
Abstract
Carotid cavernous fistula is an abnormal communication between the carotid arterial system and the cavernous sinus. We present an interesting, rare case of bilateral spontaneous ‘Barrow type- C’ fistula treated presumptively as conjunctivitis. A 66 year old patient presented in the eye casualty at North Devon District Hospital in January 2016, referred from her General practitioner complaining of bilateral red eyes. She was found to have large, prominently diffused and engorged scleral blood vessels on both sides along with raised intraocular pressures of 26mm of Hg bilaterally. The patient was diagnosed with an indirect carotic cavernous fistulas bilaterally in view of the clinical and radiology findings. Barrow type - C dural fistulas were reported to be seen bilaterally on radiology findings. Patient was referred for interventional treatment to the closest neurosurgical center where she had four failed attempts of coil embolization after which she was referred to a second neurosurgery center at Bristol where she underwent successful coil catheterization as the treatment for her carotid cavernous fistula. Indirect carotid cavernous fistula most commonly occur spontaneously. Bilateral spontaneous indirect carotid cavernous fistula is a very rare diagnosis and and there are very few cases reported in the literature without an underlying etiology or a known cause like Ehlers -Danlos syndrome or diabetes mellitus. Bilateral spontaneous carotid cavernous fistulas are difficult to diagnose due to mild symptoms and no history of trauma. We conclude that carotid cavernous fistulas are a threat to the vision if left untreated due to delayed diagnosis. We recommend considering bilateral carotid cavernous fistula as a differential diagnosis in patients with an ongoing history of red eyes or those unresponsive to conventional topical treatment for conjunctivitis like symptoms.
Introduction
Carotid cavernous fistula (CCF) is an abnormal communication between the carotid arterial system and the cavernous sinus. CCF can be classified in a number of ways, as direct or indirect fistula based on anatomical features, traumatic or spontaneous on the basis of etiological features, or as high or low flow based on hematological basis. The most common etiology of direct fistula is a head trauma, as a result of which the internal carotid artery is damaged and a fistula is formed between the lacerated artery and the cavernous sinus. CCF uncommonly occurs spontaneously though. Barrow and colleagues 1 classified the CCF into direct (type A) and indirect (types B–D) types. Type A is high flow shunts between the internal carotid artery (cavernous portion) and the cavernous sinus and are usually caused by a trauma (rupture) of an internal carotid artery aneurysm.1,2 Type A is more common in men. In women, older than 50 years, types B, C, and D are more common with 7:1 female to male ratio.2,3 Types B, C, and D are fistulas between the cavernous sinus and extradural branches of the internal carotid artery, the external carotid artery, or both. A CCF is usually unilateral but less commonly bilateral and rarely bilateral and spontaneous in nature as observed in our case.
Case presentation
A 66-year-old patient presented in the eye casualty at North Devon District Hospital (Barnstaple, UK) in January 2016, referred from her general practitioner complaining of bilateral red eyes for about 3 weeks (Figures 1 and 2), diagnosed and treated presumptively as conjunctivitis, which was found to be nonresponsive to chloramphenicol 0.5% drops. On questioning, she had complaints of intermittent headache and a feeling of thumping in her head around the same time. She also described that at night she had been experiencing scratchy sounds in her ears for about the same duration of time. She had no complaints registered otherwise. There was no significant past ocular history. Medically, she was treated for hypothyroidism. Her medical history was unremarkable otherwise. There was no history of head or eye trauma.
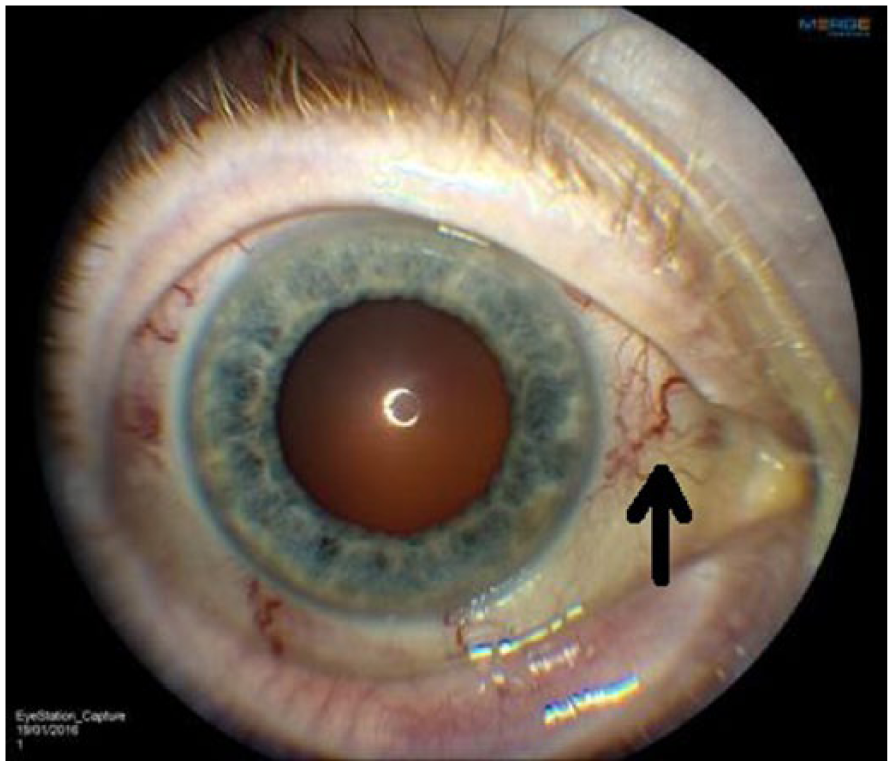
Visible engorged and dilated scleral blood vessels on the right eye (black arrow).
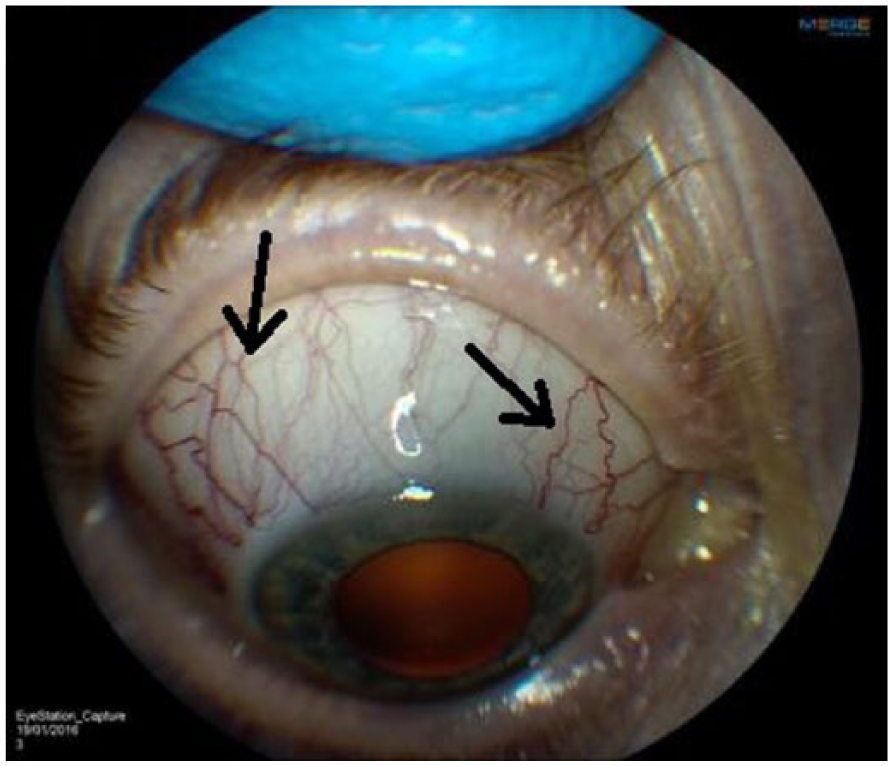
Superiorly visible engorged and dilated scleral blood vessels on the right eye (black arrows).
On examination, the lady had an uncorrected visual acuity of 6/12 on the right eye and 6/6 on the left eye with no improvement of visual acuity on pinhole examination. There were large, prominently diffused, and engorged scleral blood vessels to be seen on both eyes. Visual fields were full to confrontation. Pupil examination was normal with normal reactivity on both eyes. There was no relative afferent pupillary defect. Her intraocular pressures (IOPs) were 19 mm Hg on the right eye and 20 mm Hg on the left eye. She was orthophoric in primary gaze, however, showed mild restriction of her extra-ocular movements bilaterally in horizontal gaze, suggesting both a mild abduction and adduction deficit in the two eyes along with slow saccadic movements overall. Neither proptosis nor bruit was observed at the time. No diplopia was reported by the patient. Fundus examination was unremarkable.
Diagnosis of spontaneous CCF, thyroid eye disease, and orbital varix were considered as differentials. Patient was seen again after 5 days and in review they had developed diplopia on looking at extreme gaze both right and left. She was found to have raised IOPs of 26 mm Hg bilaterally. A B-scan was performed which showed dilated superior ophthalmic veins bilaterally (Figures 3 and 4) which prompted an urgent magnetic resonance imaging (MRI) head scan to be carried out. Results showed dilated left superior ophthalmic vein along with enlarged cavernous sinus on the scan. Our colleagues from the radiology department suspected the same on right side but were not sure and hence the patient was referred by the local radiology department to a neuroradiology unit in a tertiary center for a further computed tomography angiography/MR angiography (CTA/MRA) scan. The CTA scan showed signs of bilateral CCF along with dilated superior ophthalmic veins on both sides (Figures 5 and 6). A further carotid angiogram confirmed bilateral CCF with a markedly dilated superior ophthalmic vein on the left side (Figure 7). The patient was diagnosed with an indirect CCF bilaterally in view of the clinical and radiology findings. Barrow type C-dural fistulas were reported to be seen bilaterally on the radiology findings; however, there were no other associated or underlying pathologies seen on the scans, and pathologies like orbital inflammatory disorders, space-occupying lesion, or cavernous sinus thrombosis were not observed on her MRI, CTA, or carotid angiogram. Patient in the mean time was reviewed again locally after 2 days in the clinic and was found to have a significant reduction in her vision with further increasing IOP. Her visual acuity was reduced to 3/60 bilaterally with IOP of 34 mm Hg on the right side and 32 mm Hg on the left side along with sluggish reaction of pupils on both sides; however, no anisocoria and no relative afferent pupillary defect were noted. She was started on Latanoprost eye drops to both eyes. The patient was also seen by an orthoptist for a formal Hess charting and was found to have a partial left-sided third nerve palsy with mildly reduced adduction on that side. A mild abduction deficit on both sides was also observed which was not clinical of sixth nerve palsy. Arrangements were made to refer the patient urgently to the closest neurosurgery center at Derriford Hospital (Plymouth, UK) where she was seen semi-urgently and four attempts were made to embolize the fistula with coil catheter. However, all four attempts failed and she was referred to a second neurosurgical center in Bristol where she underwent coil catheterization successfully as the treatment for her CCF. After 2 months of the interventional procedure, her symptoms were resolved and her IOP was back to normal at around 16 mm Hg in both eyes along with restoration of full extra-ocular movements on both sides and a normal vision of 6/9 bilaterally.

Dilated superior ophthalmic vein visible on the right eye scan (orange arrow).

Dilated superior ophthalmic vein visible on the left eye scan (orange arrow).
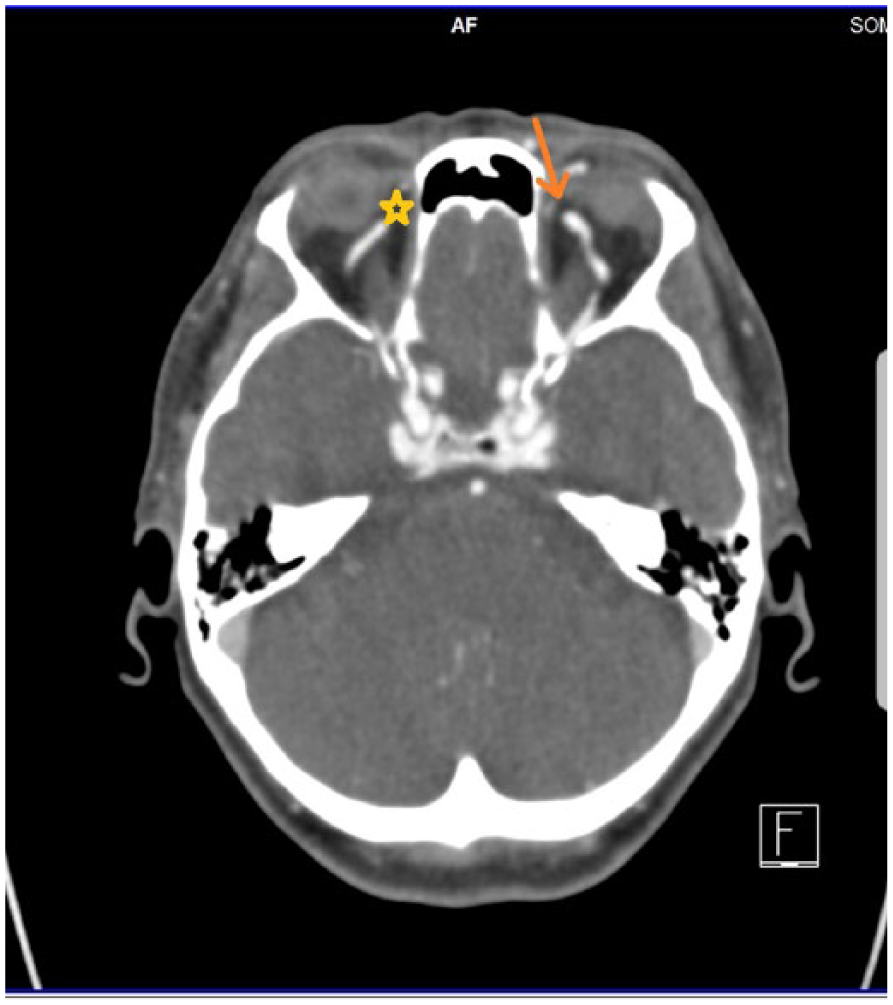
Computed tomography angiogram (CTA) image showing moderately dilated superior ophthalmic vein on the right side (yellow star) and a more marked dilated superior ophthalmic vein on the left side (orange arrow).

Computed tomography angiogram (CTA) images showing prominent superior ophthalmic veins on the right side (yellow stars) and tortuously dilated superior ophthalmic veins on the left side (orange arrows).

Carotid angiogram lateral view showing CCF with a dilated left side superior ophthalmic vein (arrow).
Discussion
CCF is found more commonly as a result of trauma; however, a spontaneous CCF is not uncommon. Helmke and colleagues 4 in their study showed 42 cases of type A nontraumatic CCF. They further suggested that a sudden increase in the intraluminal pressure ruptured the internal carotid artery which may explain the nontraumatic cause of these. Diagnosis of CCFs should be considered with bilateral eye symptoms and bilateral nerve palsies. 5 Treatment of CCF is mainly interventional in nature; however, it includes observation and medical management in a few cases. Type A fistulas very rarely resolve spontaneously; however, type B, C, and D fistulas have a higher incidence of spontaneous resolution.6,7 Therefore, some cases of indirect and low-flow fistulas can initially be observed only or managed conservatively for ocular symptoms with medical management or manual carotid compression. 8 Interventional treatment options include both surgical and endovascular options which are ligation of the external or internal carotid arteries, fistula embolization with glue, microcoils, and stents and detachable ballons. 9
In summary, indirect CCF most commonly occurs spontaneously. 10 Bilateral spontaneous indirect CCF is a very rare diagnosis and there are very few cases reported in the literature without an underlying etiology or a known cause like Ehlers–Danlos syndrome or diabetes mellitus. A recent case report and review article have mentioned only 26 reported cases in literature excluding their 2 cases of bilateral nontraumatic spontaneous CCFs according to their review of literature since 1963. 11 Our literature search has found a total of 35 reported cases of spontaneous, nontraumatic bilateral CCFs since 1963 now including our case. We found another six cases in our review of literature that were not included in this recent literature review along with the two additional cases which they have reported in their article. 11 Table 1 shows a summary of all reported 35 cases of bilateral spontaneous CCF with patient demographic data, reported presentation, treatment, and outcomes. There have been only two reported cases12,13 of bilateral type C fistulas in the literature out of the 35 reported cases of bilateral CCFs (Table 1) which make this case report very rare as our case is presented as the only third case of bilateral Barrow type C fistulas in the literature. Bilateral spontaneous CCFs are difficult to diagnose due to mild symptoms and no history of trauma. B-scan ultrasound is an easy investigative tool which shows dilated superior ophthalmic veins in CCF patients;14–16 hence, CCF can mostly be diagnosed easily in the smaller community hospitals or large general practices with it if the access to B-scan is available. In difficult cases where further investigation is required, MRI head scan becomes necessary as it is critical in diagnosing CCF. Diagnosis may be delayed due to not having the access to MRI facility locally; hence, an important aspect of early diagnosis in some cases is dependent on the ease of access to MRI facility. Optical coherence tomography angiography (OCT-A) is a noninvasive investigation previously limited to retina and posterior segment examinations but is now beginning to be used for assessment of anterior segment vasculature and may hold some utility in evaluation of patients with suspected CCF.17,18 A case report by some researchers have used OCT-A of the anterior segment for studying the delineation of abnormal episcleral venous plexus secondary to dural CCF. 18 We conclude that CCFs are a threat to the vision if left untreated due to delayed diagnosis. Raised venous pressure and IOP in a CCF patient may compromise the retinal perfusion and result in loss of visual acuity. 19 Also, raised IOP as seen in our case can cause damage to the optic nerve by causing secondary glaucoma due to persistently raised IOP if CCF is not treated or there is a delay in the treatment. We recommend considering bilateral CCF as a differential diagnosis in patients with an ongoing history of red eyes or those unresponsive to conventional topical treatment for conjunctivitis-like symptoms.
Review of the bilateral spontaneous carotid cavernous fistula (CCF) reported cases.

Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was obtained from the patient for this case report information and for the images related to the case report to be published anonymously for educational and research purposes.