
Abstract
Introduction
This focused review examines the use and effectiveness of self-management strategies in preventing or managing pain, which is among the most common secondary conditions faced by individuals with a mobility disability.
Methods
This focused review was part of a two-phase comprehensive scoping review. Phase I was a comprehensive scoping review of the literature targeting multiple outcomes of self-management interventions for those with mobility impairment, and Phase II was a focused review of the literature on self-management interventions that target pain as a primary or secondary outcome. Two authors searched CINAHL, PubMed, and PsyclNFO for papers published from January 1988 through August 2014 using specified search terms. Following the scoping review, the authors independently screened and selected the studies and reviewed the eligible studies, and the first author extracted data from the included studies.
Results
The scoping review yielded 40 studies that addressed pain self-management interventions for those living with mobility impairment. These 40 accumulated papers revealed a heterogeneous evidence base in terms of setting (clinic, community, and online), target populations, intervention duration (3 weeks to 24 months), and mode (health-care providers and lay leaders). Most of the reviewed studies reported that the self-management intervention led to significant reduction of pain over time, suggesting that self-management may be a promising approach for addressing pain experienced by people who live with mobility limitations.
Discussion
This review also reveals moderate-to-high bias across studies, and findings indicate that future research should enhance the methodological quality to provide stronger evidence about the effectiveness of self-management strategies for reducing pain among those with mobility impairments.
Introduction
In the midst of the shifting paradigm in disability that has allowed us to conceptualize people with disabilities as able to achieve health,1,2 substantial attention has focused on secondary conditions. This notion, first coined by Marge, 3 recognized that people living with primary disabilities (eg, paralysis due to spinal cord injury) often experienced health problems secondary to their disability (eg, pressure sores), but that most were preventable. Yet, 25 years later, people with disabilities continue to experience high rates of secondary conditions.4,5 In addition, there is growing evidence that prevalence of chronic conditions (eg, heart disease, cancer, diabetes, and hypertension) is significantly higher among individuals with a disability than individuals without.6,7 Due to the increasing evidence that having a disability increases an individual's risk of experiencing poor health, there is a growing recognition of the need for health promotion efforts.2,8,9
In the general population, rates of chronic conditions such as arthritis, diabetes, and asthma have steadily risen,10–12 which has led to efforts targeting patient self-management of disease. Dr. Katie Lorig at Stanford was among the first to develop a layled self-management program for people living with arthritis, which yielded successful outcomes related to increasing patient knowledge, health behaviors, and health status. 13 While a consistent definition of self-management has not been established, Barlow's definition encapsulates the complexity of the approach,
“Self-management refers to the individual's ability to manage the symptoms, treatment, physical and psychosocial consequences and life style changes inherent in living with a chronic condition. Efficacious self-management encompasses ability to monitor one's condition and to effect the cognitive, behavioral and emotional responses necessary to maintain a satisfactory quality of life. Thus, a dynamic and continuous process of self-regulation is established.” 14 (p. 178)
With an evolving health-care system and the growing number of individuals living with a disability, implementing evidence-based self-management approaches for individuals with complex medical conditions, including those with a disability, is becoming increasingly important. This is especially pertinent as individuals spend limited time (on average 12.8-18.3 minutes) with their health-care provider and yet need to have the knowledge and skills to manage their symptoms, make healthy lifestyle changes, and take medication.15–18
Substantial heterogeneity exists within disability, including age and manner of onset (eg, congenital, disease, traumatic injury, and age-related), body system(s) affected (eg, sensory, physical, cognitive, and emotional), severity, and impairment status (eg, stable, episodic, and progressive). Yet, US disability estimates consistently show that limitations involving walking/climbing are the most common.19–21 Notably, while having a disability increases one's risk for secondary health problems, recent evidence about the prevalence and incidence of these health issues indicate that they are highest among individuals living with mobility limitations. 4 People living with mobility impairments are at increased risk for an array of secondary health problems, 4 yet six commonly experienced secondary conditions among people with mobility limitations include chronic pain, chronic fatigue, depression/mental health, urinary tract infection, bladder/bowel problems, and pressure ulcer/sore.22–24 The purpose of this paper is to provide a focused review of the literature examining self-management programs designed to prevent or manage pain, one of the leading secondary conditions experienced by individuals with mobility impairment.
Methods
Definitions
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 25 guided the process for conducting this focused review of the literature. We defined the population of interest and identified search terms before searching online databases for relevant papers. Populations of interest for this search included those who experience a health condition (from birth, disease, or injury) that impairs mobility. This focused review on pain self-management was part of a comprehensive scoping review of the literature that consisted of two phases. Phase I was a scoping review of the literature that targeted multiple outcomes of self-management programs for those with mobility impairments, and Phase II specifically targeted reviewing literature focused on self-management programs that target chronic pain as either a primary or a secondary outcome. Thus, Phase I of the scoping review targeted locating published literature examining the effect of using self-management strategies to reduce or manage secondary conditions commonly experienced by individuals with disabilities. This scoping review of the literature included publications that addressed any one of the six most commonly experienced secondary conditions among people with mobility limitations, which included chronic pain, chronic fatigue, depression/mental health, urinary tract infection, bladder/ bowel problems, and pressure ulcer/sore.22–24 Interventions included in the scoping review covered programs that taught self-management or self-control skills to prevent or manage at least one of the six identified secondary conditions.
The authors established inclusion and exclusion criteria for retaining or eliminating publications for the focused review. The inclusion criteria were (1) the publication included results of intervention outcomes on at least one of the six identified secondary conditions; (2) >50% of the sample experienced a mobility impairment, or an impairment such as arthritis or back pain that can impair mobility, even if the authors did not comment on the participants’ mobility status; (3) enrolled participants who experienced mobility impairment ≥6 months, or the mean time with disability was ≥6 months for the full sample; (4) included the targeted age range, as long as the study did not predominantly focus on age-related disability, and the sample mean age was < 65 years old; (5) explicitly included one of the identified secondary conditions, even if it was a secondary outcome; (6) conducted an intervention to assess the effects of a self-management intervention; and (7) the paper presented the main effects of the self-management intervention on outcomes of primary interest (eg, numeric or text results of clinical or statistical significance, which includes P-value or effect size). The intent of this review was to examine the effectiveness of using self-management approaches to reduce chronic pain for adults living with permanent mobility impairment, and exclusion criteria were developed to assure that the subset of papers reviewed would target these groups. Thus, criteria were developed to assure that the studies represented adult samples without explicit aging-related mobility impairment, with diagnoses likely to result in permanent mobility problems. As self-management programs may either be structured differently or have different effects for people with cognitive impairments, we developed criteria to eliminate studies with samples whose diagnoses were likely to yield cognitive problems (eg, brain injury). Criteria set for excluding papers from review were as follows: (1) sample targeted < 18 or >65 years old; (2) sample had cognitive or psychiatric impairment (eg, traumatic brain injury, bipolar, and intellectual disability); (3) sample experienced neck pain, or arthritis predominantly in the hand; (4) sample experienced a time-limited event that causes disability (eg, pregnancy); or (5) study was cross-sectional (correlational study) or a case study.
Literature search
The literature search was completed in September 2014 using the search engines CINAHL, PubMed, and PsycINFO for papers published from January 1988 through August 2014. The authors used the following terms and included the truncation algorithm to search indexed databases: disability (disability*), physical disability (disability*), mobility impairment, self-management, self-care, self-regulation, lifestyle, self-control, secondary conditions, urinary tract infection, bladder/bowel problems, pain, chronic pain, fatigue, depression, and mental health. In addition, we supplemented the search of indexed databases by manually examining the reference lists of literature identified through the electronic search.
Figure 1 depicts results from the process of identifying and selecting papers for this review. Our scoping review yielded 5,068 citations, which after removing duplicates (2,624) and those that fell outside our criteria (1,244 irrelevant) left 1,200 citations for review. The review process began with establishing interrater agreement among the three study authors in identifying citations to retain for full review. The authors independently reviewed the titles/abstracts of a randomly selected 20% of the 1,200 citations, and then discussed issues for those citations with initially discordant ratings until consensus was reached. The remaining 940 citations were equally divided in a random fashion among the three authors to select citations for full review, and this consensus process was used for every citation that did not clearly fall within the established criteria. This led to selecting 109 citations for a full-text review and identifying 50 studies that met our inclusion/exclusion criteria.
These 50 papers were organized according to the secondary conditions measured across the self-management interventions. Organizing in this manner revealed that the published literature addressed only three of the six identified secondary conditions, namely, pain, depression, and/or fatigue. Yet, 22 studies targeted multiple outcomes (eg, pain and depression). Due to the large number and heterogeneity of included studies, this focused review is limited to 40 studies that targeted pain as an outcome. Then, the first author completed a standardized abstraction form for all 40 retained papers to report elements of study design, sample size, population characteristics, intervention strategies, duration, and between-group and within-group outcomes. Separate focused reviews will be published for papers that addressed outcomes of depression/mental health and fatigue.

PRISMA flow diagram.
Review of study bias
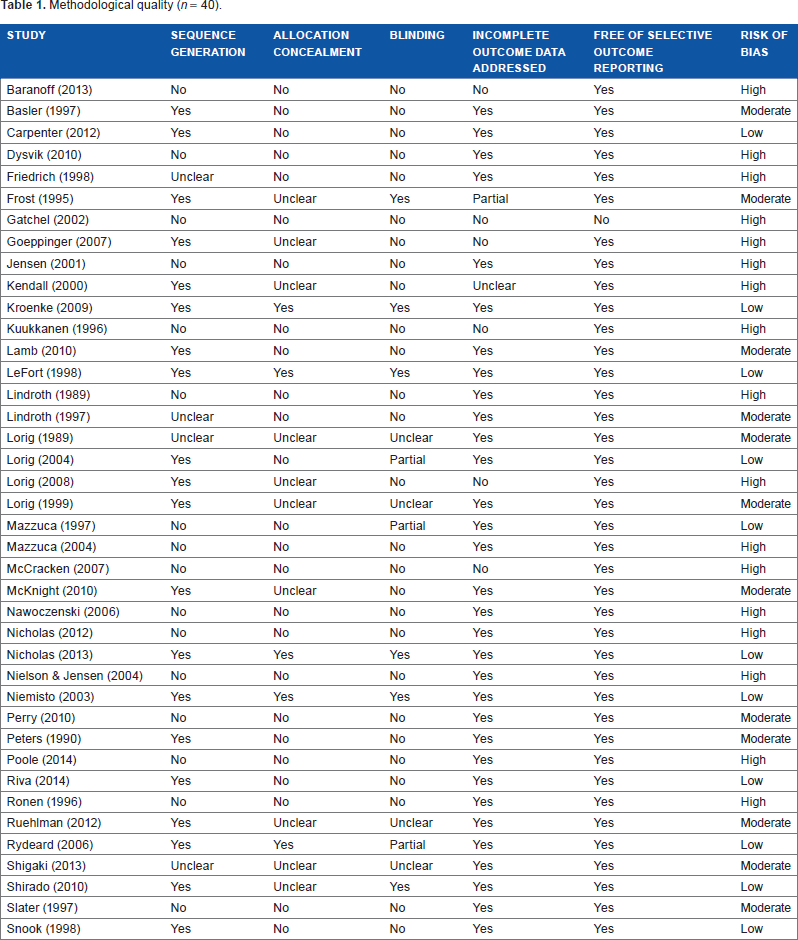
We assessed risk of bias using the Cochrane Risk of Bias Tool. 26 Risk of bias was completed for each study by considering the following five factors: sequence generation, allocation concealment, blinding, incomplete outcome data assessed, and free of selective outcome reporting. If all criteria were met, the study was considered to have low risk of bias. Where one or more criteria were partially met, the study was deemed to have a moderate risk of bias, and studies with two or more were classified as high risk.
Results
Study bias
Based on the Cochrane grading criteria, 72.5% of the studies were considered to have moderate-to-high bias (Table 1). The two most common areas of concern related to bias were the absence of blinding and concealing allocation. Yet, many studies lacked sufficient detail to ascertain one or more features in determining quality.
Participants
Forty studies included in the review represent participants with various diagnoses for which pain is a common secondary condition. Table 2 provides a snapshot related to the diagnostic groups studied, research designs used, participants enrolled, and data regarding their age, gender, and race. Over half (n = 22, 55%) of the included studies targeted individuals with chronic low back pain or musculoskeletal pain, yet more participants with arthritis or other connective tissue disorders were enrolled across the 15 studies. The type of pain participants experienced is best characterized as musculoskeletal pain. About two-thirds of the studies were randomized controlled trials (RCTs), and the total sample across the studies included 8,831 participants. The studies tended to enroll middle-aged (average 51.31 ± 5.51 years old) women (69.4%). Although women experience higher arthritis prevalence at all ages than men, 11 the discrepancy in arthritis prevalence between men and women is not that large. However, US estimates indicate that two-thirds of those who report experiencing activity limitations due to arthritis are women. 27 Younger males were better represented in studies that enrolled individuals with mobility impairments due to diagnoses such as spinal cord injury and chronic low back pain. Race was reported in less than half (48%) of the studies. Among the studies that did report race, whites comprised the vast majority (83%) of the samples. Yet, three studies included in this review were designed to target minority groups.28–30
Methodological quality (n = 40).
Settings
The review includes studies predominantly conducted in North America (n = 21, includes the US and Canada), many studies conducted in Europe (n = 7, counting Israel as in Europe) or Nordic countries (n = 5), several studies conducted in Australia or New Zealand (n = 6), and one study conducted in Asia. Interventions were delivered in an inpatient rehabilitation center, 31 15 were provided in clinical settings, including hospital-based outpatient clinics,32–44 one combined delivering the intervention in a clinical setting with a transition to home,30,45,46 several were in the community (mail or small group)28,29,47–51 including the home,52,53 and six were offered via the Internet.54–59 Notably, many clinic-based studies had a multidisciplinary team of physicians, nurses, physical therapists, and psychologists delivering the intervention. Approaches included promoting exercise in group-based settings with two studies that compared exercise approaches 60 and one combined education with exercise. 61
Intervention
Intervention programs generally focused on educating participants about using cognitive-behavioral strategies to manage pain. The programs typically combined cognitive (eg, desensitization, cognitive restructuring, pain management, and problem solving), behavioral (eg, goal setting, relapse prevention, stress management, relaxation, increasing self-efficacy, and social support),32,33 and physical components (eg, strengthening specific muscles, encouraging exercise to reduce pain, and teaching body mechanics) 62 to address self-management. Investigators implemented various modes of delivery, including individualized, 62 small group, or online/telephonically. Many interventions were relatively brief, ranging in duration from 3 to 4 weeks,30,31,34–36,38,39,61,63,64 6 to 10 weeks,29,40–42,46–48,53,55–57,65–67 and one was 18 weeks. 38 Several studies delivered longer interventions, including two studies that recommended participants to engage in behavior change for 6 months,53,68 and three studies that provided ongoing intervention for 12 months,37,49,52 and one study lasted for 24 months. 43
In terms of the theoretical underpinnings used in these studies, several studies explicitly stated using cognitive-behavioral approaches to address behavior change,35,38–40,47,50,56,63 and two studies37,66 formally addressed incorporating two primary theoretical frameworks, including social cognitive theory29,37,48,49,57,67 and social learning theory. 59 In addition, one research group has hypothesized that the transtheoretical model plays a role in program adherence and outcomes in pain management. 44
Outcome measures
There was substantial variability regarding the aspects of pain assessed and the specific measures used. Pain intensity was often measured, but other aspects of pain included pain interference, pain symptoms, pain severity, pain catastrophizing, pain acceptance, pain self-efficacy, pain stages of change, and pain locus of control. A visual analog scale was commonly used to assess pain intensity. Other pain instruments included the Brief Pain Inventory, Multidimensional Pain Inventory, Arthritis Impact Measurement Scales, McGill Pain Questionnaire, SF-36 pain subscale, Western Ontario and McMaster Universities Osteoarthritic Index (WOMAC), and the Wheelchair User's Shoulder Pain Index.
Summary of 40 studies regarding the diagnoses, research design, number of participants studied, and their mean ages.

Averages and proportions weighted by sample sizes of the studies.
Results
The reviewed studies can be grouped into five broad categories, based on the type of intervention delivered. Self-management intervention approaches represent those that were delivered (1) as in-person classes in clinical settings, (2) as in-person classes in the community, (3) as mixed in-person sessions in the clinic with a transition to home, (4) in combination with exercise programming, and (5) online. This section presents results separately for these broad categories. Detailed information for all 40 reviewed studies is located in Table 3.
Self-management programs delivered in clinical settings
Of the 15 studies delivered in clinical settings, 13 (85%) reported that the self-management program resulted in significantly reduced pain. Among the nine RCTs or quasi-experimental designs, groups receiving self-management training had significantly greater reductions in pain than the groups receiving usual care37,50 or compared with a control group.42,65 Several studies also compared effects of the self-management program with other active intervention arms. Lamb et al 51 reported that the use of cognitive-behavioral therapy (CBT) was more effective in reducing pain than active management alone and that combining active management with CBT had greater benefits than CBT only. Peters and Large 40 demonstrated that teaching self-management strategies was more effective than usual care within both inpatient and outpatient settings. However, Nicholas et al 39 reported that combining CBT with teaching participants’ techniques either to distract themselves from pain or to expose themselves to pain both yielded significantly less pain. Furthermore, all six studies that used a single-group, pretest-posttest design reported that the self-management program led to significantly reduced pain over time. Notably, these intensive interventions were delivered by a multidisciplinary team35,44,69,70 during intensive 90-minute or five to eight hours/day sessions over three weeks,32,35,38,44,69,70 with one delivered over 12 weeks.
Program adherence was only reported in two (13%) studies,38,39 which were conducted by the same research group and measured participants adherence using the five to seven self-management strategies taught (activity pacing, using a flare-up plan, stretch exercises, desensitizing, thought challenging, fitness exercises, goal setting). Both also examined outcomes based upon adherence to using these strategies and, as hypothesized, use of more strategies was associated with greater improvements in pain. Notably, the investigators directly observed patients use of these strategies as these studies were conducted within inpatient and all-day outpatient settings. Attrition was reported in 13 studies (87%) with an average retention rate of 81%, and four conducted intent-to-treat analyses.37,41,47,51
Study summary.

Seven (47%) clinic-based studies reported effect sizes, with data indicating that changes in participants’ pain ratings were generally small to medium (-0.33 to -0.54), while effect sizes for accepting or coping with pain were medium to large (0.62-1.3). However, a 10-session, group-based CBT program that included 45 contact hours reported a large effect size (1.0) for usual pain ratings by those with spinal cord injury. 33 In this comparative parallel design study, Perry et al enrolled 36 participants all of whom were receiving care at a pain clinic, including 92% who experienced neuropathic pain. The study did not randomly allocate participants to groups, and significant differences in usual pain intensity existed at baseline between the self-management and usual-care groups, with the self-management group experiencing significantly greater pain. Notably, effect sizes are based on the final sample size of 13 people retained in the study at the final assessment by nine months. Thus, while the effect size on usual pain intensity was large, the small sample size may be biased as it includes both those with higher pain and who, for whatever reason, valued the intervention.
Self-management programs delivered in community settings
This section describes the results of five studies conducted in community-based settings. All the community-based studies compared the self-management approach with another arm using RCT designs, and most (n = 4, 80%) reported significant effects of the self-management program on pain outcomes. Three (60%) studies with a comparison arm reported a significant between-group effect,28,29,47 while two studies did not report significant between-group effects for reduced pain.48,49 A mailed self-management program was not significantly better than sessions delivered in person or usual care. 49 Delivering reinforcement strategies using newsletters or in-person sessions eight months after the self-management intervention was no more effective in reducing pain than doing nothing. 48 Notably, while Goeppinger et al 28 reported significant between-group effects for pain outcomes, the study compared two self-management programs, namely, the Arthritis Self-Help Course (ASHC) and Chronic Disease Self-Management Program (CDSMP). The authors examined the effectiveness of incorporating cultural adaptations to the ASHC and the CDSMP for a predominantly (82%) African-American sample and reported 4- and 12-month outcomes for the entire group and separately for African-Americans. By four months, for both the entire sample and African-Americans, CDSMP participants reported significantly less pain than ASHC participants, yet these changes were not sustained at one year. These results suggest that only one of these two culturally adapted self-management programs resulted in significant reductions for pain. However, it is worth noting that both self-management programs yielded significant four-month changes on other measured outcomes.
Four (80%) of the community-based studies reported on program adherence. Goeppinger et al 28 and LeFort 71 reported participants attending between 72% (M = 4.3/6) and 82% (M = 4.9/6) of sessions of a six-week program. Yet, Lorig and Holman 48 reported that only 24% of people randomized to attend a six-week course designed to reinforce self-management strategies eight months after the initial intervention attended the sessions. In a separate study conducted by Lorig et al 49 that compared a mail-delivered, tailored print self-management (SMART) program to usual care and a six-session group-based arthritis self-management program, the average number of mailings participants completed was three out of a possible four, which includes 11% of SMART participants who never participated. This 75% participation rate is similar to that of the studies by Goeppinger et al 28 and LeFort. 47 The average retention rate reported across all five community-based studies was 85%, which is notable given that four were conducted over a year or longer and only one conducted intent-to-treat analyses. 47 Yet, none of the classes delivered in community-based settings reported effect sizes.
Self-management delivered in a mixed clinical/community settings
Three studies provided initial training in the clinical setting and transitioned ongoing program delivery to the home, with significant effects only reported by one. In two separate studies, Mazzuca et al30,45 initially offered individualized training by a nurse educator in the clinic who provided telephone follow-up to reinforce self-care activities twice (at one and four weeks) in one study 30 and up to nine times (biweekly for 18 weeks) in the other. 45 The programs yielded no significant between-group effects on pain at posttest or six-month follow-up, but one study observed significant differences in pain by 12 months. Ronen et al 46 combined clinical and community settings so that participants received eight weeks of rehabilitation in a multidisciplinary setting before transitioning to continue using self-management strategies at home. While there was no control group, participants reported significantly reduced pain at eight weeks and one year. The study by Ronen et al was the only one to report on participants’ adherence during the home-based phase of principles taught (range 32%-82%) and continued exercise (60%). It is important to note that the authors do not address attrition and only present data for the 60 participants who fully completed the program at one year. However, the average retention reported by two other studies was 75%.30,45 As the only study to report on effect sizes, Ronen et al reported that the intervention yielded large effects (-1.19) on pain at the eight-week posttest and moderate effects (-0.50) one year later.
Self-management programs combined with exercise
All the 11 studies that examined self-management programs that formally incorporated exercise reported a significant improvement in pain over time. Yet, as described below, two studies that compared the effects of multiple strategies found that all the strategies resulted in significantly reduced pain over time with no difference between groups. For example, Kuukkanen and Malkia 60 found no difference between participants in an exercise program, an intensive exercise training (eg, supervised sessions, special equipment), or a control group that received usual care. In addition, McKnight et al 43 found no differences in pain between those given a strength program, a self-management program, and a combined strength and self-management program. However, effect size data indicate that while all groups reported improved pain, the combined self-management with strength training group experienced larger effects (-0.70) than either the self-management (–-0.59) or strength training (0.24) group. Notably, this was the only study to report on effect sizes.
The six studies (55%) that reported in some manner on participants’ compliance with the intervention components reveal compliance rates of 67.5%-100%. Compliance was high for attending in-person exercise sessions (86%-91%);34,61 self-management classes (75%), supervised strength training (75%), or the combined classes (72%); 43 completing clinic visits (100%); 64 or self-reporting home exercise compliance (75% were highly adherent); 62 or following restrictions for movement in the morning for 58 minutes. 53 Most studies (91%) reported on attrition, and one study that enrolled only 39 participants retained only 42% by the end of the year, 64 in which the authors used an intent-to-treat analysis using the last observation carried forward approach. The average retention rate across studies was 81%, with six reporting outcomes for up to a year and three reporting outcomes over one and a half years to two and a half years. The high retention is notable given that most lasted a year (n = 6) and several (n = 3) continued for over one and a half years to two and a half years. Although retention was generally high, only two studies62,64 implemented intent-to-treat analyses.
Online self-management programs
Six studies examined the effect of delivering self-management intervention over the Internet. Three (50%) yielded significantly reduced pain and a fourth reported that the Internet program yielded significant changes in other aspects of pain, including pain attitudes and pain catastrophizing. Only two studies reported about adherence. While Lorig et al 57 used website analytics to report that participants logged into the website an average of 31.6 ± 24.5 times over six weeks, Carpenter et al 63 found that 81% of the group reported completing all six online chapters. All six studies reported on participant attrition, with an average retention rate of 85% across the studies. Two studies used an intent-to-treat approach to address attrition. Effect sizes reported across five studies suggest that these effects were small to moderate (ranged from –-0.31 to –-0.57) for pain, with a large effect size of 1.01 reported for pain control in one study. 63
Discussion
This review of the published literature reveals a burgeoning evidence base that has examined the effect of self-management interventions on reducing and managing pain among individuals living with mobility-related disabling conditions. The published evidence reveals substantial heterogeneity in terms of targeted diagnostic groups (eg, chronic low back and other locations, arthritis, other connective tissue diseases, and neurologic disorders), settings (eg, clinic, community, home, and Internet), approaches (eg, intensive multidisciplinary training, combining exercise with CBT, etc.), and countries (eg, US and Canada, Europe, Nordic countries, and Japan). Nevertheless, the collective body of evidence suggests that delivering self-management training often, but not always, yields significant, but small, improvements in participants’ self-reported pain.
This review suggests that educating individuals about their symptoms and using both cognitive and behavioral approaches that emphasize applying self-management strategies to manage symptoms and make lifestyle changes can produce positive outcomes on participants’ self-reported pain. These effects have been achieved through teaching skills in both clinical and community settings, through combining self-management strategies with exercise programs, as well as using an online format. While two studies38,39 reported that better outcomes are related to participants’ use of self-management skills, only 15 (38%) reviewed studies reported on participants’ adherence with the program delivery or components. Although no single approach emerged as clearly more efficacious than others, it is important to highlight that retention has been high not only in clinic-based studies (81%) but also in community-based (85%) studies and for online settings (85%).
Several shortcomings of the literature are noteworthy. An important limitation is that 70.7% of reviewed studies have moderate-to-high risk of bias, predominantly due to the lack of blinding and concealing participant allocation to groups. While it is feasible to blind testers to participant group assignment in studies that teach self-management skills, it is not possible to blind participants. Yet, this inability to mask participants can introduce response bias, especially when assessing subjective outcomes such as pain. Thus, it is possible that at least some of the observed effects on pain are due to this response bias. A second shortcoming is based on the lack of consistency across measures for specific outcomes of interest. Researchers used an array of outcome measures for pain (eg, visual analog scale, Oswestry Low Back Pain Index, McGill Pain Questionnaire, Modified von Korff Scale, SF-36 bodily pain, Brief Pain Inventory, etc.), which limits the ability to provide direct comparison across studies. Notably most outcome measures used across these studies were given at a single time point to reflect participants’ outcome across a specified period (right now [McGill Pain Inventory], last 24 hours [Brief Fatigue Inventory], last week [Brief Pain Inventory], or last 4 weeks [SF-36]). Only two reviewed studies53,61 used daily pain diaries to capture fluctuations in pain over the course of the day. Evidence suggests that individuals’ recall of pain intensity over longer periods is higher than observed on momentary reports.72,73 A third limitation is the fact that studies generally did not measure participants’ adherence to the intervention components, and thus, it is unclear whether the dose received is related to the effect on the outcome. A final shortcoming is that despite substantial heterogeneity across studies in terms of settings, modes of delivery, duration, and intensity, the evidence lacks racial/ethnic diversity as the vast majority of studies have been conducted among Caucasian and female samples. Yet, two studies demonstrated that making culturally appropriate adaptations to self-management programs yielded significantly improved outcomes.28,29
To summarize, this focused review offers evidence that self-management approaches have successfully been used to reduce pain among individuals living with mobility limitations. While effect sizes were reported in only 40% (n = 16) of the studies, the programs generally yielded small effects on participant pain ratings, although moderate-to-large effects were reported for coping with pain. Of promise is the potential for using the Internet to deliver self-management intervention, as many individuals who live with disabilities face persistent transportation barriers, which can limit attendance for in-person educational meetings. These interventions resulted in significantly improved pain as compared with usual care groups in several studies and across time in others, with similar albeit small effect sizes as reported by clinic-based studies.
Yet, the review reveals that the accumulated studies have moderate-to-high risk of bias, generally due to the lack of allocation concealment and blinding, which may particularly influence subjective outcomes. Nevertheless, it is important to examine intervention approaches that offer potential strategies for reducing pain given its prevalence and impact on the lives of individuals living with mobility impairments. Future studies should increase the methodological rigor to yield stronger evidence about the effectiveness of self-management strategies for reducing pain among those with mobility impairments. Recommendations for future studies include (1) using a control group with no intervention or minimal intervention to increase power to detect treatment effects, (2) using technology such as cell phones to assess pain in real time over multiple times during the day rather than relying on single point in time assessments that reflect a brief, specified time period to determine intervention effects on pain, (3) measuring adherence to the intervention to determine whether there are dose-response relationships, and (4) having authors present effect sizes.
Author Contributions
Conceived and designed the experiments: KFG, SJD, KDS. Analyzed the data: KFG, SJD, KDS. Wrote the first draft of the manuscript: KFG. Contributed to the writing of the manuscript: KFG, SJD, KDS. Agree with manuscript results and conclusions: KFG, SJD, KDS. Jointly developed the structure and arguments for the paper: KFG, SJD, KDS. Made critical revisions and approved final version: KFG, SJD, KDS. All authors reviewed and approved of the final manuscript.