
Abstract
Vitreoretinal surgery has advanced extensively from the first days of vitrectomy. During the last decade, new developments in intravitreal pharmacotherapy have created new opportunities to enhance the surgical outcomes of our patients. In this article, we review and discuss some of the supporting evidence of different pharmacotherapies that may be used as an adjunct to vitrectomy for select common etiologies. Triamcinolone acetonide, dexamethasone, and angiogenesis inhibitors are among the most commonly used drugs given their safety profile and proven efficacy. Other pharmaceuticals have also shown promising results in small studies. The adoption of individualized medical treatments prior, during, and after vitrectomy will continue to increase as new evidence supporting the benefit of pharmacotherapy as an adjunct to vitrectomy becomes available.
Keywords
Introduction
Vitreoretinal surgery has advanced extensively from the first days of vitrectomy during the early 1970s when Dr Robert Machemer performed the first vitrectomy. Today, retinal surgeons have access to a wide variety of microincision vitrectomy surgery instrumentation, a myriad of intraocular implants such as multidensity silicone oil, perfluorocarbon liquids, and various gases for endotamponade. Similarly, during the last decade, new developments in intravitreal pharmacotherapy have created new opportunities to enhance the surgical outcomes of our patients.
In this article, we review and discuss some of the supporting evidence of different pharmacotherapies that may be used as an adjunct to vitrectomy for select common etiologies.
Methods
Data extraction was conducted through keyword search containing ‘diabetic retinopathy’, ‘proliferative vitreoretinopathy’ (PVR), and ‘epiretinal membrane’, in conjunction with ‘triamcinolone acetonide’, ‘dexamethasone’, ‘angiogenesis inhibitor’, or ‘pharmacotherapy’. English articles in PubMed with a publication date including or after 1979 were considered. Qualitative synthesis was used to integrate information. A total of 42 articles were reviewed for the discussion.
Diabetic retinopathy
Triamcinolone acetonide
Historically, triamcinolone acetonide has been used to suppress inflammatory mediators associated with multiple retinopathies including diabetic retinopathy. During the early days of vitrectomy, Dr Machemer used triamcinolone acetonide for diabetic retinopathy and was the first to describe in experimental animal studies the decreased duration of triamcinolone acetonide in eyes that underwent vitrectomy.1,2
The Diabetic Retinopathy Clinical Research Network investigated the efficacy of intravitreal triamcinolone acetonide for diabetic retinopathy and found regression of retinopathy scores and decreased macular edema. 3 These effects were not seen with subtenon therapy. However, triamcinolone acetonide monotherapy was limited due to intraocular pressure elevation and the progression of cataracts. This concept has continued to encourage surgeons to use triamcinolone acetonide to suppress postsurgical inflammation and treat diabetic retinopathy.
A prospective multicenter randomized study that compared intravitreal injection of triamcinolone acetonide at the end of vitrectomy versus vitrectomy alone in subjects with vitreous hemorrhage due to proliferative diabetic retinopathy was recently performed. 4 There was a significant decrease in central macular thickness in the acute postoperative period in subjects who were treated with triamcinolone acetonide at the end of vitrectomy when compared with vitrectomy alone. No differences in intraocular pressure, visual acuity, or recurrence of hemorrhage were detected. This study suggests superior postsurgical inflammatory control with intravitreal triamcinolone acetonide in eyes with diabetic retinopathy compared with vitrectomy alone.
Similarly, a prospective, randomized clinical trial that included 72 consecutive subjects undergoing pars plana vitrectomy for treatment of diabetic nonclearing vitreous hemorrhage found better visual acuity and lower rates of recurrent vitreous hemorrhage at 6 months after surgery compared with controls. 5 This study concluded that intravitreal triamcinolone acetonide reduced rebleeding in eyes undergoing pars plana vitrectomy for the treatment of diabetic vitreous hemorrhage.
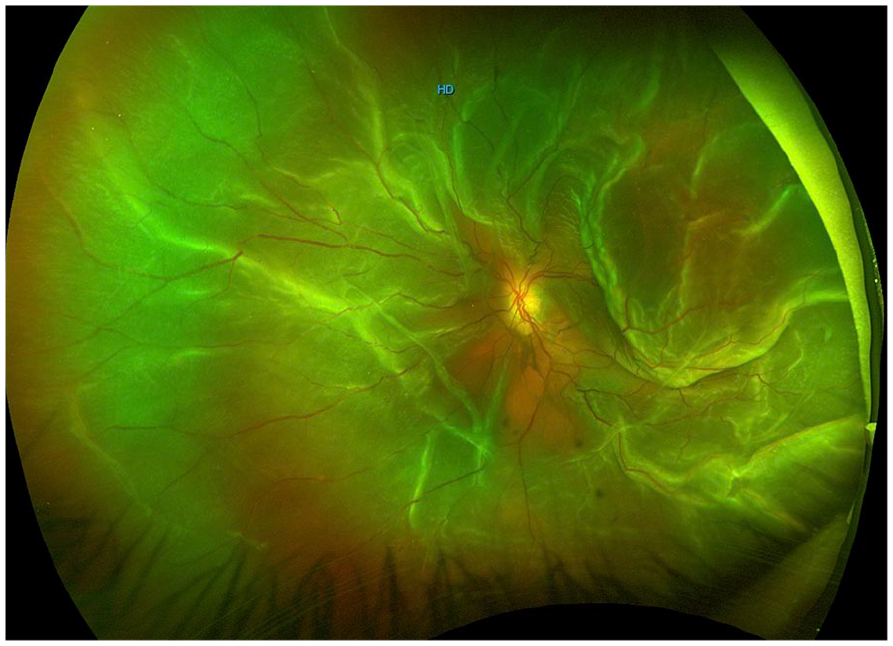
Most recently, a prospective cohort study performed in Japan evaluated the effect of triamcinolone acetonide on retinochoroidal thickness after pars plana vitrectomy combined with scatter photocoagulation in subjects with proliferative diabetic retinopathy. 6 Eyes underwent vitrectomy alone or with either subtenon or intravitreal triamcinolone acetonide at the end of vitrectomy. Eyes that underwent subtenon or intravitreal therapy with triamcinolone acetonide showed significantly less retinochoroidal edema compared with vitrectomy alone. No significant intraocular pressure increase was documented. Other studies, including retrospective case studies and nonrandomized clinical trials, have also reported similar positive outcomes when triamcinolone acetonide is used at the end of vitrectomy in patients with diabetic retinopathy (Figures 1 and 2).7,8

Ultra-widefield fundus photograph of the right eye in a patient with proliferative diabetic retinopathy and tractional retinal detachment (TRD).

(a) Macular SD-OCT prior to surgery (BCVA 20/800). (b) Macular SD-OCT after vitrectomy with retinal detachment repair and intravitreal injection of triamcinolone acetonide at the end of vitrectomy (BCVA 20/25).
Dexamethasone
The slow-release dexamethasone implant has also become a common pharmacotherapy in the clinic for many retina specialists. However, new research has demonstrated positive outcomes when combined with vitrectomy in diabetic patients.
A recent nonrandomized controlled trial that evaluated 13 subjects who underwent pars plana vitrectomy for tractional and nontractional refractory diabetic macular edema (DME) found a statistically significant improvement in visual acuity and central macular thickness in both tractional and nontractional DME. 9 The study concluded that vitrectomy combined with intraoperative dexamethasone implant may be safe and effective in treating DME, especially when associated with traction.
A previous similar retrospective observational study that evaluated 62 subjects who underwent vitrectomy with concomitant dexamethasone implant for DME, retinal vein occlusion, and noninfectious posterior uveitis had improvement in central foveal thickness and best-corrected visual acuity up to 1 year. 10 Transient intraocular pressure elevation was most common during the first week, especially in uveitic subjects. Other interventional case series studies evaluating the safety of vitrectomy and intravitreal dexamethasone implant have had similar positive visual outcomes.11,12
Angiogenesis inhibitors
Anti–vascular endothelial growth factor (anti-VEGF) agents have undoubtedly revolutionized the care of patients with retinovascular disease, especially diabetic retinopathy. Many retina specialists currently use intravitreal anti-VEGF routinely for hemostasis prior to surgery. However, there is still debate among clinicians about the best timing, medication, and dosage. 13
A prospective randomized study that evaluated 206 subjects who underwent intravitreal bevacizumab for proliferative diabetic retinopathy at three different doses (0.625 mg versus 1.25 mg versus 2.5 mg) found that higher doses of intravitreal bevacizumab correlated with higher rates of preoperative TRDs. 14 No differences in final best-corrected visual acuity, postoperative complications, or unplanned reoperations were found. Therefore, low doses of intravitreal bevacizumab may minimize morbidity. Newer and more potent preoperative anti-VEGF agents may be used with caution.
Another recent randomized clinical trial that was designed to assess the optimal interval of preoperative intravitreal bevacizumab administration in diabetic subjects undergoing pars plana vitrectomy for severe manifestations of active proliferative diabetic retinopathy was undertaken. 15 All subjects underwent treatment with intravitreal bevacizumab 2.5 mg/0.1 mL; however, they were randomized into two groups: administration 1–3 days versus 5–10 days prior to vitrectomy. There were no significant differences with regard to baseline features, intraoperative time, intraoperative complications, and incidence of unplanned vitrectomy during the study interval. Both treatment groups had a significant improvement in visual acuity at 6 months. However, the group of patients who received intravitreal bevacizumab 5–10 days before vitrectomy had less incidence of recurrent vitreous hemorrhage after vitrectomy at 6 months. A possible explanation for this is that preoperative intravitreal bevacizumab administered 1–3 days before vitrectomy may not allow enough time to effectively regress neovascularization, compared with intravitreal bevacizumab performed 5–10 days before vitrectomy.
In fact, a recent meta-analysis supports these findings. 16 The study compared the efficacy of the different perioperative time-points of anti-VEGF administration reported in the literature. They concluded that administration 6–14 days prior to pars plana vitrectomy showed the best efficacy in improving visual acuity and reducing incidence of recurrent vitreous hemorrhage since this interval allows significant regression of neovascularization. Nonetheless, Russo et al. 17 showed in a retrospective cohort that when the injection was given more than 10 days before vitrectomy, the rate of tractional macular detachment increased significantly. Based on this, one may conclude that an interval of 5–10 days is adequate to provide hemostasis without compromising anatomical structure.
Anti-VEGF agents may also be used at the end of surgery to minimize postsurgical vitreous hemorrhage. A retrospective case study that compared intravitreal bevacizumab versus triamcinolone acetonide at the end of vitrectomy for subjects with proliferative diabetic retinopathy and vitreous hemorrhage with or without TRD found positive anatomical and visual outcomes compared with controls that did not receive any intravitreal pharmacotherapy at the end of surgery. 7 The rate of postoperative vitreous hemorrhage after surgery was higher in the control group versus both treatment groups. No significant difference was found regarding best-corrected visual acuity and reoperation rates among all groups. The study concluded that intravitreal bevacizumab and triamcinolone were useful adjunctive therapy for reducing early postoperative vitreous hemorrhage.
Proliferative vitreoretinopathy
Triamcinolone acetonide
Despite vast advances in surgical techniques, a major complication after rhegmatogenous retinal detachment repair continues to be the development of PVR (Figure 3). It has been postulated that inflammatory mediators that develop after an anatomical injury to the retina and retinal pigment epithelium lead to the development of vitreous, epiretinal, and subretinal membrane proliferation. Animal studies have demonstrated a statistically significant decrease in the development of PVR with intravitreal triamcinolone and methylprednisone.18,19
Primary rhegmatogenous retinal detachment with grade C proliferative vitreoretinopathy.
A recent retrospective interventional case series evaluated the effect of low-dose (2 mg) triamcinolone acetonide as adjuvant to vitrectomy with silicone oil tamponade. Of the 37 eyes with grade C or D PVR, 84% had an improvement in visual acuity after a mean follow-up of 23 months. 20 Only one eye had loss of visual acuity from baseline. The study concluded that intravitreal triamcinolone acetonide was effective and safe in treating PVR grade C or D. Another small retrospective case series had similar outcomes. 21
The largest prospective randomized controlled clinical trial evaluating the effectiveness of intravitreal triamcinolone acetonide for PVR grade C enrolled 75 subjects. 22 Eyes underwent vitrectomy with silicone oil tamponade with or without 4 mg of intravitreal triamcinolone acetonide at the end of surgery. Retinal reattachment without any reoperation was achieved in 84% of eyes in the treatment group versus 78% in the control group at 6 months. Although the difference was not statistically significant, there was a trend for better anatomical outcomes in eyes treated with intravitreal triamcinolone acetonide.
Dexamethasone
Recently, a single-center, prospective, randomized study was performed to evaluate slow-release dexamethasone implant for PVR. 23 A total of 140 subjects with grade C PVR were enrolled in the study and were treated with pars plana vitrectomy and silicone oil tamponade with or without the dexamethasone implant at the end of surgery. No differences were detected in redetachment rates or visual acuity. Retinal attachment was less than 50% in both arms of the study. Although the study concluded that the dexamethasone implant did not improve redetachment rates, both arms of the study had poor anatomical outcomes compared with historical controls.
Methotrexate
Given its anti-inflammatory properties, systemic and intraocular methotrexate have been used successfully for the treatment of various ocular diseases. Adverse reactions to intraocular methotrexate have been reported previously in the past and include corneal epitheliopathy, corticosteroid-responsive sterile endophthalmitis, and intravitreal hemorrhage. 24 However, more recent case series have demonstrated an excellent safety profile with no significant adverse reaction observed.25–27
A recent retrospective cohort study was performed to evaluate the effects of repeated intrasilicone oil injections of methotrexate on the outcomes of surgery for rhegmatogenous retinal detachment with grade C PVR. 28 Eleven subjects were included in the study with a mean follow-up of 3 months. Two intravitreal injections were performed at 3 and 6 weeks after surgery. All eyes were attached at the end of the follow-up period. No ocular or systemic adverse effects were documented. Repetitive intravitreal methotrexate may be a reasonable clinical strategy in high-risk PVR. Other recent studies with intravitreal methotrexate for PVR have had positive anatomical and visual outcomes.25,26
Antiproliferative agents
Antiproliferative drugs have also been used in the treatment of PVR to control the mitogenic activity of cells at the vitreoretinal interface. A recent prospective noncomparative case series that evaluated 16 consecutive eyes with perforating choroidal injury was performed to investigate the potential role of mitomycin C in preventing PVR in eyes with open globe trauma. 29 Postoperative PVR developed in 3% of subjects. There were no adverse events associated with mitomycin C after a 2-year follow-up. The study suggests that intraocular application of mitomycin C may have a potential role in reducing the rate of post-traumatic PVR and improving anatomical and functional outcomes in eyes with perforating, deep choroidal, foreign body injuries. Other chemotherapeutic agents (e.g. daunorubicin, fluorouracil with or without heparin) have also been used with inconsistent results.30,31
Wiedemann et al. 30 reported decreased reoperation rates in patients treated with adjuvant daunorubicin; however, whether this association was due to daunorubicin use or due to the surgical technique employed remains unclear. Kumar et al. 31 randomized 30 patients with Stage D1 or worse PVR to receive an intravitreal injection of daunorubicin (5 mg) or no additional treatment at the conclusion of retinal surgery. However, no significant difference in attachment rate was observed at 3 months. Additional randomized trials are needed to clarify the role of daunorubicin as an adjunctive treatment.
Asaria et al. studied the effect of using 5-fluorouracil in combination with low-molecular-weight heparin as adjunct to vitrectomy in patients with retinal detachment and high-risk factors for developing PVR. In their randomized clinical trial, the incidence of PVR was significantly lower in the study group (5-fluorouracil in combination with low-molecular-weight heparin) (12.6%) than in the placebo group (26.4%). 32 This study supports the prophylactic use of these medications in patients with high-risk characteristics of developing PVR.
A recently investigated drug for the prevention and/or treatment of PVR is decorin, a small proteoglycan with inhibitory effects over the cytokine transforming growth factor-β (TGF-β). 33 This inhibitory effect is of particular interest because TGF-β plays an important role in the formation of fibrous membranes found in PVR. A recent experimental animal study reported the effects of adjuvant decorin use during vitrectomy in a rabbit model of PVR. 34 Severe PVR with TRD was reported in 80% of the control eyes versus in 6–13% of the treated eyes. They concluded that decorin effectively reduced fibrosis and TRD development and as such had potential for prevention of PVR. No obvious toxicity concerns were reported in this study; however, a subsequent pilot study was undertaken to investigate the safety profile of this drug on human eyes. In this interventional case series, 12 eyes with perforating injuries were injected 48 h after injury with either 200 µg/0.05 mL or 400 µg/0.1 mL of decorin. 35 The authors reported no short-term safety concerns after a single intravitreal injection of decorin with no reported systemic or ocular adverse effects in any of the subjects. Some of the limitations of this study were its considerably small sample size and the absence of a control group; thus, larger randomized studies are needed to establish a better understanding of this drug’s safety and efficacy.
Finally, the role of low-dose, oral isotretinoin for PVR prophylaxis following rhegmatogenous retinal detachment repair has also been studied. 36 A prospective cohort study that evaluated 109 subjects with PVR or at high risk of developing PVR was undertaken. Subjects were treated with 20 mg of oral isotretinoin in the experimental arm. The anatomical success rate after a single surgery was 78.4% in the experimental arm versus 70.0% in the control arm in eyes with PVR. Similarly, the anatomical success rate after a single surgery was 84.5% in the experimental arm versus 61.1% in the control arm in eyes with high risk of developing PVR. The study concluded that oral isotretinoin may reduce the risk of redetachment in eyes with primary rhegmatogenous retinal detachment and high-risk characteristics for the development of PVR.
Angiogenesis inhibitors
A recent meta-analysis evaluated the effect of intravitreal bevacizumab in vitrectomy for patients with PVR-related retinal detachment. 37 The study concluded that the differences in visual acuity and redetachment rates between the groups were not significant clinically or statistically. Intravitreal bevacizumab at the end of vitrectomy does not seem to have any benefits in eyes with rhegmatogenous retinal detachment.
Epiretinal membrane
Triamcinolone acetonide
Epiretinal membranes may arise from multiple mechanisms including posterior vitreous detachment, uveitis, and retinal vascular disease. Despite studies demonstrating significant anatomical and visual improvements after surgical removal of preretinal membranes, postoperative macular edema continues to limit optimal visual outcomes. Multiples authors have demonstrated the safety and efficacy of intravitreal triamcinolone acetonide during and after vitrectomy for complex retinovascular disease with or without preretinal proliferation (Figures 4 and 5).38–41

Ultra-widefield fundus photograph of the left eye in a patient with a vasoproliferative tumor and profuse epiretinal membrane formation.

(a) Macular SD-OCT prior to surgery (BCVA counting fingers). (b) Macular SD-OCT after vitrectomy, epiretinal membrane peeling, and intravitreal injection of triamcinolone acetonide at the end of vitrectomy (BCVA 20/60).
A retrospective case series evaluated the effects of the concomitant use of triamcinolone acetonide after pars plana vitrectomy for idiopathic epiretinal membranes. In this study, 75 subjects who received intravitreal therapy versus 49 subjects who underwent surgery without intravitreal therapy were compared. Evaluation 3 months after surgery showed a statistically significant difference between groups regarding best-corrected visual acuity and central macular thickness. The study concluded that anatomical and functional visual improvements are superior at 3 months with adjuvant intravitreal triamcinolone acetonide. 42
Dexamethasone
A retrospective consecutive case–control study was performed to compare the visual and anatomical outcomes of eyes undergoing pars plana vitrectomy and epiretinal membrane peel with the intraoperative use of the dexamethasone intravitreal implant versus triamcinolone acetonide. 43 Fifty-five subjects were analyzed in the study. There were no exclusion criteria regarding the etiology of the epiretinal membranes. There was no statistical difference between groups regarding best-corrected visual acuity and central macular thickness at 1 and 6 months. No significant adverse effects were reported. The study concluded that both agents were effective in improving vision and anatomical outcomes.
Angiogenesis inhibitors
A prospective case series study that evaluated the effects of intravitreal injection of bevacizumab at the end of vitrectomy for macular epiretinal membrane was undertaken. 44 Thirty-three eyes were enrolled in the study. Follow-up ranged from 3 to 14 months. No significant difference between groups was seen. Subjects that underwent concomitant therapy with intravitreal bevacizumab had decreased central macular thickness compared with controls. The study concluded that despite superior short-term anatomical outcomes, visual acuity improvements may not be detectable in subjects undergoing intravitreal bevacizumab as an adjuvant to vitrectomy with epiretinal membrane peel.
Conclusion
Currently, there is a myriad of pharmacotherapies that can be used before, during, and after surgery to enhance the surgical outcome of our patients. Triamcinolone acetonide, dexamethasone, and angiogenesis inhibitors are among the most studied drugs used for diabetic retinopathy, PVR, and epiretinal membrane. Besides the anatomical and functional benefit of these drugs, some have also been shown to decrease the operating time and reduce the rate of intraoperative complications. Based on the current literature, we recommend treating patients with diabetic retinopathy with low-dose intravitreal bevacizumab 5–10 days prior to vitrectomy. Studies have shown that modulating intraocular inflammation after surgery allows faster visual recovery, less macular edema, and decrease in inflammatory-related complications. Therefore, we recommend the use of corticosteroids at the end of vitrectomy for diabetic retinopathy, PVR, and epiretinal membrane peeling.
Individualized pharmacotherapy after vitrectomy remains an important component to optimize the long-term outcomes after surgery. As the field of vitreoretinal surgery continues to move forward, larger prospective studies will allow surgeons to have additional tools to improve vision and change lives.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.