
Abstract
Cystoid macular edema (CME) is an important cause of visual loss after cataract surgery. Treatment is usually with topical anti-inflammatory agents, with anti-vascular endothelial growth factor agents and steroids used intravitreally in resistant cases. Even though time-domain Stratus OCT can quantify the macular thickness, it cannot prognosticate visual outcomes due to the poor resolution of images, especially the outer segment-inner segment junction. Spectral-domain OCT (SD-OCT) by its ability to acquire large number of images in a short span of time provides high resolution cross-sectional images of the retina, which not only highlights the underlying pathological changes, but in addition can prognosticate visual recovery. We describe pre and post SD-OCT features of a case of refractory CME who was treated with intravitreal triamcinolone actetonide.
Keywords
Introduction
Cystoid macular edema (CME) is a common cause of visual loss after complicated cataract surgery. 1 Intraoperative vitreous loss, placement of anterior chamber intraocular lens, prolonged postoperative inflammation are some of the risk factors associated with CME. 2 Diagnosis is based on the clinical findings and characteristic appearance on fundus fluorescein angiography and optical coherence tomography (OCT).2,3 OCT is a sensitive non-invasive tool in detecting and quantifying the macular thickness associated with CME. Recently, a novel advancement in technology, spectral-domain OCT (SD-OCT), has been used to describe the ultra structural changes in various retinal pathologies. SD-OCT with its ability to acquire large number of scans in a short period of time (the number of A-scans acquired is 40000 as compared to 400 on Stratus OCT) provides high resolution images comparable to histological changes described. 4
In this case report, we describe SD-OCT features of a case of pseudophakic CME which resolved successfully after intravitreal triamcinolone actetonide injection.
Case Report
A 51 year old woman who had undergone cataract surgery with intraocular lens implantation in her right eye presented with complaint of blurring of vision of 6 months duration. She was on topical ketorolac tromethamine 0.5% (Acular, Allergan Inc, US) eye drops 3 times a day. Past medical history was significant for hypertension for which she was on antihypertensive medications. On examination her best-corrected visual acuity (BCVA) was 20/60 in her right eye and 20/20 in the left eye. Anterior segment examination revealed a clear cornea, a Kelman style anterior chamber intraocular lens and a patent peripheral iridectomy. Anterior chamber was quiet and there was no evidence of prolapsed vitreous. Dilated fundus evaluation revealed a thickened macula with presence of cystoid spaces. There was no associated vitreous inflammation or disc edema. Stratus OCT (Zeiss Inc. USA) scan of the fovea revealed cystoid changes with retinal thickening. However, delineation of individual layers of retina on Stratus OCT is limited due to poor resolution (Fig. 1). SD-OCT (Spectralis, Heidelberg Engineering, Germany) showed an increased thickness of the fovea and presence of large cystoid spaces in the outer plexiform layer with stretching of the Muller cell processes (Fig. 2). The central subfield thickness (CST, an area with a diameter of 1 mm centered at the fovea) was 500 microns, volumetric measurement was 0.36 mm3. Photoreceptor layer (as represented by inner segment-outer segment line [IS-OS line]) was intact and the continuity of the external limiting membrane (ELM) was maintained. The patient was diagnosed to have pseudophakic CME and intravitreal 4 mg of intravitreal triamcinolone actetonide (Kenalog, Allergan) was administered. 3 months later, the patient's BCVA was 20/20 and a repeat SD-OCT showed reduction in foveal thickness (CST measurement was 224 microns and volumetric measurement was 0.25 mm3 and return of normal foveal contour (Fig. 3).

Stratus OCT cross-sectional image of the fovea revealing an increase in foveal thickness and presence of cystoid spaces.
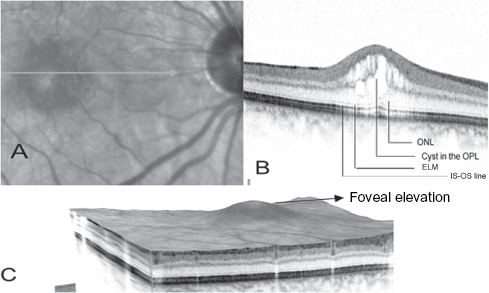
A) Infrared image of the right of the patient showing cystic spaces at the fovea.

A) Infrared image of the right of the patient showing resolution of the edema.
Discussion
The incidence of CME after uncomplicated cataract surgery as detected by fluorescein angiography is 20%. However it is visually significant in only 1% of cases. 1 3 The development of macular edema is a result of breakdown of blood-retinal barrier secondary to persistent inflammation. Vascular endothelial growth factor (VEGF) has been found to play a limited role in the pathogenesis.2,3 The resultant fluid accumulation occurs in the outer plexiform layer which shows intracellular swelling. With progressive accumulation of fluid, cystic changes occur and as these cystoid spaces enlarge, they involve the adjoining nuclear layers. The cystoid spaces at the fovea transform the pit into a central mound causing an increase in retinal thickness. 5
Retinal thickness measured with the optical coherence tomography is an important indicator for prognosticating visual outcomes following treatment for macular edema. 6 Occasionally, poor visual outcomes are noted after effective treatment in spite of normal foveal contour on time-domain Stratus OCT. 7 Location of cyst within the fovea, whether outer, central, or inner, and integrity of the IS-OS line, which has been reported to correspond to the reflection derived from the junction between inner and outer segments of the photoreceptor layer, are prognostic factors in predicting visual outcomes after resolution of macular edema. 8 However, since time domain OCT had constraints of resolving the retinal images beyond a particular point, it was difficult to analyze the ultrastructural changes associated with cystoid macular edema. SD-OCT, an important advance in OCT technology, acquires upto 40000 A-scans in a short period of time and renders a 3-dimensional image with cross-sectional sections providing detailed ultrastructural changes within the retina. 4 The changes seen on SD OCT in our case included a large cyst in the outer plexiform layer, increased thickness of the outer nuclear layer and intact IS-OS line that corresponded to the changes described histologically.
Anti-inflammatory therapy including topical NSAIDs and corticosteroids administered in a stepwise approach is the mainstay of treating postoperative CME. Resistant cases required the use of peribulbar steroids to achieve high concentrations near the macula. In the rare case, intravitreal steroid is required for the resolution of CME.2,3 In our case, we used intravitreal triamcinolone actetonide after the edema was persistent after a trial of topical NSAIDs. SD-OCT demonstrated the return of the normal foveal contour and thickness one month after treatment.
In summary, SD-OCT is a useful tool in identifying the ultrastructural changes associated with CME after cataract surgery and in monitoring response to treatment.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.