
Abstract
We examined the concentrations of water-soluble vitamins in blood and urinary excretion of 22 patients with type 2 diabetes mellitus (type 2DM) and 20 healthy control participants. Macronutrient and vitamin intakes of type 2DM subjects were measured using a weighed food record method. Control participants consumed a semipurified diet for eight days. Multiple linear regression models were used to determine whether significant differences existed in vitamin concentrations in blood independent of age, sex, and other confounding factors. Concentrations of vitamins B2, B6, C, niacin, and folate in blood were significantly lower in type 2DM subjects than in controls, independent of confounding factors. Renal clearances of vitamins B6, C, niacin, and folate were significantly higher in type 2DM subjects than in controls. In conclusion, concentrations of vitamins B2, B6, C, niacin, and folate in blood were significantly lower in type 2DM subjects than in controls, independent of confounding factors; based on the evidence of increased urinary clearance of these vitamins, the lower levels were likely due to impaired reabsorption processes.
Keywords
Introduction
Type 2 diabetes mellitus (DM) was previously considered to be a disease of Western countries but has now become a worldwide issue. The International Diabetes Federation reported that DM affects at least 285 million people globally, and that the number is expected to reach 438 million by the year 2030, with two-thirds of all DM cases occurring in low- to middle-income countries. 1 Asia accounts for 60% of the world's diabetic population. Asia has undergone rapid economic development, urbanization, and transitions in nutritional status in recent decades, 2 which have led to a marked increase in the prevalence of DM within a relatively short time.
The percentage of patients with type 2 DM who die as a direct consequence of the disease, eg because of diabetic ketoacidosis, is small; mortality of patients with type 2 DM has mainly been attributed to its associated complications: microvascular diseases such as diabetic nephropathy or macrovascular diseases such as myocardial infarction and stroke.3,4 Increasing evidence has shown the importance of prediabetes and family history of DM in the increasing cardiovascular (CV) risk profile of the general population. 5 In spite of the availability of extensive treatments for hyperglycemia, the risk of CV disease in patients with type 2 DM has not been sufficiently reduced.6,7 These findings have prompted the search for other metabolic and nutritional factors that may influence the development of vascular complications in patients with type 2 DM. Some studies have shown that the concentrations of several vitamins in blood were low in patients with type 2 DM,8,9 and supplement therapy with vitamin B1 or E has been found to be effective in preventing CV complications in patients with type 2 DM.10–13 Previous studies have focused on the concentration of a specific vitamin in patients with type 2 DM; the concentrations of water-soluble vitamins in blood and urinary excretion have not yet been comprehensively examined in patients with type 2 DM. Therefore, the aim of the present study was to comprehensively compare the concentrations of water-soluble vitamins in blood and urinary excretion in patients with type 2 DM and healthy control participants.
Methods
Participants
Patients with type 2 DM
Our study included patients with type 2 DM with significant comorbidities (renal insufficiency, those receiving insulin therapy, those with thyroid dysfunction, or those receiving warfarin). We invited 30 patients with type 2 DM, of whom 8 patients were excluded from the study because of missing data (dietary records, 24-hour urine, or data on blood chemistries). Thus, 22 patients (13 men and 9 women) with a mean age of 58.9 years (range 36-79 years) with type 2 DM who visited the outpatient clinic of Shiga University of Medical Science Hospital were enrolled in this study. All patients received full explanations of the study and gave informed consent. This part of the study was performed from August to December 2010. The protocol of this study was approved by the institutional review board of the Shiga University of Medical Science (No 22-42, 2010), and the research was performed in accordance with the Declaration of Helsinki.
Control participants
Healthy Japanese college students, 10 males and 10 females with a mean age of 20.7 years (range 19-23 years), served as the control group for the study. Prior to the experiment, they had physical checkups, and their hematological and blood biochemical analyses showed normal values. All participants received full explanations of the study and gave informed consent. This study was reviewed and approved by the ethical committee of the Incorporated Administrative Agency of Health and Nutrition. All participants were housed in the same facility for eight days. The daily schedule was partly restricted: the lights were turned off at 22:00 in order to promote sleep and the participants got up at 06:00. The precise experimental design is published elsewhere. 14 This part of the study was carried out from March 1 to March 8, 2002, for females, and from August 27 to September 3, 2002, for males.
Blood and urine sample collection
Patients with type 2 DM
Fasting blood was collected into ethylenediaminetetraacetic acid tubes. Whole blood and plasma samples were stored at -20°C for later analysis. Twenty-four-hour urine samples before the day of the blood examination were collected at home. Urine samples were stored in ice. After the volumes of the urine samples had been measured, the collected urine samples were immediately treated as described in the “Analyses of blood and urine vitamins” section in order to avoid the destruction of water-soluble vitamins and then stored at -20°C for later analysis.
Control participants
The control participants’ 24-hour urine samples were collected from the second urinary excretion on day 7 to the first one on day 8. After the volumes of the urine samples had been measured, the collected urine samples were immediately treated as described in the “Analyses of blood and urine vitamins” section to avoid destruction of water-soluble vitamins and then stored at -20°C until needed. The blood was taken from a cubital vein at 08:30 on day 8 before breakfast, treated immediately to avoid destruction of water-soluble vitamins, and then stored at -20°C until needed.
Dietary assessment
Patients with type 2 DM
Food intake was recorded by each patient using a weighed food record method with supplemental use of photography at home. Instructions on weighing and taking photographs were given by a registered dietician. The validation of this method has been reported elsewhere. 15 The daily intakes of macro- and micronutrients by each patient were calculated using software (Excel Eiyokun version 4.5, Kenosha, Inc.) based on the fifth revised and enlarged edition of the Standard Tables for Food Composition in Japan.
Control participants
The breakfast time was 08:00-09:00, lunch 12:30-13:10, and dinner 18:30-19:00. Subjects consumed a semipurified diet based on Japanese Dietary Reference Intakes. 16 The composition and amount of the semipurified diet are published elsewhere. 14
Chemicals
Thiamine hydrochloride, riboflavin, pyridoxine hydrochloride, pyridoxal phosphate monohydrate, cyanocobalamin, nicotinamide, folate, and L (+)-ascorbic acid were purchased from Wako Pure Chemical Industries. 4-Pyridoxic acid (4-PIC) was synthesized by ICN Pharmaceuticals and obtained from Wako Pure Chemical Industries.
Analyses of blood and urine vitamins
The concentrations of total vitamin B1 in whole blood and urine were measured by the high-performance liquid chromatography (HPLC)-postlabeled fluorescence method of Kimura et al.
19
The concentration of total vitamin B2 in whole blood was determined by the HPLC–lumiflavin method of Ohkawa et al,
20
with slight modifications. The concentration of vitamin B2 in urinary excretion was analyzed according to the method of Ohkawa et al.
21
Pyridoxal phosphate (a coenzyme of vitamin B6) in plasma was determined using the HPLC method.
22
4-PIC, a catabolite of vitamin B6, was measured in urine by the HPLC method.
23
Concentrations of vitamin B12 in plasma and urine were assayed by the microbiological method with
Vitamin clearances
Vitamin clearances in milliliters per minute were calculated from concentrations of vitamins in 24-hour urinary excretion and blood.
Estimated glomerular filtration rate
Body surface area (BSA) was calculated using the following formula:
BSA = 0.007184 x body weight (kg)0.425 x height (cm)0.725. 30
Estimated glomerular filtration rate (eGFR) in patients with type 2 DM was calculated using the following equations:
eGFR (mL/min) = 194 x (BSA/1.73) x Cr-1.094 x age-0.287 (for men)
eGFR (mL/min) = 194 x (BSA/1.73) x Cr-1.094 x age-0.287 x 0.739 (for women) 31
Because concentrations of creatinine in serum in control participants were not available, eGFR was estimated at 100 mL/min.
Statistical analysis
SAS version 9.4 for Windows (SAS Institute) was used. The chi-squared test was used to compare dichotomous variables between patients with type 2 DM and controls. Student's
Results
Descriptive statistics
Characteristics of patients with type 2 DM and control participants are shown in Table 1. Mean age was higher in patients than in controls. Mean BMI was larger in patients than in controls. No significant difference was observed in the percentage of men between the groups. The duration of type 2 DM, use of statins, use of metformin, mean glycated hemoglobin (HbA1c), fasting blood glucose, creatinine, and eGFR in patients are also shown in Table 1.
Participant characteristics.

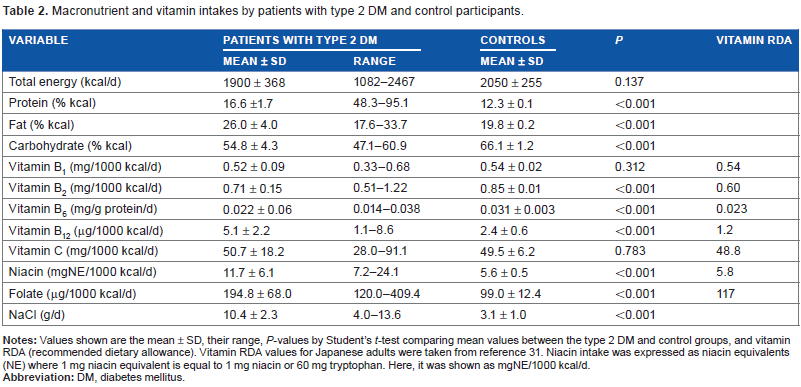
Macronutrient and vitamin intakes by patients with type 2 DM and controls are shown in Table 2. The recommended dietary allowance (RDA) values of the vitamins, as stated in 2010 by the Ministry of Health, are also shown in Table 2. 35 The mean values of vitamins B1, B2, B6, and C were approximately the same as the RDA values. Almost half of the patients with type 2 DM had intakes of these vitamins below the RDA values. Some patients’ intakes of vitamins B12 or folate were below the RDA values. Compared to controls, intakes in patients with type 2 DM of protein, fat, vitamin B12, niacin, folate, and NaCl were significantly higher; those of carbohydrates, vitamin B2, and vitamin B6 were significantly lower. Total energy intake and intakes of vitamin B1 and vitamin C were not different between the two groups.
Macronutrient and vitamin intakes by patients with type 2 DM and control participants.
Urinary vitamin excretion in patients with type 2 DM and controls
Urinary vitamin excretion in patients with type 2 DM and controls is shown in Table 3. Mean urinary excretion of vitamin B12 in patients with type 2 DM was significantly lower, and those of vitamin C and of total niacin catabolites were significantly higher, compared to control participants. The other values were not different between the two groups.
Urinary vitamin excretion in patients with type 2 DM and controls.

A catabolite of vitamin B6.
Sum of MNA, 2-Py, and 4-Py, which are the major catabolites of niacin. Urinary vitamin excretions in patients with type 2 DM and controls are shown as the mean ± SD with their ranges.
Concentrations of vitamins in blood in patients with type 2 DM and controls
The concentrations of vitamins in blood in patients with type 2 DM and controls are shown in Table 4. Without adjustments (Model 0), the concentrations of vitamins B1 and B12 in blood were higher, while those of the other vitamins were lower in patients with type 2 DM than in controls. With an adjustment for age (Model 1), the differences in the concentrations of vitamin B1 and B12 in blood between the two groups became nonsignificant. With further adjustments for age, sex, BMI, eGFR, urinary excretions of vitamin, and dietary intake of each vitamin (Model 2), the concentrations of vitamin B2, pyridoxal phosphate (a coenzyme of vitamin B6), vitamin C, niacin, and folate in blood remained significantly lower in patients with type 2 DM than in controls. Finally, with the addition of total energy intake to Model 2, the differences in the concentrations of vitamin C in blood between the two groups became nonsignificant. The concentrations of vitamin B2, pyridoxal phosphate (a coenzyme of vitamin B6), niacin, and folate in blood remained significantly lower in patients with type 2 DM than in controls. Since concentrations of folate in blood were significantly lower in patients with type 2 DM than in controls, a Model 3 analysis replacing an indicator for group (metformin use = 1, 0 otherwise) in patients with type 2 DM was performed. However, no significant difference was observed in concentrations of folate in blood between patients who were on metformin and those who were not (
Concentrations of vitamins in blood in patients with DM and controls.

Vitamin B12 concentrations were shown as median (25th, 75th percentile).
Vitamin clearances in patients with type 2 DM and controls
Vitamin clearances in patients with type 2 DM and controls are shown in Table 5. Mean clearance of vitamin B12 in patients with type 2 DM was significantly lower than that in controls. Mean clearances of vitamin B6, niacin, folate, and vitamin C in patients with type 2 DM were significantly higher than those in controls.
Vitamin clearances (mL/min) in DM and control.

Discussion
The main results of the present study were that among water-soluble vitamins, concentrations of vitamin B2, B6, niacin, and folate in blood were significantly lower in patients with type 2 DM than in controls, independent of age, BMI, dietary intake, eGFR, and other confounding factors. Despite reduced concentrations of these vitamins in blood, renal clearances of vitamin B6, niacin, and folate were significantly higher in patients with DM than in controls.
The concentrations of several vitamins in blood in patients with DM have been reported to be lower than normal.8,9 The lower concentrations of some vitamins in blood were attributed to enhanced renal clearances of these vitamins, possibly due to impaired reabsorption processes in patients with DM. Thornalley et al 8 reported that the renal clearance of vitamin B1 was 16-fold higher in patients with type 2 DM, and concentrations of vitamin B1 in plasma correlated inversely with the renal clearance of vitamin B1. Larkin et al 36 suggested that glucose-induced decreased expression of thiamine transporters in the tubular epithelium might mediate renal mishandling of thiamine in diabetes. However, Fukui et al 37 did not note any significant differences in the renal clearance of vitamin B1 between patients with type 2 DM and normal controls. Our results in the present study showed that the concentrations as well as renal clearances of vitamin B1 in blood in patients with type 2 DM were not significantly different from those in controls. However, mechanisms similar to those postulated by Thornalley et al 8 may be affecting reabsorption of other water-soluble vitamins in DM. Shibata reported that renal clearances of vitamin E and most water-soluble vitamins were higher in streptozotocin-induced diabetic rats than in controls, despite no higher concentrations of these vitamins in blood. 38 Although the concentration of vitamin C in blood in patients with type 2 DM became statistically nonsignificant compared to controls after an addition of total dietary energy intake in the final model, the possibility of over adjustment in analysis cannot be ruled out.
In addition to a higher clearance of niacin in patients with type 2 DM in the present study, a lower concentration of niacin in blood was also found; it is noteworthy that a previous study found the conversion rate of tryptophan to niacin markedly lower in diabetic rats induced by streptozotocin than in control rats. 39
Reductions in the concentrations of several vitamins in blood can be related to an increased prevalence of CV complications in patients with type 2 DM. Previous clinical studies and trials examined the benefits of vitamin supplemental therapy in DM for prevention of CV and/or other complications. The combination of vitamin B1 with B6, but not alone, has been shown to decrease DNA glycation in leukocytes of DM patients. 40 A six-month supplementation trial with a combination of vitamins B6, B12, and folate showed a decrease in retinal edema and an increase in light sensitivity in diabetic patients with nonproliferative retinopathy. 41 Concentrations of vitamin C in plasma have been inversely correlated with HbA1c and fasting and postprandial blood glucose and oxidative stress, but not to lipid profiles.42,43 Diabetes has also been associated with periodontal disease, and vitamin C supplementation together with dental treatment has been shown to improve chronic periodontitis in newly diagnosed type 2 diabetic patients. 44 A three-month supplementation of vitamins C and E decreased hypertension and blood glucose while increasing superoxide dismutase and glutathione levels. 45 Vittone et al examined the effects of niacin plus simvastatin on the progression of coronary stenosis in patients with metabolic syndrome as a subgroup analysis of the HDL-Atherosclerosis Treatment Study and found that the treatment with niacin plus simvastatin reduced changes in the mean proximal percent stenosis more than a placebo in participants with metabolic syndrome and in a more insulin-resistant group of participants. They also found that overall primary clinical events were 60% lower with niacin plus simvastatin than with a placebo. 46 Smulder et al 47 reported that homocysteine concentrations in type 2 DM were increased, even with modest deterioration of renal function or when the vitamin status was in the low to low-normal range, eg 20 pmol/mL for folate; higher than the mean concentration of folate in blood in patients with type 2 DM in the present study. They also showed that fasting homocysteine correlated with macrovascular diseases. Folate supplementation has been shown to lower homocysteine concentrations and may also improve endothelial function in patients with coronary artery disease. 48 Sudchada et al 49 performed a meta-analysis on the effects of folate supplementation in patients with type 2 DM. They screened 4 studies with 183 patients. Folate supplementation exerted significant effects on homocysteine levels. Although its effects on HbA1c levels were not significant, folate supplementation led to slightly better glycemic control than with a placebo. 49
A slight reduction in the intakes of these vitamins and increases in their renal clearances in patients with type 2 DM in the present study may have caused significantly lower concentrations of vitamin B2, B6, niacin, and folate in blood in patients with type 2 DM than in controls independent of confounding factors. These reductions in the concentrations of some vitamins in blood in patients with type 2 DM may be of clinical relevance, such as the future development of macrovascular diseases.
The strengths of the present study were: (1) the comprehensive measurement of blood, urine, and dietary intakes of water-soluble vitamins in patients with type 2 DM and healthy controls; and (2) the standardized collection of samples and high-quality laboratory measurements. The study was limited by its cross-sectional design; its results must be interpreted cautiously with regard to cause–effect relationships. The age ranges of patients and control participants differed and may have affected the results of statistical analyses. However,
In conclusion, concentrations of vitamin B2, B6, niacin, and folate in blood were significantly lower in patients with type 2 DM than in controls, independent of age and other confounding factors. These reductions in the concentrations of these vitamins in blood in patients with type 2 DM may be of clinical relevance in areas such as the future development of macrovascular diseases. Thus, changes in the management of patients with type 2 DM, including dietary adjustments and/or vitamin supplementation, may be warranted.
Author Contributions
Conceived and designed the experiments: HI, ToF, and KS. Analyzed the data: HI, YN, and TsF. Wrote the first draft of the manuscript: HI and YN. Contributed to the writing of the manuscript: HM, YD, and KS. Agreed with manuscript results and conclusions: HI, YN, ToF, TsF, SU, HM, YD, and KS. Jointly developed the structure and arguments for the paper: HI, YN, YD, and KS. Made critical revisions and approved final version: ToF, TsF, SU, and HM. All the authors reviewed and approved the final manuscript.