
Abstract
We evaluated the effect of intravitreal bevacizumab (IVB) injection before pars plana vitrectomy (PPV) on intravitreal hemorrhage (VH) during and after vitrectomy for postoperative the first day and the first month in pseudophakic patients with proliferative diabetic retinopathy (PDR). This retrospective study was performed on 44 eyes of 44 patients who underwent vitrectomy for PDR. Patients were divided into PPV (n = 22 eyes) and PPV + IVB (n = 22 eyes) groups. Injection of bevacizumab (1.25 mg/0.05 mL) was performed 3 days before vitrectomy. Outcomes of visual acuity as well as intraoperative and postoperative VH were compared between the two groups. One month after surgery, visual acuity improved in PPV and PPV + IVB groups (
Introduction
Intravitreal hemorrhage (VH) during vitrectomy and postoperative rehemorrhage into the vitreous are common complications in patients with proliferative diabetic retinopathy (PDR). Intravitreal hemorrhage, preretinal fibrovascular membranes, and tractional retinal detachment are the major causes of decreases in vision in patients with PDR. 1 Pars plana vitrectomy is used to remove VH, preretinal membranes, and relieve vitreoretinal tractions. 2 Bevacizumab is a recombinant monoclonal antibody against vascular endothelial growth factor (VEGF) and was approved by the US food and Drug Administration (FDA) for treating colorectal cancer. Intravitreal bevacizumab (IVB) has been used for choroidal neovascularization secondary to age-related macular degeneration (AMD), 3 proliferative diabetic retinopaty (PDR),4,5 rubeosis iridis (RI),6,7 and macular edema (ME) secondary to diabetic retinopathy (DR) or retinal vein occlusion (RVO). 8 13 The aim of this study was to examine the effect of IVB before vitrectomy on VH during and after vitrectomy in pseudophakic patients with PDR.
Methods
Data for patients who underwent pars plana vitrectomy (PPV) and PPV with IVB injection 3 days before vitrectomy were reviewed. Preoperative values for best corrected visual acuity (BCVA, decimal), intraocular pressure (IOP), and records of intraoperative VH and postoperative BCVA (decimal), IOP, VH, retinal detachment, and endopthalmitis at 1 month were analyzed.
This study included pseudophakic diabetic patients who had preretinal fibrovascular membranes involving or threatening the macula, PDR associated rubeosis iridis, massive preretinal bleeding covering the posterior pole, and BCVA of ≤0.1. Patients with pregnancy, phakic, history of hemodialysis, retinal vein occlusion, history of IVB injection, optic atrophy, behcet disease, trauma, and history of vitrectomy, break/s of retina, use of gas, silicon oil or air the end of vitrectomy, preoperative BCVA of ≥0.1 were excluded.
Patients were divided into 2 groups. The PPV group included 22 eyes of 22 patients (8 male, 14 female); the PPV + IVB group included 22 eyes of 22 patients (10 male, 12 female) undergoing PPV from January 2008 to December 2012. The mean age was 58.8 ± 9.0 years in the PPV group and the mean age was 60.7 ± 7.8 years in the PPV + IVB group (Table 1). All patients had type 2 diabetes mellitus and had no treatment with panretinal photocoagulation. However, panretinal photocoagulation was performed intraoperatively or during the first month after surgery.
Demographic characteristics, preoperative fasting glucose level, HbA1c, and follow-up time.

Statistical value
Bevacizumab was injected 3 days before PPV at a dose of 1.25 mg/0.05 ML (Avastin; South San Francisco, CA, USA) injected into the vitreous body using a 27-gauge (g) needle 3.5 mm posterior of the limbus at the inferotemporal area in the operating room.
Central macular thickness (CMT) was measured by optical coherence tomography (OCT) pre- and post-operatively at one month in patients who had no VH.
Standard three port PPV was performed using 23-gauge (g) vitrectomy systems (Alcon Lab, Inc., Fort Worth, TX, USA) in all patients. Preretinal membranes were peeled using scissors, a pick, or the vacuum mode of vitrectomy systems. Triamcinolone acetonide was used in all cases for visualization of the vitreous. The internal limiting membrane was not peeled.
Patients were examined before surgery and at 1, 7 days and 1 month after surgery. Values for the two groups were compared used their data of preoperative, intraoperative, and postoperative at 1 day and 1 month. The study was approved by the local ethics committee. The study performed according to the tenets of the Declaration of Helsinki. All patients gave their written informed consent before participating in the study.
Mean measurements were expressed as the mean ± standard deviation (SD). Mean BCVA (baseline and at 1 month), IOP (at baseline and at 1 month), and VH (at 1 day and at 1 month) were compared. SPSS 10.0 software was used for evaluation. The 2-sample
Results
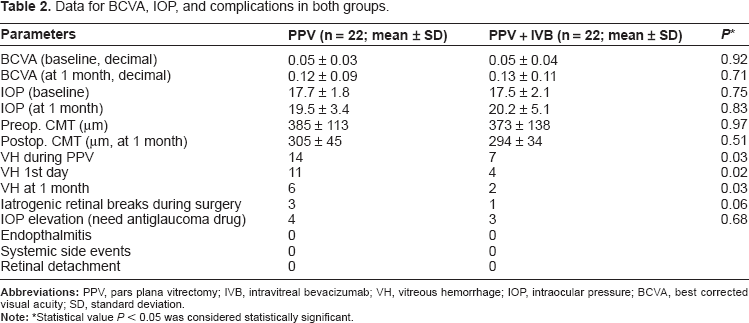
In the PPV group; final BCVA showed improvement in 15 eyes (68.2%), stabilized in 4 (18.2%) eyes and decreased in 3 (13.6%) eyes after surgery at one month. The mean baseline BCVA was 0.05 ± 0.03 and mean postoperative BCVA was 0.12 ± 0.09 at one month (
Intraoperative VH occurred in 14 eyes, with postoperative VH recorded in 11 eyes on the first postoperative day; VH was recorded in six eyes at 1 month. In five eyes, VH was cleared spontaneously during the first postoperative month. Iatrogenic retinal breaks during surgery were recorded in 3 eyes.
In the PPV + IVB group, final BCVA showed improvement in 19 eyes (86.4%), no change in one (4.5%) eye, and decrease in two (9.1%) eyes. The mean baseline BCVA was 0.05 ± 0.04 and mean postoperative BCVA was 0.13 ± 0.11 at 1 month. Intraoperative VH occurred seven eyes. VH was recorded in 4 eyes on the first day and in 2 eyes at 1 month. During the first month after surgery, VH was cleared spontaneously in 2 eyes. Iatrogenic retinal break/s was/were recorded in one eye during surgery. The BCVA was ≥0.1 in 14 eyes at one month.
Patients who received retinal tamponade (silicon oil, gas or air) were excluded, so the level of BCVA was not affected by the tamponade. Elevated IOP (>21 mmHg) was recorded in 4 eyes in the PPV and in 3 eyes in the PPV + VB group (
Pre- and postoperative values in mean BCVA and IOP were similar in both groups (Table 2). Mean preoperative CMT values were 385 ± 113 and 373 ± 138 μm (
Data for BCVA, IOP, and complications in both groups.
Statistical value
Discussion
VEGF has been shown to contribute significantly to PDR. Increased production of VEGF produced by retinal pigment epithelium (RPE) cells, pericytes, and endothelial cells secondary to ischemia can be blocked by retinal laser photocoagulation by decreasing the ischemic area. IVB blocks the effect of VEGF on receptors and inhibits retinal new vessels and cells in neovascular membranes.14,16 IVB has potent anti-angiogenic effects and has been shown to cause regression of neovascularization. 17
The effects of IVB in patients with neovascularization elsewhere in the retina secondary to PDR have been evaluated in a number of studies. Fluorescein angiography revealed a reduction of leakage from the foci of neovascularization elsewhere in the retina secondary to PDR or neovascularization of the optic disc. 18 A study reported regression of neovascularization in eyes with active progressive PDR. 19 Preoperative IVB made the surgery much easier by decreasing the activity of new vessels and causing less bleeding during removal of the proliferative membrane. 20
This study revealed that IVB reduces the rate of VH during and after PPV in patients with PDR. This study showed that IVB is helpful for limiting fibrovascular proliferation before vitrectomy, making surgery easier.
Injection of IVB before vitrectomy also decreased surgical time. 21 Intraoperative VH is an important complication associated with PDR in PPV. 22 We determined VH by direct observation during surgery and found VH in 14 eyes in the PPV group. Removal of the hemorrhage may not only create iatrogenic breaks but also extend the breaks, resulting in significantly more bleeding. In some instances, surgery cannot continue due to the hemorrhage and a second surgery is required. Often, surgery with intraoperative bleeding shows an increased risk of postoperative hemorrhage. It has been suggested that IVB is useful for avoiding hemorrhage. VH occurred less frequently in the PPV + IVB group than in the PPV group. The use of IVB reduced intraoperative hemorrhage and made the surgery technically easier.18,23,24 A previous study found no effect of IVB before vitrectomy. 25
Recently, two studies found excellent clinical outcomes with IVB pretreatment in vitrectomy in patients with severe diabetic retinopathy.26,27
IVB was found to be safe and effective for reducing the incidence of recurrent postoperative VH. 28 This study showed that preoperative IVB caused less intraoperative and postoperative VH. Preoperative IVB injection was found to be a good strategy for the after-surgery period. 29 IVB injection before vitrectomy for PDR facilitates the surgery and decrease postoperative VH. 30 IVB injection 1 week before surgery reduced the incidence of postvitrectomy VH in diabetic patients. 31 In this study IVB injection was performed 3 days before surgery. Postoperative VH was reported in 6 eyes in the PPV group and in 2 eyes in the PPV + IVB group at one month. The sources of hemorrhage are often difficult to locate at the time of surgery. The results of this study showed that the ratio of re-hemorrhage into the vitreous was low in the PPV + IVB group. IVB prevented recurrence of VH in the early postoperative period. Injection of IVB into the vitreous decreased VH by blocking VEGF activity for 4 weeks, although some studies showed better visual results than this study. This study did not include eyes with preoperative cataract or lenticular opacification. Several studies included patients that had undergone phacoemulsification with PPV, in which a consequent increase in BCVA was expected. No observed systemic or ophthalmologic side effect/s of IVB in either group.
The limitations of this study were its retrospective design, small sample size, and lack of comparison of fluorescein angiography for baseline and after vitrectomy.
In summary, preoperative IVB injection was helpful for reducing intraoperative VH and postoperative VH complications in patients with PDR.
Author Contributions
Analyzed the data: MD, OK. Wrote the first draft of the manuscript: MD, EC. Contributed to the writing of the manuscript: EC, OK. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: All authors. Made critical revisions and approved final version: All authors. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.