether patients received early rehabilitation in the ICU, patients tended to have the same level of functional independence at discharge following successful CABG. Although the value of the functional independence achieved by the patients receiving early rehabilitation in the ICU was evaluated only short-term in this study, early rehabilitation in the ICU has considerable economic and social benefits. The patients undergoing early rehabilitation were able to achieve basic self-care within 3 to 4 days after surgery, in this study; therefore, early rehabilitation reduced the economic costs of care for families and reduced the required degree of nursing care. The long-term impact of early rehabilitation in the ICU and specific ward-based rehabilitation may not be easy to determine, and more research is needed.
This study showed that adding additional ICU-based rehabilitation after CABG benefitted patients regarding the ICU stay and the hospital stay. In 2012, a Japanese study also found that early CR in the ICU for elderly patients could be an effective tool to significantly shorten the durations of hospital stay and ICU stay. 20 Shorter ICU stay and hospital stay have significant impacts on healthcare costs. Cardiovascular disease and cardiac surgery, in particular, are associated with large expenditures of healthcare resources. The European Respiratory Society and the European Society of Intensive Care Medicine advise starting early active and passive exercise in critically ill patients. 21 Recent literature suggests that it is possible to conduct early mobility therapy in the ICU,22,23 and early rehabilitation in the ICU prevented the neuromuscular complications associated with critical illness and improved the patients’ functional status.24,25 While patients after CABG surgery generally do not remain in the ICU for long periods (the average ICU stay in this study was 48 hours), our results fully demonstrated the importance, feasibility, and safety of early rehabilitation in the ICU.
To date, research in early rehabilitation has generally been confined to the investigation of the effect of CR in the ICU on short-term functional outcomes at transfer out of the ICU or at hospital discharge. Thus, future randomized controlled trials are advocated to evaluate the effect of CR on long-term outcomes.
The results of our study did not show a significant difference in PPC incidence between groups, which was similar to the findings in Manapunsopee et al.’s study. 26 The reason for this lack of difference might be the small sample size and insufficient power, or the pre-operatively-issued free incentive spirometer device and education. As Boden et al. showed, pre-operative education about breathing exercises could halve the incidence of PPCs in post-abdominal surgery. 27
There are some limitations in this study. First, the sample for this study was small and this limits the external validity of our findings. The primary limitation in the study was the inability to blind the outcome assessors to group allocation. However, we believe that this had minimal impact on the results of the study owing to the stringent assessment procedures that we used, which allowed for no assessor subjectivity or encouragement. Second, the activities of daily living (measured by the Barthel Index score) could not completely reflect physical function. To address this, we also evaluated the 6-minute walk distance (6-MWD) on the day of hospital discharge between the groups (minimum clinically important difference between the groups: 25 m, standard deviation: 32 m), and found similar results to those obtained with the Barthel Index scores. However, the 6-MWD elicits a maximal to submaximal exercise response that can progress to mild heart failure and may induce symptomatic angina, severe dyspnea, and dizziness before CABG. Considering the patients’ safety, we performed the 6-MWD test only after CABG for all patients, which meant that we had no baseline evaluation. Therefore, the results of the 6-MWD test were for reference only. Third, we investigated the outcomes only during hospitalization. Long-term follow-up is required to further investigate the effects of early rehabilitation therapy on clinical outcomes after patients leave the hospital. Finally, early rehabilitation may also influence other clinical indices, such as oxygen index, tidal volume upon spontaneous breathing, and C-reactive protein.
In conclusion, from the analysis of our data, we suggest that early rehabilitation implemented during the ICU stay and on the general ward results in significant improvements in functional independence and could be a safe part of routine care post-CABG.
Footnotes
Acknowledgements
The authors thank all the members of the Department of Rehabilitation Medicine for their generous technical assistance and guidance, and the nursing team led by the Department of Surgery for their technical support. We also thank all the study participants for their kind participation and cooperation.
Author contributions
Peipei Han and Hairui Yu wrote the manuscript. Qi Guo, Xiaocheng Liu, and Zhigang Liu conceived and designed the research. Fandi Xie and Xiaoyu Chen analyzed the data. Xing Yu, Jing Li, Xiangjing Liu, Bohan Shao, Yaping Liu, and Jianjun Liu performed the bulk of the research. Ming Li provided constructive comments during the review process.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded by the Shanghai Sailing Program (grant number: 20YF1418200), Scientific Research Foundation of SUMHS (SSF-21-03-007), and the Wu Jieping Medical Foundation (grant number: 320.6750.17073).