
Abstract
Aim
To assess serum Cu/Zn SOD (Superoxide Dismutase) concentration in autistic children and evaluate its possible relationship to GI Symptoms.
Subjects and Methods
Serum from 50 autistic children (31 with chronic digestive disease (most with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectal, small bowel and/or stomach) and 19 autistic children without GI disease), and 29 non autistic controls (20 age matched non autistic children with no GI disease and 9 age matched non autistic children with GI disease) were tested for Cu/Zn SOD using ELISAs.
Results
Serum Cu/Zn SOD levels of autistic children were significantly lower than all non autistic controls (p < 0.0001). Serum Cu/Zn SOD of autistic children with severe GI disease was significantly lower than autistic children with no GI disease (p < 0.0001), non autistic children without GI disease (<0.0001) and non autistic children with GI disease (p = 0.0003).
Discussion
These results suggest an association between Cu/Zn SOD serum levels and autism, particularly autistic children with GI disease, and that the concentration of serum Cu/Zn SOD may be a useful biomarker for autistic children with severe GI disease.
Introduction
Autism is a complex, behaviorally defined neurodevelopmental disorder characterized by social deficits, language impairments, and repetitive behaviors with restricted interests.
There has been a dramatic increase in the diagnosis of autism over the past decade. 1
While genes play a major role in the etiology, the cause of autism remains elusive, and is considered multifactorial, influenced by genetic, environmental, and immunological factors, as well as increased vulnerability to oxidative stress. No single gene has been found to be associated with autism, and involvement of multiple genes has been postulated.2–5 Environmental factors, such as mercury, lead, measles, rubella virus, retinoic acid, maternal thalidomide, valproic acid and alcohol use during pregnancy have been suggested to be involved in the etiology the disease,6–10 and behavioral impairments, gastrointestinal disturbances,11–15 epilepsy, 16 immune,3,17–19 autoimmune,20–22 and infectious factors8,9,23–27 have also been suggested to play role in autism pathophysiology.
In vivo, oxygen radicals are produced as byproducts of normal oxidative metabolism. 28 Hence, activated cells with increased metabolism produce more oxygen radicals. In addition, macrophages, which are phagocytic cells, produce and release reactive oxygen species (ROS) 29 in response to phagocytosis or stimulation with various agents. It has long been known that control of the intracellular redox environment is vital for proper cellular function. To protect themselves from the constant oxidative challenge, cells have developed defense mechanisms that ensure a proper balance between pro- and antioxidant molecules. 30 Cu/Zn superoxide dismutase (SOD-1) is a key enzyme in the dismutation of superoxide radicals resulting from cellular oxidative metabolism into hydrogen peroxide. 29
Increasing evidence suggests a role for oxidative stress in the manifestation of autism.31,32 In fact, oxidative stress has also been implicated in the pathogenesis of other neuropsychiatric diseases, including schizophrenia,33–35 major depressive disorder, 35 anxiety disorders such as panic disorder, 37 and obsessive-compulsive disorder. 38 It is probable that autism may result from an interaction between genetic, environmental, and immunological factors, with oxidative stress as a mechanism linking these risk factors.
Several studies have suggested that modifications in anti-oxidant enzymes may play a role in the etiology of autism. For instance, compared to controls, patients with autism showed decreased activity of glutathi-one peroxidase in plasma 39 and in erythrocytes,39,40 reduced levels of total glutathione, lower redox ratio of reduced glutathione (GSH) to oxidized glutathione (GSSG) in plasma, 41 and decreased catalase and SOD 39 activity in erythrocytes.
Zinc to copper ratio is abnormally low in individuals with autism42,43 and zinc is also antagonistic to copper absorption, and therefore zinc deficiency often occurs simultaneously with an excess of copper. 44 The loss of copper and zinc homeostasis is purportedly a likely indicator of a metallothionein deficiency. 43
Low zinc levels have been directly related to low Cu/Zn SOD concentration. 45 Because of this, we hypothesized that autistic children, particularly those with GI disease, would have abnormal levels of Cu/Zn SOD.
Materials and Methods
ELIsA to measure serum Ou/Zn sOD (Bender Systems)
All reagents and specimens were equilibrated to room temperature before the assay was performed. A 1:51 dilution of the patient samples was prepared by mixing 10 µl of the patient's sera with 0.5 ml of Serum Diluent. One hundred microliters of calibrators (0.08-2.5 ng/ml Cu/Zn SOD), serum diluent alone, and diluted patient samples were added to the appropriate microwells of a microculture plate (each well contained affinity purified polyclonal IgG to Cu/Zn SOD). Wells were incubated for 60 minutes (±5 min) at room temperature, then washed 4x with wash buffer. One hundred microliters of pre-diluter antihuman Cu/Zn SOD IgG conjugated with HRP was added to all microwells, incubated for 30 minutes (±5 min) at room temperature, then wash 4x with wash buffer. One hundred microliters of enzyme substrate was added to each microwell. After approximately 30 minutes at room temperature, the reaction was stopped by adding 50 µl of 1 M sulfuric acid, then the wells were read at 405 nm with an ELISA reader (BioRad Laboratories, Inc., Hercules, CA, USA).
Subjects
The diagnosis of autism for all subjects in this study was made using the standard Autism Diagnostic Interview-Revised (ADI-R) algorithm, and ASSQ assessment was used to exclude autism in controls.
GI pathology was determined through medical history data and, in the case of those with GI disease, through endoscopic diagnosis.
Experimental
Serum from autistic individuals with GI disease (n = 31) was obtained from the Thoughtful House, Austin, Texas and chosen randomly. All of these children (median age 6 years; range 2-16; 8 male) had chronic digestive disease, most characterized with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach (identified by endoscopy).
Controls
Three control groups (n = 48) were studied, 19 autistic children without GI disease, and 29 non autistic controls (20 age matched non autistic children with no GI disease and 9 age matched non autistic children with GI disease). Serum and medical history of controls were obtained from the Autism Genetic Resource Exchange (AGRE * ).
The Autism Genetic Resource Exchange (AGRE) is the first collaborative gene bank for the study of autism spectrum disorders and one of the world's largest shared resources for the study of autism and related disorders, with a collection of over 900 well-characterized multiplex and simplex families made available to the greater scientific community. Founded by Cure Autism Now (CAN) in 1997, AGRE is currently funded by the National Institute of Mental Health (NIMH) and Autism Speaks (AS), which merged with CAN in 2006.
Serums
Experimental (Thoughtful House ** ) and control (AGRE) serums were all morning draws and then treated in an identical fashion—frozen at −70C immediately after collection and cell/serum separation, then stored at −70C until thawed for use in ELISAs.
The Thoughtful House is a comprehensive treatment and research center, specializing in the care of children with neurological disorders, including autism.
Statistics
Inferential statistics were derived from t-test and odds ratios with 95% confidence intervals. ANOVA analysis was used to do an analysis of variance and multiple comparisons.
Approval
This project has been approved by the Institutional Review Board of the Pfeiffer Treatment Center, Warrenville, Illinois.
Results
Serum from 50 autistic children; including 31 with chronic digestive disease (most with ileo-colonic lymphoid nodular hyperplasia and inflammation of the colorectum, small bowel and/or stomach) and 20 autistic children without GI disease, and 29 non autistic controls; including 20 age matched non autistic children with no GI disease and 9 age matched non autistic children with GI disease, was tested for Cu/Zn SOD using ELISAs designed to quantitate Cu/Zn SOD levels (described above). Each assay was repeated two or more times, with multiple wells for each serum in each assay. The results of a typical assay are represented on Figure 1. (Fig. 1: Controls).

The mean +/- SD Cu/Zn SOD concentration (ng/ml) of 50 autistic children (31 with chronic digestive disease (most with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach) and 19 autistic children without GI disease), and 29 non autistic controls (20 age matched non autistic children with no GI disease and 9 age matched non autistic children with GI disease).
Serum Cu/Zn SOD levels of autistic children were significantly lower than non autistic children (p < 0.0001) (Table 1), and serum Cu/Zn SOD levels in autistic children with GI disease were significantly lower than each of the other groups (autistic children with no GI disease (p < 0.0001), non autistic children without GI disease (<0.0001) and non autistic children with GI disease (p = 0.0003)) (Table 2). A one-way ANOVA analysis was also performed on the four groups (F = 24.83; p < 0.0001).
Significant difference between Cu/Zn SOD concentration (pg/ml) of 50 autistic children (with and without GI disease) and 29 age matched non autistic controls (with and without GI disease).
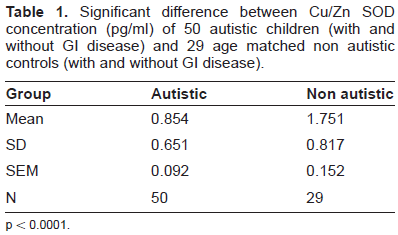
p < 0.0001.
Significant difference between Cu/Zn SOD concentration (ng/ml) of 31 autistic children with chronic digestive disease (most with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach) and 20 autistic children without GI disease, and 20 age matched non autistic children with no GI disease and 9 age matched non autistic children with GI disease.
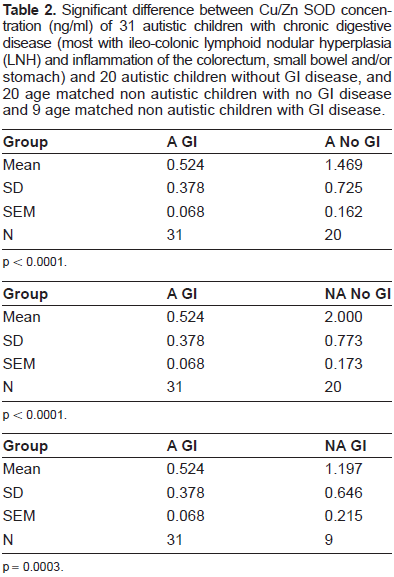
p < 0.0001.
p < 0.0001.
p = 0.0003.
Cu/Zn SOD concentration of autistic children with GI disease was compared to GI disease severity (including LNH and erythema). There was no significant association between Cu/Zn SOD levels and severity of the GI disease, including severity of LNH and erythema.
We previously reported that some of these same autistic children with GI disease had serum autoanti-bodies, measured by ELISA.57,58 We found borderline association between the presence of three autoantibodies (anti-PR3, anti-MPO and ASCA) and low Cu/Zn SOD (Table 3).
Serum Cu/Zn SOD associated with severity of GI disease and auto antibodies.

Discussion
Evidence suggests that increased oxidative stress is associated with autism, with likely contributions from environmental,46,47 genetic48–51 and immunological52–58 factors. This may be due to (a) increased production of endogenous pro-oxidants (such as NO, xanthine oxidase, homocysteine)59–64 or environmental pro-oxidants,65,66 or deficiencies of antioxidants (ceruloplasmin, transferrin, superoxide dismutase, glutathione peroxidase, catalase, reduced glutathione), or both.67–70 Reduced levels of serum ceruloplasmin (a copper-transport protein) and transferrin (an iron-transport protein) in autism suggest that metabolism of iron and copper (pro-oxidant components of oxidative stress) may be abnormal.
Increased oxidative stress, in turn, may lead to membrane lipid abnormalities,71,72 mitochondrial dysfunction,73–75 excitotoxicity,76,77 inflammation,78,79 and immunedys-regulation77,80–82 in autistic children, and might contribute to behavioral aberrations, sleep disorder, and gastrointestinal disturbances.83,84 Preliminary results of clinical trials have suggested improved behavior in individuals with autism who receive antioxidant therapy.85–87
A major cause of damage to cells results from reactive oxygen species (ROS)-induced alteration of proteins and DNA by reactive electrophilic oxidation products from polyunsaturated fatty acyls in membrane lipids. Oxidative stress and ROS have been implicated in disease states such as Alzheimer's disease, Parkinson's disease, cancer, atherosclerosis, age-related macular degeneration (AMD), and aging. Under normal conditions, ROS are cleared from the cell by the action of superoxide dismutase (SOD), 88 and abnormal concentrations may lead to an atypical brain phenotype in autistic children. 89
Our results show that a significant number of autistic children, particularly those with severe GI disease, have a lower concentration of serum Cu/Zn SOD when compared to controls.
Because low zinc levels have been associated with autism and related to lower Cu/Zn SOD levels, it may be associated with low Zn levels in autistic children. Also, low Cu/Zn SOD suggests a relationship between this anti-oxidant, thus oxidative stress, and autism-particularly in autistic children with GI disease.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author reports no conflicts of interest.