
Abstract
Introduction
This focused review reports on the impact of self-management interventions on depression in people with a mobility disability.
Method
There were two phases to the search including a comprehensive scoping review of the literature examining multiple secondary conditions impacted by self-management programs (Phase 1) and a focused review of the literature detailing the impact of self-management interventions on depression (Phase 2). CINAHL, PubMed, and PsyclNFO were searched for articles published between January 1988 through August 2014 and studies were screened by the first author based on specific inclusion and exclusion criteria.
Results
Twenty-five studies met criteria with results, demonstrating a mixed effect of self-management programs on depression. Sixteen studies included an intervention and control/comparison group, of which eight (50%) had a significant effect on depression. A further nine studies did not include a control/comparison group and five found significant changes in depression and four found no change. Eighteen out of 25 studies (72%) were rated as having moderate-to-high bias and nine different outcome measures were used across studies.
Discussion
Based on the mixed findings and varied approaches adopted for intervention and outcome assessment, future research should adopt a more rigorous methodological approach to examine self-management interventions on depression.
Introduction
Due to the complexity of mobility impairments (eg, spinal cord injury [SCI] multiple sclerosis), there is a recognized need for increased self-management support to reduce secondary and chronic conditions,1–3 as individuals often have to self-manage diverse aspects of their health and health care. The importance of self-management is emphasized by the fact that disability increases an individual's risk of experiencing secondary (eg, pressure ulcers, urinary tract infections, bowel management issues, pain, depression) and chronic conditions (eg, diabetes, heart disease), with evidence suggesting that the issue is the greatest among people with mobility impairment. 4 These secondary and chronic conditions have been documented to have a significant impact on an individual's quality of life, morbidity, and mortality. Despite this, it is important to recognize that secondary and chronic conditions are preventable if individuals are able to appropriately self-manage their health and health care. 5 Therefore, clinicians and researchers are challenged to find ways to positively impact the health promoting behaviors of people with mobility impairments.6–8
One secondary condition that has a significant impact on the health and function of people with mobility impairment is depression. In the general population in the United States, there is a lifetime prevalence of major depressive disorder of 19.1%, although this is higher in people with mobility impairment. For example, the prevalence of depression in people with multiple sclerosis has been reported at 50%, 9 and it is estimated that this rate is 40% in people with SCI during acute rehabilitation. 10 The high prevalence of depression in people with mobility impairment is compounded by the negative impact on other areas of functioning. Specifically, depression has been linked with reduced functional improvements, decreased mobility, and lower functional independence in people with SCI completing inpatient rehabilitation 11 as well as poor treatment compliance in people with multiple sclerosis. 12 Fortunately, depression can be modified and prevented through the use of self-management programs.13–16
Thus, the purpose of this study is to provide a focused review of the literature on self-management programs developed to prevent or manage depression in individuals with mobility impairment.
Methods
Procedure
There were two phases to the current review. During Phase 1, we completed a scoping review of the literature examining the impact of self-management programs on secondary conditions in people with mobility impairments. The population of interest included people with a congenital or acquired (ie, disease, injury) health condition that impaired mobility. Six of the most prevalent secondary conditions experienced by people with mobility impairment17–19 were used as search terms and included chronic pain, chronic fatigue; depression/mental health, urinary tract infections, bowel/ bladder issues, and pressure ulcer/sore. Self-management interventions focused on positively impacting one of these six secondary conditions were included in the scoping review. Phase 2 involved completing a focused review of the literature using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 20 as a guide. Specific inclusion and exclusion criteria were developed and are described in Froehlich-Grobe, Driver, and Sanches. 21
Literature search
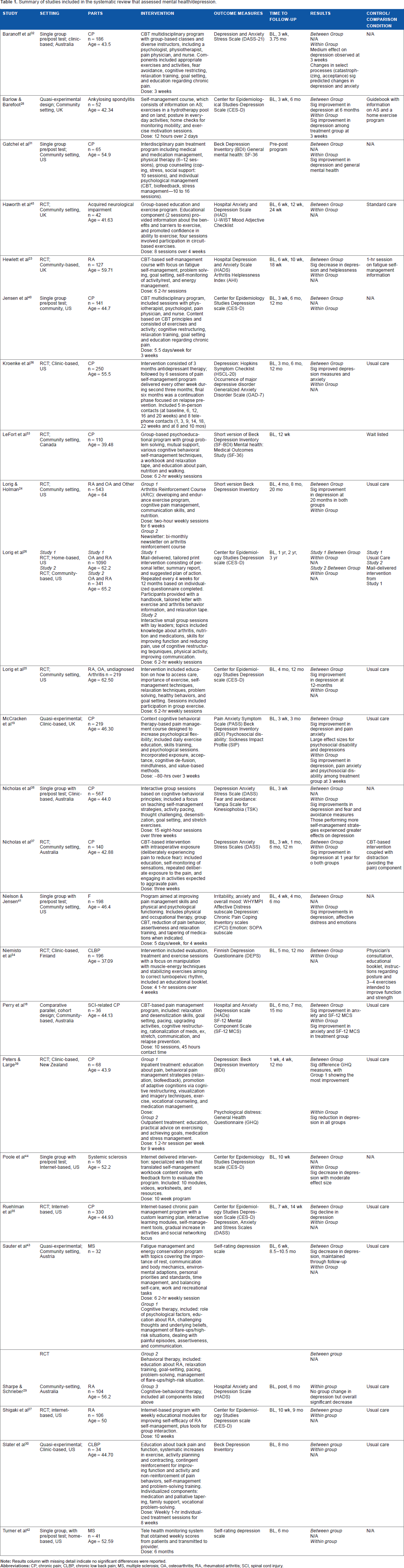
CINAHL, PubMed, and PsyclNFO were searched using a truncated algorithm in September 2014, for papers published between January 1988 and August 2014. Keywords included disability (disability*), physical disability (disability*), mobility impairment, self-management, self-care, self-regulation, lifestyle, self-control, secondary conditions, urinary tract infection, bladder/bowel problems, pain, chronic pain, fatigue, depression, and mental health. The reference lists of identified literature were also manually searched. The results of Phase 1 and 2 are outlined in Figure 1 and the process of identifying appropriate articles is described in Froehlich-Grobe et al. 21 Ultimately, 25 publications focused on the impact of self-management interventions on depression as the primary outcome. The first author then recorded key components of the literature into Table 1.

PRISMA flow diagram. Adapted from Moher et al. 20
Summary of studies included in the systematic review that assessed mental health/depression.
Review of Study Bias
The Cochrane Risk of Bias Tool 22 was used to assess bias and included the evaluation of sequence generation, allocation concealment, blinding, incomplete outcome data assessed, and free of selective outcome reporting. Studies with all criteria met were classified as low risk of bias, >1 partially met were moderate risk, and >2 were high risk.
Results
Participants
Populations comprised individuals with arthritis (n = 7/rheumatoid and osteoarthritis),23–29 back pain (n = 6),30–35 chronic pain (n = 7/lower body),19,36–41 and neurological disorders including SCI, 18 multiple sclerosis,42,43 systemic sclerosis, 44 and general neurological impairment (brain, spinal condition, or neuropathy). 45 Participant ages across these studies ranged from 36 to 65 years (mean age 49 years old) with sample sizes ranging from 16 to more than 1000. For studies that reported race, most included white participants (60%-98% white participants in sample),19,27,31,35,36,39–42,44 with only one study focusing solely on Spanish-speaking individuals. 25 Women comprised most participant samples and studies typically included three to four times as many women.
Settings
The majority of studies were completed in a hospital-based outpatient clinic setting18,19,23,28–33,36–38,40,41,45 with other settings including online/telehealth interventions,27,35,42,44 and community (mail or small group).24–26 One study compared the effect of an intervention between individuals in an inpatient and outpatient setting. 39 Thirteen studies were completed in the North America,24–27,30,31,33,35,36,40–42,44 six in Europe,19,23,28,34,43,45 and six in Australia/ New Zealand.18,29,32,37–39
Intervention
All of the programs were multidisciplinary and combined cognitive (eg, restructuring thoughts), behavioral (eg, goal setting, utilizing social support, problem solving), physical (eg, therapy, exercise, relaxation), and medication therapy. Most studies formally included cognitive behavioral therapy (n = 11) into the self-management program.18,23,27,29,31–33,35–37,40 The programs were also delivered in different formats including individualized, small group, or online/telephonically. The length of the intervention ranged from being individualized, 31 to three weeks19,40,41 to monthly for one year. 26 Finally, social cognitive theory was the theoretical framework used to develop the respective interventions.27,28,36,45
Outcome measures
Depression was measured with nine different outcomes assessments with the most commonly used assessments being the Center for Epidemiological Studies-Depression Scale,25–28,35,40,44 Hospital Anxiety and Depression Scale,18,23,29,45 Beck Depression Inventory,19,30,31,39 Depression and Anxiety Stress Scale,32,35,37,38 and Short Version of Beck Depression Inventory.24,33
Results
Of the 25 studies, results indicated a mixed effect of the intervention on depression; eight found a significant improvement in depression when compared to the control/comparison group,18,19,23,25,28,35,36,43 eight found no difference,26,27,30,33,34,40,42,45 and five studies designed without a comparison group reported a significant difference over time.31,32,38,41,44 Four studies also reported no significant differences between groups but reported a significant difference when all participants were aggregated.24,29,37,39 In studies where a significant effect was reported, maintenance of changes varied from 3 weeks 19 to 12 months.34,36 The length/intensity of the intervention did not have a consistent connection with effectiveness of the intervention on reducing depression.
Study bias
Out of 25 studies, 18 (72%) had moderate-to-high bias (Table 2) with lack of blinding, allocation concealment, and sequence generation being the most prevalent issues, although many studies did not include enough detail to assess bias.
Methodological quality of included studies (n = 25).

Discussion
This focused review suggests that there is a growing body of literature examining the effect of self-management interventions on depression in people with mobility impairment. This is emphasized by the fact that a greater number of the 25 articles identified have been published more recently (1980's = 1; 1990's = 5; 2000's = 8; 2010's = 10). Overall, results of the self-management intervention were mixed. For example, interventions were equally effective for all samples (ie, arthritis, back/chronic pain, neurological impairment). However, while the majority of studies included people with arthritis and chronic back pain/pain, few of the published interventions included people with SCI or multiple sclerosis, despite the recognized need.1,3,10,46 This provides opportunity for future intervention efforts for these populations. The content of the intervention was also mixed (eg, exercise prescription, relaxation techniques, nutrition, self-talk), although cognitive behavioral therapy was the most commonly adopted approach. One result of note across studies that reported adherence was that people who completed more components of the intervention (eg, greater attendance and tracking of behaviors) experienced improved outcomes. This finding emphasizes the important role that participant engagement and consistent tracking of behavior has on self-management behavior. 38 Finally, participants benefited from short interventions with less dosage (eg, 12 hours over 3 weeks) as well as more intense and extended programs (eg, 45 hours over 15 months).
This variability may be due to methodological limitations common across studies. First, 72% of reviewed studies were determined to have moderate-to-high risk of bias, mainly as a result of a lack of blinding and concealing participant allocation to groups (although this is challenging with self-management intervention delivery). This significantly impacts the reliability and validity of results and ability to generalize findings between settings. Second, the variability of outcome measures (n = 9) used to assess depressive symptoms, substantially limits the ability to directly compare study findings. Third, few studies (only 4/25) used theory to guide intervention development,27,28,36,45 although several studies incorporated theoretical components such as self-efficacy or cognitive behavioral strategies (eg, goal setting, self-monitoring). Fourth, the body of evidence lacks racial and gender diversity, as most studies included white females, with only one intervention modified to address the needs of a minority group. 25 Fifth, participants’ adherence to intervention components was rarely assessed and thus it cannot be determined whether non-significant findings were due to ineffective intervention or dose received.
Overall, this focused review suggests that a variety of different approaches are taken to self-management intervention delivery and measurement. While individual investigators may be systematic in their approach (see Kate Lorig's work) the field of self-management intervention research has greater variability in delivery (eg, intensity, duration, theoretical underpinning), setting, and outcome measures used. Sallis et al 47 introduced a behavioral epidemiological framework that suggests if research efforts are to effectively address public health issues, such as depression in individuals with disability, they must be completed sequentially. Specifically, the framework proposes five phases of research that build upon the evidence base sequentially and include (1) linking the health behavior (eg, depression) to outcomes (eg, return to work, quality of life, functional ability), (2) identifying tools to accurately measure the health behavior, (3) detecting mediators and moderators of the behavior, (4) developing evidence-based behavioral interventions, and (5) disseminating results to influence policy and programming. Based on the large differences found in approach, outcome measures, and results, there is a clear opportunity to adopt a more systematic approach to self-management research addressing depression in individuals with mobility impairment. Future efforts should be made to standardize factors such as setting (eg, clinic, community, telehealth), mode and timing of outcome assessments, and intensity, duration, and frequency of intervention.
Telehealth interventions (ie, telephonic, web-based) present clinicians and investigators with a unique opportunity to deliver an intervention while overcoming many transportation barriers faced by people with mobility impairment. Of the four studies that adopted a telehealth approach in the current review,27,35,42,44 two reported a significant decrease in depression.
In conclusion, this review suggests that self-management approaches have successfully reduced depression among people with mobility impairment in about half of the published studies. Yet, it is also important to recognize that the evidence base is best characterized as having moderate-to-high risk of bias and relies upon self-reported data. Future efforts should include a systematic approach to self-management program delivery (ie, setting; mode and timing of outcome assessment; frequency, duration, and intensity of intervention), examine telehealth approaches, document intervention adherence, use randomized controlled designs, and standardized presenting results to include effect sizes to facilitate the ability to complete meta-analyses.
Author Contributions
Conceived and designed the experiments: SJD, KFG, KDS. Analyzed the data: SJD, KFG, KDS. Wrote the first draft of the manuscript: SJD. Contributed to the writing of the manuscript: SJD, KFG, KDS. Agree with manuscript results and conclusions: SJD, KFG, KDS. Jointly developed the structure and arguments for the paper: SJD, KFG, KDS. Made critical revisions and approved final version: SJD, KFG. All authors reviewed and approved of the final manuscript.