
Abstract
Purpose
The aim of this study was to assess bleb function using Wuerzburg bleb classification score (WBCS) for bleb morphology on slit lamp, intraocular pressure (IOP), and gonioscopy.
Methods
A total of randomly selected 30 eyes posttrabeculectomy were assessed for bleb function with the trio of bleb morphology, IOP, and gonioscopy. Bleb was assessed using the WBCS of 0–12 on slit lamp, IOP was assessed using applanation tonometry, and visualization of inner ostium and iridectomy were assessed using gonioscopy. Postoperative patients of less than six weeks were excluded from the study.
Results
The correlation between WBCS and the duration of trabeculectomy was found to be highly significant (P value = 0.029). The correlation of IOP with WBCS was also found to be strongly positive (P = 0.000). IOP was found to be highly associated with peripheral iridectomy (P = 0.000), internal window (P = 0.001), and bleb characteristics.
Introduction
Trabeculectomy (Trab), introduced by Cairns 1 in 1968, is widely applied by surgeons worldwide and is still considered the gold standard. Good functioning of Trab is dependent on the proper outlet of aqueous from the scleral ostium into the subconjunctival space, which leads to the formation of filtering bleb. The functioning of filtering bleb is in turn influenced by a number of factors, including postoperative wound-healing properties. 2 Scarring of structures at Trab site, including conjunctiva, episclera, scleral flap, and ostium, may lead to poor formation of bleb and hence poor shunt function, resulting in suboptimal intraocular pressure (IOP) control. In spite of surgical meticulousness, Trab failures occur at an inconstant rate. Reports about long-term success rates of this procedure are difficult to equate. The changes in bleb morphology can help us to ascertain the early failing blebs and also help to foretell the cases that are likely to fail in the future. Along with gonioscopy, we can also find the cause behind the failure.
Aim
The aim of this study was to assess bleb function using trio of IOP, gonioscopy, and Wuerzburg bleb classification score (WBCS) for bleb morphology.
Objective
The primary objective of this study was to find the correlation between IOP and bleb morphology and its association with gonioscopy. The secondary objective of this study was to find the correlation between IOP and duration of surgery.
Methods
This was a cross-sectional study where patients were selected from the hospital over the time without any follow-up. A total of 30 eyes of 12 females and 18 males were examined over a period of one and a half years from July 2014 to December 2015. Patients gave their written, informed consent to participate in this research, which was conducted in accordance with the principles of the Declaration of Helsinki. The research protocol was approved by the Ethical and Research Committee of SAMC & PGI Indore.
Inclusion criteria
Postoperative patients of more than three months from Trab were included.
Patients with only Trab without any intervention of mitomycin-C were included.
Exclusion criteria
Postoperative patients of less than three months of surgery were excluded. Patients presenting to our institute with a history of Trab were subjected to routine thorough examination.
Vision was recorded on Snellen chart, and slit lamp examination to study the morphology of bleb, gonioscopy by two mirror goniolens, fundus examination by 90-D lens, and IOP recording by applanation tonometry were performed. Patients were divided into the following two groups: group A with IOP ≤ 18 and group B with IOP > 18 (Table 1). Distribution of patients on the basis of IOP.

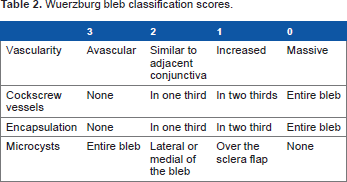
Wuerzburg bleb classification scores.
Gonioscopy was performed using two-mirror gonio lens. The patency of internal ostium and the inner window was noted, and the photograph was taken.
Statistical Analysis
Correlation was calculated between two numeric variables, and analysis of variance was performed to assess the difference in mean values among more than two groups, whereas the significance of association and difference between categorical variables were assessed by using the chi-square test. All values were calculated at 95% confidence level. SPSS version 21 was used for performing all statistical tests.
Observations
Trab is still the gold standard surgical management for various types of glaucoma. The clinical assessment of surgical success in the postoperative period is clinically based on IOP control and the development of a filtering bleb. Currently available bleb grading systems are all based on the bleb morphologic features as a guide to evaluate bleb function. However, these systems are considered relatively subjective and are prone to interobserver variability.
In our study, we attempted to determine the correlation between WBCS on slit lamp examination, with the gonioscopy findings, and the level of IOP control. This might provide more objective data on subsequent bleb function.
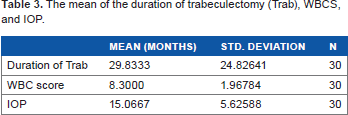
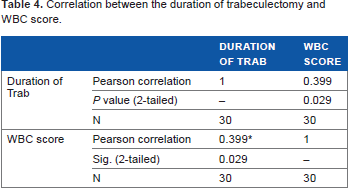
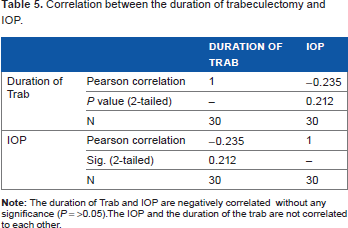
Out of 30 patients, 12 patients were male and 18 patients were female. Descriptive statistics for mean of the duration of Trab, WBCS, and IOP were calculated (Table 3). Positive correlation was found between the duration of Trab and WBCS (Table 4), which was significant (P < 0.05), indicating that as the duration of surgery increases, the bleb score also becomes better. The correlation between the duration of Trab and IOP was found to be negative without any significance (P ≥ 0.05) (Table 5), testifying that there does not exist any correlation between the two. The correlation between IOP and WBCS was found to be significantly negative (P = 0.00) (Table 6), indicating that as the IOP becomes normal, the score attained by the bleb morphology on slit lamp also becomes better. This can be explained by the observation that out of the four patients in group B, three patients had WBCS less than 6 and all of them had IOP levels more than 18 (Graph 1).

Distribution of the two groups according to WBCS.
The mean of the duration of trabeculectomy (Trab), WBCS, and IOP.
Correlation between the duration of trabeculectomy and WBC score.
Correlation between the duration of trabeculectomy and IOP.
Negative correlation between IOP and WBC score.

The mean of IOP was calculated on the basis of presence or absence of peripheral iridectomy (PI) (Table 7). The positive association between IOP and PI was found to be highly significant (P = 0.000) in nature (Table 8). PI was not seen in 50% of patients of group B and 7.69% of patients of group A (Graph 2). This suggests the fact that the presence of patent PI is important for the maintenance of normal IOP and success of the operation. One patient of category other had IOP more than 40 where the pupil was semidilated and corneal edema was present such that PI was not visualized (Fig. 1). The mean of IOP on the basis of presence/absence of internal window was calculated (Table 9) and its association with IOP was calculated, which was found to be positive and also significant (P = 0.001) (Table 10).

Corneal edema (suture present at 10 o'clock) with semidilated pupil.

Distribution of patients according to the absence/presence of peripheral iridectomy (PI).
Mean of IOP depending on the absence or presence of peripheral iridectomy (PI).

The association between IOP and PI was very high, and significant (P = 0.000). The presence of PI is important to maintain normal IOP

Mean IOP for the presence, absence or other of internal ostium.
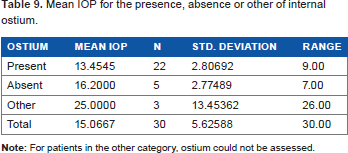
The association between IOP and ostium was highly significant (P = 0.001). Therefore, the patient's internal ostium is important for the maintenance of normal IOP.

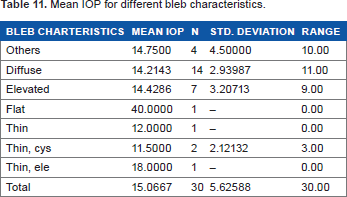
The mean of IOP according to bleb characteristics was calculated (Table 11) and the association was evaluated, which was found to be highly significant (P value ≤ 0.01) (Table 12), suggesting that the bleb characteristics are related to the level of IOP. Out of the four patients in group B, three patients were given a WBCS of 0 because of the absence of microcysts (Graph 3), testifying that the presence of microcysts is important for keeping the bleb functioning. Almost similar features were found when IOP was compared with the presence of vascularization (Graph 4), demonstrating that the presence of vascularization is detrimental to the functioning of the bleb hence decreases the life expectancy of Trab.

Distribution of patients according to microcyst score.
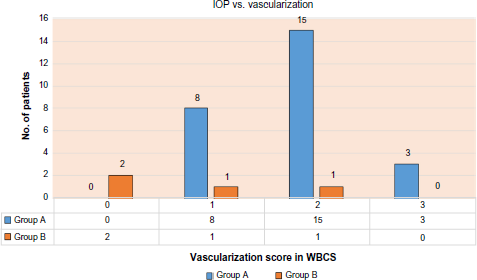
Distribution of patients according to vascularization.
Mean IOP for different bleb characteristics.
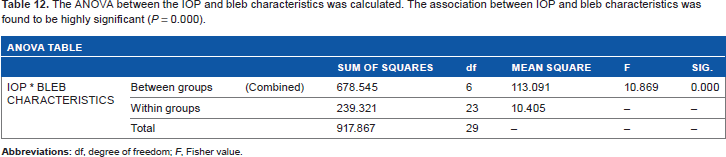
The ANOVA between the IOP and bleb characteristics was calculated. The association between IOP and bleb characteristics was found to be highly significant (P = 0.000).
Discussion
The main aim of filtering surgery is to achieve low levels of IOP in order to prevent further visual field loss. 4 Assessment of Trab has taken a major turn since the last few decades. The advent of new technologies such as anterior segment optical coherence tomography, ultrabiomicroscopy, in vivo confocal microscopy, goblet cell cytology, and indocyanine green angiography has actually revolutionized the assessment of the bleb post-Trab. Along with these, the conventional method of assessing the bleb on slit lamp also developed step by step and various bleb grading systems were published, such as the Indiana bleb grading system, the Moorefield bleb grading system, and the WBCS.
The Moorefield bleb grading and the Indiana bleb grading scores 2 were mainly based on the pictures that were to be compared with the bleb to be assessed, and the bleb was then graded according to the pictures where it would fit the best. This was totally subjective in nature. The occurrence of microcysts and the extent of vascularization were not included in the classification and assessment, which have been proved to actually play a major role in the assessment. The WBCS developed in 1998 included the microcysts and the vascularization and covered few of the loop holes left by the former classifications. Accordingly a bleb having less vascularity as compared to normal conjunctiva and having microcysts and absent corkscrew vessels and encapsulation is predictive of long-term good functioning, and any deviation from these (Fig. 2A and 2B) may lead to failure if proper management is not done on time. As shown in a recently published study by Rotchford and King, 5 there exist currently 92 different IOP-based definitions of success. 3 In our study, we considered Trab as success when the IOP was less than 18 post surgery. We assessed the Trab functioning on the basis of morphology on slit lamp using WBCS, gonioscopic findings, and IOP. Till date, we could not find any study that has used all the three for the evaluation of bleb functioning and hence the success of Trab.

(
In our study, WBCS was negatively and strongly correlated with IOP. This correlates with the findings of Furrer et al. 3 The main aim of their prospective study was to investigate whether there is an association between postoperative IOP and WBCS. They correlated the morphological findings of WBCS and IOP and found a fair association between the attainment of at least seven points and the target IOP. Based on the findings, they concluded that WBCS is applicable in clinical practice.
In our study, we observed that the duration of Trab and WBCS score were strongly and positively correlated. It is very remarkable to compare these results with those published by Klink et al. 6 Even though they did not find any prognostic value of the early WBCS for long-term success of surgery (20% pressure reduction with reference to the pretreated IOP level and an upper IOP limit of 21 mmHg without glaucoma medication), they found that a bleb score of more than 8 points in the first two weeks after Trab seemed to be associated with a lower IOP (≤12 mmHg) one year postoperatively, while patients with a total bleb score of less than 7 two weeks postoperatively showed a higher IOP.
We found no relation between the duration of Trab and IOP as IOP may increase or decrease at any point of course post Trab depending on the different local and systemic conditions.
The presence of microcysts was positively correlated with the decrease in IOP. This is in accordance with Picht and Grehn, 7 Sacu et al. 8 , and Cantor et al. 2
It was also observed that the presence of vascularization (Fig. 2B) was correlated with increased IOP; these findings are in concordance with the findings of Furrer et al. 3 who also found similar results in their study.
On evaluation of bleb characteristics, we found that a flat bleb (Fig. 3D) corresponded to elevated IOP, indicating nonfunctioning, whereas a thin, cystic bleb (Fig. 3C) corresponded to lower levels of IOP, indicating overfiltration. Diffuse blebs (Fig. 3A) and elevated blebs (Fig. 3B) had good IOP levels. These findings are consistent with the findings of Vesti 9 who retrospectively examined 88 eyes after Trab in an attempt to correlate biomicroscopic appearance and function of the filtering bleb with IOP and detect possible risk factors for bleb failure. Blebs were graded into the following three groups: diffuse filtering bleb with or without macroscopic cysts, flap-sized bleb, and bleb failure. A clear association between a diffuse bleb and a good IOP response was observed.

Different types of blebs: (
In this study, the presence of patent PI was positively and strongly correlated with the maintenance of good IOP control. Four out of 30 patients had no PI, and all of them had IOP more than 18 (Fig. 4D). These findings are not related to the findings of Matlach et al. 10 and De Barros et al. 11 who concluded that Trab performed without PI is as effective as surgeries performed with PI. They also reported that PI performed during surgeries increases the chances of postoperative hypotension, hyphema, uveitis, etc., which can be prevented without performing PI.

Different gonioscopy pictures: (
We found that the presence of patent internal ostium is a must for the long-term functioning of Trab. Since Trab surgery involves the formation of an artificial pathway for the drainage of the aqueous to form a new pathway, blockage or hindrance in the pathway will lead to increase in IOP. In this study, we had one patient with fibrosis (Fig. 4A) seen in the area of the inner ostium; one patient with vitreous (Fig. 4C) developing into a complicated cataract operated with ACIOL for which resurgery was planned at another site along with anterior vitrectomy; and three patients with iris blocking the inner ostium (Fig. 4B) totally or partially, of whom one patient with an increase in IOP was reposited and hence released from the inner ostium in the operation theater and the remaining two patients were put under regular follow-up; and many patients had pigmentation in the inner ostium (Fig. 4D) who were also put under careful monitoring.
This was a hospital-based study with a small sample size, which was one of the limitations. Nevertheless, it gives future directions to researchers to conduct a multicentric study with a larger sample size so as to achieve maximum external validity.
Conclusion
The trio of gonioscopy, IOP, and WBCS is a great boon for the assessment of bleb and hence the Trab functioning. The duration of Trab and IOP are not correlated, and IOP may increase or decrease depending on the local and systemic factors. Presence of more microcysts and less vascularization on the filtering bleb results in a better agreement in reaching the target pressure. The IOP is negatively correlated with WBCS. The presence of patent PI and patent inner ostium is important for the long-term functioning of bleb. The bleb morphology is also helpful in predicting the IOP status. The duration of Trab and WBCS are significantly correlated. As the duration increases, the WBCS becomes better.
Practical Implications
The trio of gonioscopy, IOP, and WBCS is a part of the routine ophthalmological examination. These procedures are of great benefit for doctors who are working in setups without ultrabiomicroscopy and optical coherence tomography. In a majority of patients, the cause of failing blebs can also be determined and hence can be rectified. These methods are cost-effective for the patient.
Limitations
The main limitation of the study was the small sample size. The internal morphology of the bleb cannot be studied. It was a cross-sectional study without follow-up. Hence, the morphological changes in the bleb as the duration increases were not studied.
Author Contributions
Conceived and designed the experiments: ST. Analyzed the data: ST, RR. Wrote the first draft of the manuscript: ST, RR. Contributed to the writing of the manuscript: ST, RR, NG. Agree with manuscript results and conclusions: ST, RR, NG. Jointly developed the structure and arguments for the paper: ST, RR. Made critical revisions and approved final version: ST, RR, NG. All authors reviewed and approved of the final manuscript.
Abbreviations
peripheral iridectomy
Wuerzberg bleb classification score
trabeculectomy
intraocular pressure.
Footnotes
Acknowledgment
The authors would like to thank Dr. Jagriti Jain, M.S. Ophthalmology, for the knowledge provided at the time of confusion.