
Abstract
Study Design:
Retrospective review of a prospectively collected database.
Objective:
To predict the occurrence of hospital-acquired conditions (HACs) 30-days postoperatively and to compare predictors of HACs for spine surgery with other common elective surgeries.
Methods:
Patients ≥18 years undergoing elective spine surgery were identified in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005 to 2013. Outcome measures included any HACs: superficial or deep surgical site infection (SSI), venous thromboembolism (VTE), urinary tract infection (UTI). Spine surgery patients were compared with those undergoing other common procedures. Random forest followed by multivariable regression analysis was used to determine risk factors for the occurrence of HACs.
Results:
A total of 90 551 elective spine surgery patients, of whom 3021 (3.3%) developed at least 1 HAC, 1.4% SSI, 1.3% UTI, and 0.8% VTE. The occurrence of HACs for spine patients was predicted with high accuracy (area under the curve [AUC] 77.7%) with the following variables: female sex, baseline functional status, hypertension, history of transient ischemic attack (TIA), quadriplegia, steroid use, preoperative bleeding disorders, American Society of Anesthesiologists (ASA) class, operating room duration, operative time, and level of residency supervision. Functional status and hypertension were HAC predictors for total knee arthroplasty (TKA), bariatric, and cardiothoracic patients. ASA class and operative time were predictors for most surgery cohorts. History of TIA, preoperative bleeding disorders, and steroid use were less predictive for most other common surgical cohorts.
Conclusions:
Occurrence of HACs after spine surgery can be predicted with demographic, clinical, and surgical factors. Predictors for HACs in surgical spine patients, also common across other surgical groups, include functional status, hypertension, and operative time. Understanding the baseline patient risks for HACs will allow surgeons to become more effective in their patient selection for surgery.
Introduction
In an effort to further the quality and efficiency of the American health care system, there has been a shift in emphasis from service-based care to a value-based care model. 1 As a part of this push toward increased efficiency, incentives have been put in place to prevent complications and expenditures, as well as improve outcomes. One of these incentives was put forth by the Centers for Medicare and Medicaid Services (CMS) in 2008 in which the institution defined certain nosocomial complications as “never events”—meaning that, given the standard of care is upheld, they should not occur—and categorized them as hospital acquired conditions (HACs). 2 As part of the CMS’s plan to promote prevention of HACs, policies were implemented to withhold hospital reimbursement for costs attributed to HACs. 3 As HACs include very common pathologies, including urinary tract infection (UTI), surgical site infection (SSI), venous thromboembolism (VTE), and certain types of peptic ulcer disease, in spite of their “never event” status, they occur frequently. 4 These adverse events are secondary complications that affect patients following initial hospital admission. The consequences of HACs are robust, including nearly 99 000 deaths annually in the United States and nearly 10% of inpatient hospital costs, nationally amounting to an estimated $88 billion. 5 Specific to spine surgery, postoperative HACs have been shown to lead to longer hospital stay, higher mortality, and higher rates of return to the operating room. 6 Despite advances in perioperative management and surgical technique, patients undergoing spine surgery remain at risk for complication with varying rates in the literature. 7 -9 This has led to HACs becoming an increasing financial burden for institutions as well as having deleterious effects on patient health and outcomes. 10
Given the ubiquity of HAC’s and their impact on patient outcomes and hospital management, understanding their epidemiology and pathogenesis is key to improving their prevention and management. The objective of this study was to define salient risk factors that are accurately predictive for the development of HACs in spine surgeries and compare them with the predisposing factors for other common surgeries.
Methods
Data Sources
The American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) database was used for this study. ACS-NSQIP was developed by the Department of Veterans Affairs in order to track surgical interventions across US hospitals. NSQIP tracks 135 clinical metrics, including preoperative risk factors and demographics, intraoperative variables, and 30-day postoperative outcomes using Current Procedural Terminology (CPT) and International Classification of Disease 9th Revision (ICD-9) coding. 11 More information about the ACS-NSQIP database is available at https://www.facs.org/quality-programs/acs-nsqip/about.
Study Design
This was a retrospective review of the ACS-NSQIP database from years 2005 to 2013. Inclusion criteria were patients older than 18 years who underwent elective spine surgery. Patients were also included if they were undergoing bariatric surgery, hip or knee arthroplasty (THA and TKA, respectively), or cardiothoracic surgery. Exclusion criteria were emergency cases, preoperative sepsis, pneumonia, open wounds, American Society of Anesthesiologists (ASA) class 4-5, prior surgery within 30 days, nonelective procedures, or wound class 2-4. Patients were stratified by whether they experienced at least one hospital-acquired condition (HAC): surgical site infection (SSI), urinary tract infection (UTI), or venous thromboembolism (VTE) within 30 days postoperatively. Elective spine surgery patients were compared with other patient groups listed above. The full list of ICD-9 and CPT codes used to identify these patient cohorts and HACs are included in the appendix.
Data Collection
Demographic and clinical data collected included patient age, sex, body mass index (BMI), and comorbidities, including smoking status, diabetes, hypertension, and a modified Charlson Comorbidity Index based on previously published calculation using the NSQIP database. 12 Perioperative data included length of stay and occurrence of HACs.
Primary Outcomes
Primary outcomes were the occurrence of the 3 most common HACs: superficial or deep SSI, VTE, and UTI.
Statistical Analysis
Primary analysis assessed the frequency of HAC occurrence for each surgical type. Two-sided P values <.05 were considered to be statistically significant. Random forest followed by multivariable regression analysis was used to determine risk factors for the occurrence of a HAC. All statistical analysis was conducted in SPSS version 23.0 (Armonk, NY, USA) and R statistical software.
Results
Patient Sample
A total of 399 686 patients in total were identified in the NSQIP database as undergoing common elective surgical procedures included in this study. Overall, 90 551 elective spine surgery patients were identified in the NSQIP database, of whom 3021 (3.3%) developed at least 1 HAC. Spine surgery patients most commonly experienced SSI (1.4%), followed by UTI (1.3%) and VTE (0.8%, Table 1). HACs experienced by spine surgery patients were compared to other common elective surgical groups, including bariatric surgery, TKA, THA, and cardiothoracic surgery. Among common elective surgery, cardiothoracic surgery had the highest HAC rate at 5.9%, followed by TKA (3.4%), and spine surgery (3.3%). Of note, spine surgery with fusion had an HAC rate of 3.8% (Table 1).
Breakdown of Number of Patients With an HAC for Each Surgery Type Under Investigation.
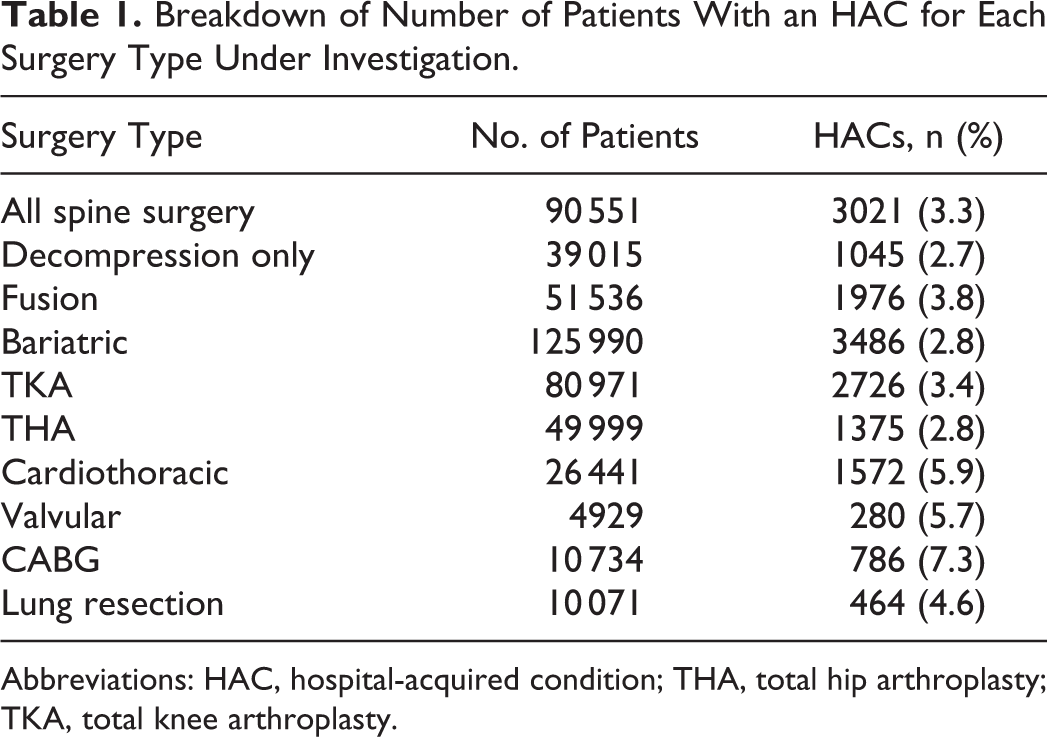
Abbreviations: HAC, hospital-acquired condition; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Predictors of HACs for Spine Surgery
The occurrence of a HAC for spine patients was predicted with high accuracy (area under the curve [AUC] = 77.7%) with the following variables, ranked by importance (Table 2): female sex (odds ratio [OR] 1.65, confidence interval [CI] 1.02-2.66), age (OR 1.014, CI 1.005-1.023), baseline nonambulatory functional status (OR 3.08, CI 1.43-6.62), hypertension (OR 1.57, CI 0.91-2.67), history of transient ischemic attack (TIA) (OR 3.21, CI 1.30-7.93), quadriplegia (OR 8.83, CI 2.22-35.03), steroid use for chronic conditions, preoperative bleeding disorders, ASA class, duration the patient is in the operating room, operative time, and level of residency supervision.
Variables Predicting Hospital-Acquired Complications Across Surgical Procedures and Ranked by Importance.
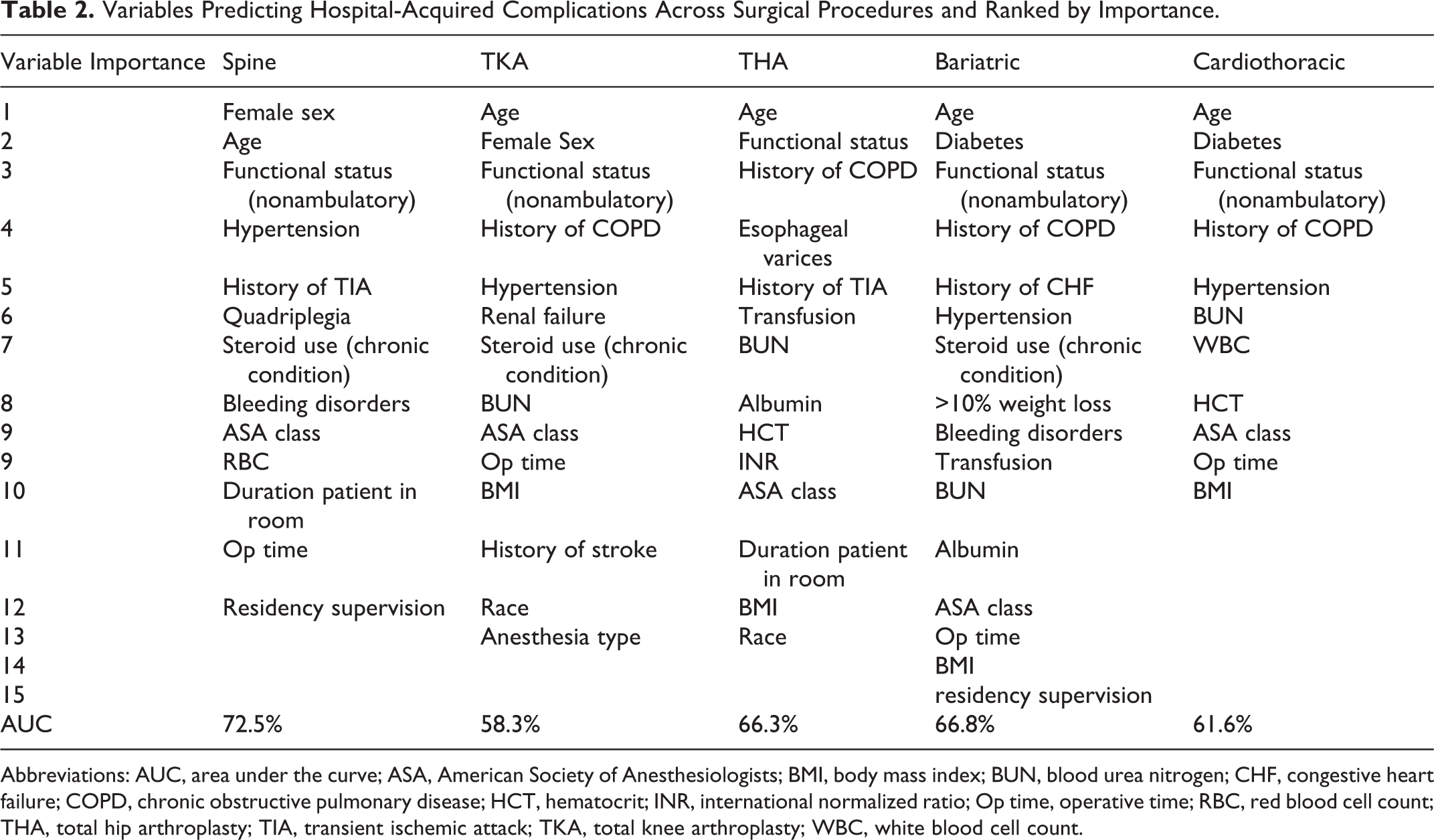
Abbreviations: AUC, area under the curve; ASA, American Society of Anesthesiologists; BMI, body mass index; BUN, blood urea nitrogen; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HCT, hematocrit; INR, international normalized ratio; Op time, operative time; RBC, red blood cell count; THA, total hip arthroplasty; TIA, transient ischemic attack; TKA, total knee arthroplasty; WBC, white blood cell count.
Predictors of HACs for Bariatric Surgery
HAC development for bariatric surgery patients was predicted with high accuracy (AUC = 66.7%) using the following combination of factors, ranked by importance: age, diabetes, baseline nonambulatory functional status, history of chronic obstructive pulmonary disease (COPD), history of congestive heart failure (CHF), hypertension, steroid use for chronic conditions, >10% weight loss in the past 6 months, bleeding disorders, preoperative blood transfusion, preoperative blood urea nitrogen levels, preoperative albumin levels, ASA class, operative time, BMI, and level of residency supervision.
Predictors of HACs for TKA
HAC development for TKA patients was predicted with high accuracy (AUC = 57.5%) using the following combination of factors, ranked by importance: age, female sex, baseline nonambulatory functional status, history of COPD, hypertension, renal failure, steroid use for chronic conditions, preoperative blood urea nitrogen levels, ASA class, operative time, BMI, history of stroke, race, and anesthesia type.
Predictors of HACs for THA
HAC development for THA patients was predicted with high accuracy (AUC = 71.1%) using the following combination of ranked factors: age, baseline nonambulatory functional status, history of COPD, esophageal varices, history of trans ischemic attack, preoperative blood transfusion, preoperative blood urea nitrogen levels, preoperative serum albumin levels, preoperative hematocrit levels, preoperative international normalized ratio of prothrombin time values, ASA class, duration the patient was in the operating room, BMI, and race.
Predictors of HACs for Cardiothoracic Surgery
HAC occurrence for cardiothoracic surgery patients was predicted with high accuracy (AUC = 69.2%) using the following combination of ranked factors: age, diabetes, baseline nonambulatory functional status, history of COPD, hypertension, preoperative blood urea nitrogen levels, preoperative white blood cell counts, preoperative hematocrit levels, ASA class, operative time, and BMI.
Comparing HAC Predictors Across Surgical Cohorts
Other common surgical procedures had similar predictors of HACs to the spine surgery patient population being studied (Table 2). Functional status was a strong predictor of experiencing a HAC for TKA, THA, bariatric, and cardiothoracic patients similarly to spine surgery patients. Hypertension was a strong predictor of HAC occurrence for TKA, bariatric, and cardiothoracic surgeries as well, similarly to spine surgery patients. ASA class and operative time were also predictors for almost all surgery cohorts. By contrast, history of TIA, preoperative bleeding disorders, and steroid use were all predictive for spine surgery patients but less predictive for most other common elective surgical cohorts.
Discussion
With growing focus on value-based care in the current health care system, greater emphasis has been placed on improving system efficiency: reducing readmissions, complications, and errors. 1 In 2008, the CMS began an initiative to improve patient care as well as decrease complications and costs. This initiative involved defining certain iatrogenic pathologies they aimed to reduce as “hospital-acquired conditions” (HACs) and incentivized their prevention by modifying payment plans so that hospitals would no longer be reimbursed for HAC associated treatment during the inpatient setting. 2,3 With adverse events included in their definition such as decubitus ulcer, fall, and UTI, these “never events” are not uncommon and the US Department of Health and Human Services estimated that an HAC occurred in 11.5% of hospital courses in 2015. 13 The significant prevalence of HACs beckons further investigation of their distribution and predisposing factors to facilitate better management and prevention.
While HACs after spine surgery have been well described in the literature, predictors of these complications post spine surgery have sparsely been published and have not led to a significant consensus. 14,15 That being said, a review of the literature shows certain risk factors have been identified as predictive for the development of post–spine surgery HACs, including comorbidities, functional status, operation time, ASA score, and increasing age. 16 -19 Studies on obesity as a predictive factor for complications represent the uncertainty of consensus with regard to risk factors for HACs in spine surgery. For example, in 2003, Olsen et al 20 found morbid obesity to be an independent risk factor predictive of SSI, which is the most common post–spine surgery HAC in our data as well as in previous studies. 21 Conversely, Yadla et al 22 conducted a study on 87 consecutive patients that showed no association between obesity and incidence of complications, major or minor. The continued deliberation over predictive risk factors for HACs following spine surgery necessitates studies like this one to bring clarity to this emerging topic.
Utilizing information from the NSQIP database, our study was able to predict with high-accuracy the occurrence of HACs in spine surgery patients as well as other common elective surgery patients (Tables 1 and 2). The predictive variables identified included patient, clinical, and surgical factors. Certain variables, such as sex fluctuated in predictiveness across different procedures, while others such as medical comorbidities and functional status were similarly predictive in spine as well as other elective surgeries.
Patient factors predictive of HAC’s in elective spine surgery included (in order of influence) female sex and age. While age has been demonstrated in the literature to be a predictive risk factor for complications post–spine surgery, there is less consensus on the predictive value of biological sex for complications in spine surgery. 15,22 -26 For example, Schoenfled et al 27 and Shen et al 28 found females to be at increased risk for complications after spine surgery; whereas, in a prospective study Reis et al 14 found no significant difference in complication risk between males and females. Furthermore, a 2015 meta-analysis displayed no significant differences between the sexes with respect to postoperative complications in spine surgery patients, but noted that males were at increased risk of mortality. 23 Our finding that not only is female sex predictive of HACs post–spine surgery, but in our analysis of 90 551 spine surgery patients, was the most predictive factor adds important understanding to this ongoing discussion.
The clinically based risk factors obtained from our analysis that were most predictive for post–spine surgery HACs were (in order of influence) functional status, medical comorbidities, ASA class, and abnormal lab values. The comorbidities noted included hypertension, history of TIA, quadriplegia, chronic steroid usage, and bleeding disorders. Comorbidities are well described as increasing risk of complication as baseline pathology can precipitate and exacerbate the many insults sustained during a surgery. 29 Hypertension was similarly noted to be a risk factor for certain HACs in multiple studies analyzing the association between medical comorbidities and postoperative spine patient complications. 22,30,31 Of all the clinically based risk factors, functional status and hypertension were the most predictive of the development of HACs after elective spine surgery. Additionally, while BMI was noted to be predictive for HACs in TKA, THA, bariatric surgery, and cardiothoracic surgery, our analysis did not reveal BMI to be correlated with HACs in spine surgery—contributing new findings to this debated topic in which the literature has not reached a consensus. 16,22,27,32
The surgical variables that accounted for the most accurate prediction of HACs following elective spine surgery were operative time as well as residency supervision. Operative time was also predictive across the different surgical procedures aside from THA (duration of patient in operating room, was however, predictive for HACs in THA). Operative time is a longstanding identified risk factor within the literature, associated with many complications including HACs. 27,33
This study identifies female sex, age, and functional status as the most predictive variables in the incidence of HACs in spine surgery. Our analysis highlights patient, clinical, and surgical factors that are predictive of HACs that surgeons can use to improve their surgical patient selection, perioperative counseling, and overall care.
Limitations of this study include its retrospective nature, use of the NSQIP database (which is not specifically designed for spine surgery and therefore lacks certain variables important in the specialty), as well as the use of ICD-9 and CPT codes to isolate surgical populations—potentially diminishing the acquisition of an unbiased patient population. Additionally, the use of SSI, VTE, and UTI as representative of all HACs is a limitation of our study due to the available information in the NSQIP database. The NSQIP database was designed in part to identify occurrence of specific adverse events, including never events. This may be reflective of the large number of well-controlled patients with chronic conditions included in the database. Despite these limitations, we believe our analysis provides meaningful understanding to the development of HACs in spine surgery.
In conclusion, we found patient, clinical, and surgical factors to be predictive of the development of HACs in spine surgery patients as well as other common elective surgeries. There was significant overlap in predictive factors with age, functional status, operative time, and comorbidities found to reach predictive significance across the common elective surgical cohorts. Female sex was the most accurate predictor of an HAC in spine surgery followed by age and functional status, respectively. We believe these findings will allow surgeons to become more effective in their selection, perioperative counseling, and overall care of patients. Predictive modeling, used within this study, can be used by hospital systems and payers to decipher appropriate care by the federal payers of Medicare and Medicaid to deny payments in cases of HAC occurrences. Furthermore, this is the first study of its kind to identify comparatively the rates among spinal procedures relative to other elective procedures. Therefore, we feel this provides perspective of normalcy in terms of these rates, and offers surgeons’ evidence that disparate rates can occur, and not necessarily that payment for the entire hospital occurrence should be denied.
Footnotes
Appendix
CPT Codes Used in This Study to Identify Each of the Surgical Groups.
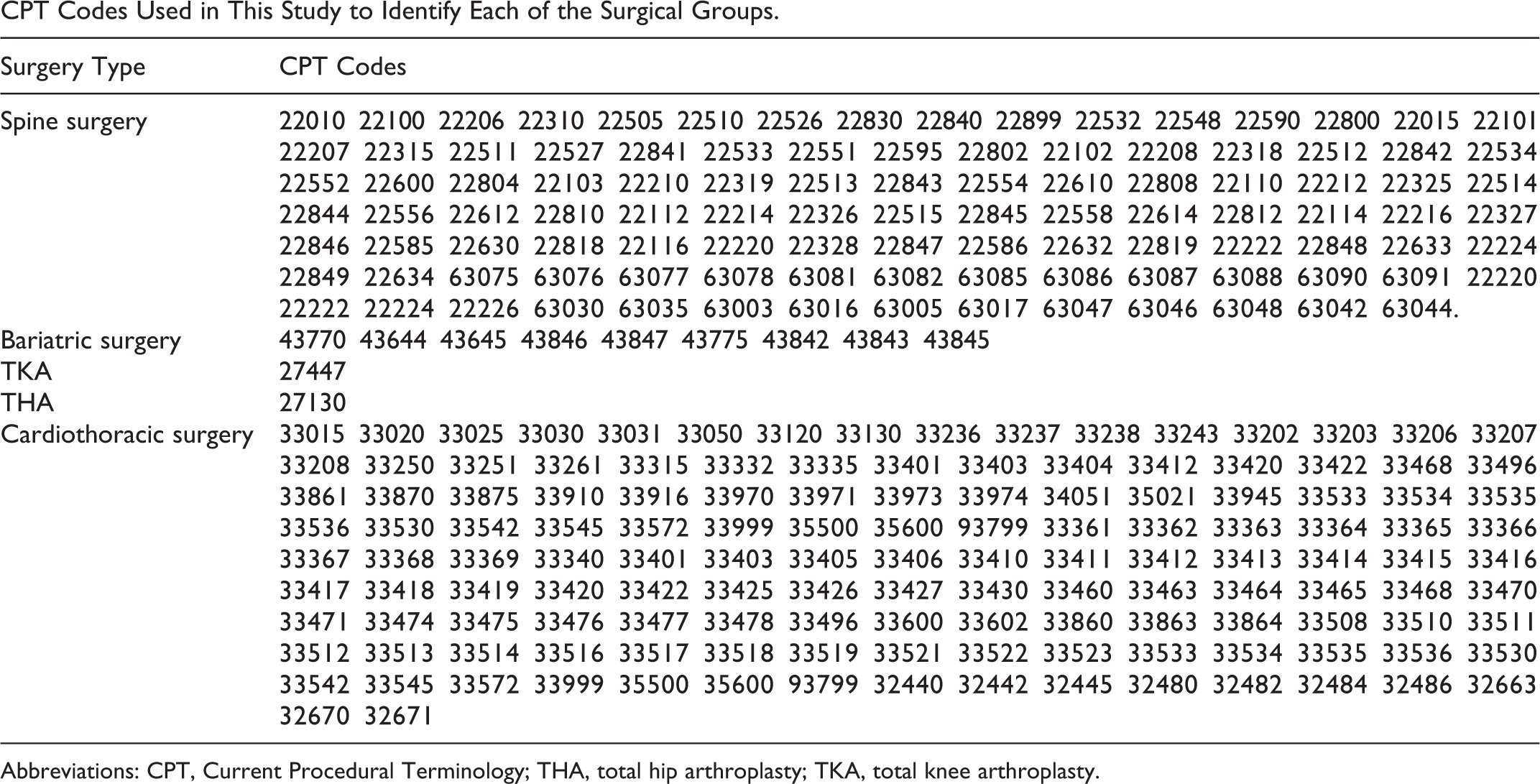
| Surgery Type | CPT Codes |
|---|---|
| Spine surgery | 22010 22100 22206 22310 22505 22510 22526 22830 22840 22899 22532 22548 22590 22800 22015 22101 22207 22315 22511 22527 22841 22533 22551 22595 22802 22102 22208 22318 22512 22842 22534 22552 22600 22804 22103 22210 22319 22513 22843 22554 22610 22808 22110 22212 22325 22514 22844 22556 22612 22810 22112 22214 22326 22515 22845 22558 22614 22812 22114 22216 22327 22846 22585 22630 22818 22116 22220 22328 22847 22586 22632 22819 22222 22848 22633 22224 22849 22634 63075 63076 63077 63078 63081 63082 63085 63086 63087 63088 63090 63091 22220 22222 22224 22226 63030 63035 63003 63016 63005 63017 63047 63046 63048 63042 63044. |
| Bariatric surgery | 43770 43644 43645 43846 43847 43775 43842 43843 43845 |
| TKA | 27447 |
| THA | 27130 |
| Cardiothoracic surgery | 33015 33020 33025 33030 33031 33050 33120 33130 33236 33237 33238 33243 33202 33203 33206 33207 33208 33250 33251 33261 33315 33332 33335 33401 33403 33404 33412 33420 33422 33468 33496 33861 33870 33875 33910 33916 33970 33971 33973 33974 34051 35021 33945 33533 33534 33535 33536 33530 33542 33545 33572 33999 35500 35600 93799 33361 33362 33363 33364 33365 33366 33367 33368 33369 33340 33401 33403 33405 33406 33410 33411 33412 33413 33414 33415 33416 33417 33418 33419 33420 33422 33425 33426 33427 33430 33460 33463 33464 33465 33468 33470 33471 33474 33475 33476 33477 33478 33496 33600 33602 33860 33863 33864 33508 33510 33511 33512 33513 33514 33516 33517 33518 33519 33521 33522 33523 33533 33534 33535 33536 33530 33542 33545 33572 33999 35500 35600 93799 32440 32442 32445 32480 32482 32484 32486 32663 32670 32671 |
Abbreviations: CPT, Current Procedural Terminology; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter G. Passias, MD, reports personal consulting fees for Spinewave, Zimmer Biomet, and Medicrea outside the submitted work. Virginie Lafage, PhD, is paid for lectures by Depuy Synthes, Nuvasive, K2M, and Medtronic and is a Nemaris Board member and shareholder.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.