
Abstract
Studies linking vitamin D and long-term metabolic health have generated much debate. Recommendations for the intake of vitamin D by the general public and by the health care professionals have been complicated by a number of inconsistencies in the literature. These caveats relate to the methodological approaches, differences in the populations (and the species) of study, and the definitions used for thresholds of vitamin D status. This review addresses current evidence available for assessing the potential programming of long-term metabolic health of offspring by maternal vitamin D status in pregnancy. It summarizes knowledge on the early origins of metabolic health and analyzes evidence for an association between the vitamin D status in pregnancy and maternal and fetal health status. In addition, we analyze the link between the regulation of inflammation and the vitamin D status in the general population to inform on the general mechanisms through which early vitamin D might affect the programming of long-term health. The evidence suggests an association between the vitamin D status in early life and the programming of long-term health. However, to the best of our knowledge, the current finding is insufficient to draw a final conclusion for evidence-based preventive actions. The data warrant replication in prospective studies and additional research substantiating the causal factors and pathways.
Introduction
The biomedical community is debating the role of vitamin D in the etiology of metabolic and cardiovascular ill health. Of the 30 leading causes of death in the US, 19 have been linked to the vitamin D status in observational epidemiological studies, albeit sometimes inconsistently and without the identification of causal pathways. 1 In fact, besides an unequivocal role of vitamin D in the calcium metabolism, bone growth, and prevention of rickets and osteomalacia, much uncertainty remains. Lower vitamin D status, ideally defined by serum concentration of 25-hydroxyvitamin D [25(OH)D], has been reported to associate with impaired metabolic function in adults, including higher risk of obesity, diabetes mellitus (type 1 and type 2), and cardiovascular diseases.2–5 The present review summarizes the evidence addressing the role of vitamin D in the promotion of long-term metabolic health. It examines vitamin D in the context of the developmental origins of health and diseases paradigm and possible mechanisms through which vitamin D exposure may affect health programming. In particular, we review the current evidence for a role of maternal vitamin D in pregnancy in the programming of long-term metabolic health and review the knowledge on the association between the vitamin D status and the modulation of systemic inflammation aiming to provide insights on the general mechanisms through which vitamin D might provoke programming.
Developmental Origins of Cardiometabolic Health
Today, societies worldwide are undergoing important changes in the environments surrounding the developmental period. The global obesity and diabetes epidemics are accompanied by the variation of major metabolic risk factors arising in early life and increasing incidence of cases of gestational diabetes mellitus (GDM) and maternal obesity (representing 6%-15% of all pregnancies).6,7 These metabolic complications affect the health of mothers with an increasing risk of direct obstetric complications (ie, miscarriage, preterm delivery, and cesarean section) and also raise the risk of long-lasting metabolic diseases.8–11 The odds of developing obesity and/or type 2 diabetes following gestational obesity and diabetes are more than double in comparison to mothers remaining healthy in pregnancy.7,9 Moreover, offspring exposed to maternal obesity and/or GDM in prenatal life may be more susceptible to early onset cardiometabolic adversities. The increased risk observed in these offspring may be independent of confounding by genetic heritability and nongenetic shared maternal–offspring traits (ie, conferral of life style and behavioral factors between generations).
There is a compelling evidence on the role of the metabolic factors in early life in programming long-term risk of diseases. Epidemiological,12,13 genomical, 14 and experimental analyses15,16 are bringing supportive evidence for a causal role of early growth performance and the establishment of cardiometabolic homeostasis throughout life. The underlying mechanisms affecting programming of metabolic health in the growing fetus are yet to be fully understood, but the current research is focusing on deciphering both tissue-specific mechanisms as well as the potential time-dependency of exposures in determining programming. 17
Early Life Energetic, Epigenetic, and Trophic Remodeling
Alterations in dietary and life style factors are linked to dramatic changes in the profiles of metabolic traits. 15 This affects the metabolic factors in terms of both the amount and the type of metabolites that are available to the growing fetus as well as the cell signaling machinery and the pro- or anti-inflammatory pathways. 18 The developmental period starting from the periconceptual period and continuing far beyond the time of birth is considered as a plastic stage for the development of long-term metabolic functions. The energy and the macro- and micronutrients available to the growing organism act via trophic and epigenetic regulation to set some degree of metabolic function. 19 All components of metabolic homeostasis could be modifiable, and multiple examples have suggested that programming occurs in many key organs, ie, the liver, kidney, pancreas, adipose tissue(s), skeletal muscles, and hypothalamus.20,21 Metabolic stressors generated by various early life exposures such as maternal overfeeding, intrauterine growth restriction, and maternal insulin resistance are associated with the direct modifications of local and systemic inflammatory responses. 17 Both the programming of cellular gene expression (via epigenetic or other mechanisms) and organ size and function is thought to be a direct consequence of altered inflammatory balance.22,23
Importance of Critical Windows of Programming
Organogenesis and later fetal development is not a gradual, continuous process. There is an evidence for critical windows of programming affecting the risk of obesity, hypertension, and type 2 diabetes (see Symonds et al 19 for review). These windows have been observed in the analyses of data from historical birth cohorts24,25 and are consistent with an experimental evidence from animal models. 26 In humans, at least four prenatal windows with differential effects are proposed to exist, including (i) the periconceptual period with expected imprinting of the gametes; (ii) the embryonic period when major changes in the methylome occur; (iii) the second trimester of pregnancy when key remodeling appears in the hypothalamic and pancreatic regions; and (iv) the perinatal period when the fetus is experiencing exponential growth. In addition to these prenatal stages, observations from animal and human data suggest that critical moderating phases after birth could also be important programming periods. 12 As such, the first month of prenatal life, the peak of adiposity accrual, the rebound of adiposity, and perhaps also the entry into the pubertal period are representing some life course stages where exposures could have pronounced and irreversible effects on the long-term metabolic health. Each of these stages is essential in setting up neuroendocrine pathways and body composition throughout the adulthood. 16
Maternal Vitamin D Status and Metabolic Complications during Pregnancy
Exposure to maternal vitamin D status in pregnancy has been suggested to play a role in programming long-term health in offspring. 25(OH)D crosses the maternal–fetal placental barrier, 27 and at birth, cord blood 25(OH)D concentration is linearly associated with maternal 25(OH)D concentration.28,29
Preeclampsia
Preeclampsia characterized by maternal endothelial dysfunction, proteinuria, hypertension, and impaired placentation affects 2%-8% of the pregnant women and is responsible for 25% of maternal deaths worldwide.30,31 Although low vitamin D status is linked to the incidence of preeclampsia, the underlying mechanisms by which 25(OH)D influence it are unclear.30,31 Two systematic reviews and one nested case–control study have concluded that women with preeclampsia had lower 25(OH)D and calcitriol [1,25(OH)2D3] concentrations in the early pregnancy in comparison to normal pregnancy.32–34 Another nested case–control study by Achkar et al, based on 169 preeclampsia cases and 1,975 controls, reported a greater odds ratio for preeclampsia in women with lower vitamin D status (<30 nmol/L) after adjustment for life style and socioeconomic factors. 35 Four meta-analyses have also suggested that low maternal vitamin D status, with inconsistency on the definition, is associated with preeclampsia.36–39 A study based on isolated syncytiotrophoblasts from normal and preeclamptic women observed an inhibition of calcitriol production in preeclampsia patients, linked to a downregulation of 1α hydroxylase gene expression. 40 The reason for such low calcitriol concentrations in preeclampsia is unknown, as other related factors such as calcium, phosphate, and parathyroid hormone do not differ significantly between healthy pregnant and preeclamptic women.41–45 These observations suggest a causal link between vitamin D status and preeclampsia risk, which might in turn affect the fetal health.40,46 Furthermore, circulating insulin-like growth factor 1 (IGF-1) and maternal parathyroid hormone-related peptide concentrations are lower in preeclamptic women.47–51 IGF-1 placental mRNA expression and IGF-1 concentrations are found to be lower in preeclamptic women in comparison to healthy pregnant women.48,52,53 In addition to some observed associations of maternal 25(OH)D concentration with preeclampsia risk, it is frequently reported that preeclampsia can be characterized by an imbalance in the systemic circulation of inflammatory cytokines.54–56 In a study using flow cytometry to investigate cytokines in healthy and preeclamptic women, healthy pregnant women had a lower Th1:Th2 ratio and Th1 cell concentration in comparison to preeclamptic women. 57 This is consistent with another study where preeclamptic women were observed to have more a detrimental low-grade proinflammatory environment when compared to inflammatory profiles of healthy pregnant women. 58 Some studies have observed that cytokines, such as interleukin 6 (IL-6), tumor necrosis factor-α (TNF-α), IL-2/IL-10, IL-15, IL-16, IL-4, IL-18, TNF-α/IL-10, and C-reactive protein (CRP) are increased in preeclamptic women when compared to women with normal pregnancy. 41 Finally, two recent meta-analyses have reported that TNF-α, IL-6, and IL-10 concentrations are significantly higher in preeclamptic women.59,60 It must be noted that so far no study has measured the inflammation and the vitamin D status at the same time in preeclampsia women to infer a causal link. The evidence so far warrants additional research to analyze the moderation of the inflammatory status by the vitamin D status to support evidence-based preventive action.
Gestational diabetes mellitus
GDM affects 5%-16% of the pregnant women in populaces worldwide, depending on the diagnostic criteria used. 7 GDM is expected to expose the fetus to intrauterine hyperglycemia and increased insulin secretion in both the mother and offspring exposed to GDM and is found to be at higher risk of later development of early onset obesity and type 2 diabetes.61–63 A systematic review and meta-analysis of seven observational studies reported an inverse association between serum 25(OH)D and GDM [odds ratio 1.61 (95% CI: 1.19-2.17; P = 0.002)]. 64 The study included 2,146 pregnant women from various countries and ethnicities, which resulted in heterogeneity. 64 However, similar results were observed in other narrative and systematic reviews.37,38,65,66 A recent comprehensive systematic review and meta-analysis of observational studies including 22,000 pregnant women have reported insufficient serum 25(OH)D concentration linked to GDM and preeclampsia. 37 An observational study from Egypt on 160 pregnant women also reported an inverse association between glycated hemoglobin (HbA1c) and 25(OH)D concentrations. 67 The reasons for these associations between vitamin D deficiency and GDM have yet to be determined. A randomized controlled trial (RCT) involving 13 partners from 10 European countries Vitamin D and Lifestyle intervention for gestational diabetes mellitus prevention study (DALI study) to assess the potential effects of vitamin D supplementation in pregnancy on GDM risk has been completed in 2013, and the results are expected to give insight on future evidences for long-term metabolic health in mother and offspring. 68
Small for gestational age
Fetal growth and development might be affected by maternal vitamin D status.69,70 Several observational studies have observed the associations of higher maternal vitamin D status with lower risk of small for gestational age (SGA).69–72 In a population-based birth cohort comprising 2,274 pregnant women from the Netherlands, being in the lowest serum 25(OH)D quartile was associated with a higher risk of SGA. 72 A recent meta-analyses of 31 studies have reported that low maternal vitamin D status is associated with an increased risk of SGA [pooled odds ratio for <75 nmol/L: 1.85 (1.52-2.16)]. 37 Another meta-analysis using the literature from 24 studies reported a quite similar effect size [odds ratio (<50 nmol/L): 1.52 (1.08-2.15)]. 38 A recent birth cohort study from China examining the relationship between cord blood 25(OH)D, fetal growth, and SGA risk reported an inverted U-shaped association between 25(OH)D and fetal growth along with a moderate reduction of SGA risk with increased 25(OH)D. 73 The mechanism by which maternal serum 25(OH) D could affect the intrauterine growth or SGA remains elusive. A few well-designed epidemiological studies have provided human evidence to support the anti-inflammatory actions of the serum 25(OH)D status as frequently seen in experimental conditions in animal models74,75 and, more specifically, the potential for vitamin D receptor (VDR) to modulate the placental inflammation. 76 Studies using rodents as experimental models have also shown an association of maternal and placental inflammation with fetal growth restriction.75,77 An epidemiological study comparing cytokines in 19 women with normal pregnancy and 24 preeclamptic women showed that serum IL-8 and TNF-α concentrations were associated with fetal growth restriction in preeclamptic mothers. 78 More evidence is required to understand the exact mechanism by which serum 25(OH)D could be causally related to reduced risk of SGA in neonates. As described earlier, lower vitamin D status of women is linked to a number of adverse health traits in observational studies, but these associations may not represent causality and could reflect several other reasons such as lack of adjustment for residual confounding and/or reverse causality.
Vitamin D and its Role in Fetal Development
Experimental evidence suggests that vitamin D plays a profound role in fetal development through its action in human placental trophoblasts via the VDR and VDR signaling pathways. Placental trophoblasts also express cytochrome P450 enzymes encoded by 25-hydroxyvitamin D3 1-alpha hydroxylase (CYP27B1) and 1,25-dihydroxyvitamin D3 24-hydroxylase (CYP24A1) genes.79,80 1,25(OH)2D3 in the placenta is involved in the regulation of hormones involved in pregnancy,81,82 regulation of human chorionic gonadotropin expression, and secretion in synctiotrophoblast 83 and in the fetal glucose/insulin axis. 84 In addition, calcitriol plays an important role in the implantation by inducing decidualization and the modulation of the immune function during gestation.85–87 For example, primary cultures of human decidual cells and trophoblasts treated with 1,25(OH)2D3 (1-100 nM) showed an inhibition of granulocyte macrophage colony stimulating factor 2, TNF-α, and IL-6 and increases dose-dependent cathelicidin antimicrobial peptide (CAMP) production.88–90
Epidemiological Evidence for Associations between Maternal Vitamin D Status and Fetal Development
A recent study on serum 25(OH)D concentrations measured during pregnancy at three time points suggested that higher vitamin D status in the third trimester leads to 47% decrease in preterm births. 91 As discussed earlier, the review of the evidence is suggesting a role of vitamin D in the regulation of systemic inflammation during pregnancy, with potential downstream implications for offspring development and health. Observational evidence suggests that calcitriol could modulate immune function in the early life, modulate fetal and postnatal growth, and further supports speculations on the importance of vitamin D status in early life programming of long-term health.
The current knowledge on the association between maternal vitamin D deficiency and the programming of adiposity is shown in Table 1. The link between the maternal status in vitamin D and the risk for obesity (ie, proxied by BMI), hypertension (proxied by blood pressure), and type 2 diabetes (proxied by insulin resistance) has not been addressed in many studies, despite a potential protective role of vitamin D. A recent prospective birth cohort from a Spanish founder population (latitude 39°-43°N) has explored the link between maternal 25(OH)D at about 14 weeks of pregnancy in 2,489 mothers and growth and adiposity outcomes in offspring up to the age of four years. Offspring (irrespective of sex) born to mother with vitamin D deficiency (25(OH)D concentration < 50 nmol/L) were at a higher risk of being overweight at one year in comparison to offspring born to vitamin D-sufficient mothers (concentration > 75 nmol/L). The association in early life remains even after adjusting for maternal and fetal biological (body mass index [BMI], gestational weight gain, sex, and gestational age), social, and life style factors and could have been predicted from prenatal measures of fetal abdominal circumference. 92 Despite the lack of association observed at the age of four years, the study warrants follow-up and replication. In particular, BMI in toddler–preschool age is relatively heterogeneous and analyses focusing on more precise adiposity windows, such as the age of adiposity rebound, are critically needed.
A summary of the current surveys analyzing the impact of maternal vitamin D deficiency on offspring body composition showing large heterogeneity in the design, time of sampling during gestation, and the categorization of the vitamin D status.

Another longitudinal study of mothers and offspring from the Southampton Women's Survey (latitude 50°N) has reported a similar trend between vitamin D status measured at 34 weeks of gestation and child fat mass assayed by Dualenergy x-ray absorptiometry scanning at birth, four years, and six years of age. 93 The authors reported that lower serum 25(OH)D concentration was associated with greater fat mass at the age of six years, but the association was attenuated at the age of four years after adjustment for potential confounders. The study also reported on the positive association between maternal 25(OH)D and fat mass at birth. 93 The association at the age of six years remained significant despite correcting for multiple cofactors, including breast feeding duration and vitamin D supplementation during childhood. Interestingly, the vitamin status at 34 weeks was robustly predicted by the season of blood sampling (Fig. 1), which raises important question on the best way to define maternal vitamin D status in pregnancy. 93 Results from the Amsterdam born children and their development (ABCD) study (Amsterdam, latitude 52°N) on a multiethnic population defined a linear inverse correlation between maternal deficiency (vitamin D < 30 nmol/L) at 13 weeks of gestational age and the risk of being small for gestational age. Further aside, the observation of the current study has shown a higher postnatal growth velocity in the child born to deficient mother, suggestive of postnatal catch-up growth. 94 Another study from a German (Berlin, latitude 52°N) population of 547 singleton-bearing mothers further supports a link between maternal vitamin D status and offspring birth weight. 95 This study examined birth traits of offspring born to mothers with severe vitamin D deficiency at birth [25(OH)D < 1 nmol/L] in comparison to those born to vitamin D-sufficient mothers (controls). In this specific case, the 37 offspring had a poorer Agpar defining newborn general health status (ie, appearance, pulse, grimace, activity, and respiration) scores and were in average 14% smaller in weight than the control infants (n = 510) and were born 10 days earlier. 95 Such an example of severe vitamin D deficiency in the mother has yet to be replicated in additional studies to delineate the underlying mechanisms and the additional confounders. However, the study was substantiated by a translational experiment in mice suggesting an independent risk of postnatal growth retardation, premature death, and impaired glucose tolerance. 95 The recent China-Anhui Birth Cohort Study (latitude 30°N) on 3,658 pregnant women has reported that maternal vitamin D deficiency levels (concentration < 50 nmol/L) have a relative risk (RR) of SGA [RR: 6.47 (4.30-9.75)] and low birth weight infants [RR: 12.31 (4.47-33.89)] when compared to sufficient vitamin D levels (concentration ≥ 75 nmol/L) even after adjustment for confounders. 73 Another follow-up study of Indian children (n = 568, latitude 12°N) at the age of 5 and 9.5 years with maternal 25(OH)D measured at the time of delivery has shown that boys born to vitamin D deficient mothers (<50 nmol/L) had a higher body fat percentage and lower fat-free mass when compared to girls at the age of 5 years but not at 9.5 years. 96 The study has also observed that the lower maternal 25(OH)D status is associated with higher insulin resistance at the age of 9.5 years even after adjustment of all maternal covariates. 96 This direct link between severe vitamin D deficiency and fetal outcomes has been supported by additional experiment in rodents, including effects on reduced placental weight, increased maternal corticosterone concentrations and impairment in placental vascular development, 97 maternal hypertension and dysregulated placental development, 98 persistent inflammation, and insulin resistance in the offspring. 99 Finally, a recent systematic review and meta-analysis study on the effect of vitamin D supplementation during pregnancy have revealed that the vitamin D supplementation was associated with increased 25(OH)D concentration with positive outcomes on birth weight and birth length. 100
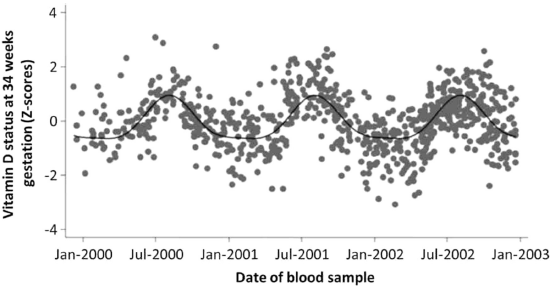
Fourier analysis of maternal vitamin D status (serum 25(OH)D concentration) at 34 weeks of gestation according to the date of blood sample collection (from Crozier et al 93 ).
VDR and the Immune System
The identification of the VDR in the membranes of peripheral blood mononuclear cells ignited early research on vitamin D as a potential immune regulator.101,102 Calcitriol exerts its genomic actions via the VDR, which is present in many tissues of the body, including trophoblasts and adipocytes.80,103,104 VDR is also expressed in monocytes, macrophages, dendritic cells, and activated T-cells, suggesting that vitamin D can affect inflammation. 102 There are more than 36 cell types that are acted upon by 1,25(OH)2D3 via the VDR. 105 Calcitriol, the active form of vitamin D, is involved in the up- and downregulation of a wide variety of genes.106,107 The studies of transcriptomics using microarray approaches focused on the protein-coding mRNAs that were regulated by the VDR, usually following the treatment with ligand. These studies quickly established the approximate size and surprising diversity of the VDR transcriptome, revealing it to be highly heterogeneous by cell type and also time dependent.89,108
Calcitriol plays an important role in modulating the immune system and the active functioning of the innate, and adaptive immune system is affected by vitamin D status. 109 Liu et al established that the paracrine synthesis of 1,25(OH)2D3 by monocytes plays an important role in the innate immune response against the infectious pathogen Mycobacterium tuberculosis. 110 The study also suggested that with the activation of the toll-like receptor (TLR), VDR, and vitamin D, 1-α-hydroxylase gene expression is upregulated in human macrophages. They further synthesize CAMP/LL37 and result in the killing of M. tuberculosis in an intracrine fashion. The serum isolated from African-American individuals in the study whose 25(OH)D concentrations were less than 30 nmol/L was more susceptible to tuberculosis due to nonsufficient cathelicidin messenger RNA induction. This suggests that low vitamin D status is associated with the increased vulnerability to attack by pathogens, suggesting the prominent role of vitamin D in immune signaling. 110 This is further supported by an experiment on isolated macrophages where vitamin D dosing was found to upregulate I-kappa levels and a subsequent decrease of nuclear NF-kappa beta (NF-κβ) activity. NF-κβ is an important transcription factor for inflammatory mediators, and the results of the study suggest that 1,25(OH)2D3 has an anti-inflammatory action in macrophages.107,111 In monocytes and macrophages, intracrine synthesis of 1,25(OH)2D3 stimulates bactericidal activity, whereas in dendritic cells, its function and maturation are suppressed.89,112,113 Calcitriol further enhances dendritic cells and stimulates the production and function of T-regulatory cells, which are important mediators of immune tolerance. 114
The innate immune system that activates the adaptive immune system is primarily made up of T- and B-lymphocytes. 115 In adaptive immune system, calcitriol inhibits the proliferation of T-lymphocyte and the differentiation and proliferation of B-lymphocytes and inhibits immunoglobulin production.116–119 The differentiation of T-cells is affected by calcitriol in vitro, which inhibits Th1 response and stimulates the Th2 response. 120 To date, in CD4+ T-cells, 102 genes targeted by 1,25(OH)2D3 have been recognized, 121 and it is considered that the immunomodulatory effects of vitamin D on the Th1/Th2 response occur by decreasing the production of interferon-γ (IFN-γ) and IL-2 and increasing the production of IL-4, IL-5, and IL-10 and shift toward Th2 response.122,123 The effects of 1,25(OH)2D3 on B-cells are noticeable in patients with systemic lupus erythematous. 116 The neutrophils that are also a part of the innate immune system express abundant VDR. They also act in a similar way to monocytes in the induction of LL37 and bactericidal activity in response to 1,25(OH)2D3.124,125
Adipose Tissue and Inflammation
The obesity pandemic is increasing worldwide at a staggering rate, and the epidemic parallels the rise in the incidence of vitamin D insufficiency.18,126,127 A meta-analysis reported a significant inverse but minute correlation between higher BMI and serum 25(OH)D. 128 Another recent (2015) systematic review and meta-analysis study examining 23 relevant articles from PubMed/Medline, Web of Science, and Scopus databases reported a prevalence of vitamin D deficiency of 35% and 24%, respectively, in obese and overweight individuals irrespective of age. 129 There are various plausible hypotheses pertaining the link between a reduced vitamin D concentration in obese and overweight individuals that include limited dietary intake, reduced sun exposure due to limited outdoor physical activity, reduced intestinal absorption, and the sequestration of vitamin D in adipose tissue.128,131,132 The association between the BMI and the vitamin D status is further supported from a bidirectional instrumental variable approach (Mendelian randomization) and meta-analysis of 21 population cohorts that included up to 42,024 participants with 12 BMI-related single nucleotide polymorphisms (SNPs). The study concluded that for every 1 kg/m2 increase in BMI, serum 25(OH)D was decreased by 1.2%, and for every 10% increase in instrumental BMI variable, the serum 25(OH)D decreased by 4.2% (IV estimate 95% CI: -7.1, -1.3, P = 0.005). 3 This supports a causal link between obesity and lower vitamin D status, and not the reverse. 3 As to whether the impaired vitamin D status associated with obesity can alter metabolic health via proinflammatory pathways remains to be fully discerned. 18 Adipose tissue is now recognized as an important mediator of impaired metabolic health in relation to obesity, most of which can be explained by the release of proinflammatory mediators.132–134
For instance, the hypertrophy of the adipose organ leads to a reduced secretion of adiponectin and increased secretion of proinflammatory mediators, namely, IL-6, TNF-α, IL-8, monocyte chemoattractant protein-1, and resistin.135–137 Adipose tissue is a major determinant of IL-6 concentration that increases with obesity and leads to lipolysis and fatty acid oxidation.138,139 Interestingly, experimental studies on mouse 3T3-L1 cell line and isolated human adipocytes have shown that 1,25(OH)2D3 modulates chronic inflammation in adipose tissue. 18 For example, research on mature adipocytes from our own group illustrated that 1,25(OH)2D3 could suppress Lipopolysaccharide-stimulated IL-6 secretion by NF-κβ inflammatory pathway in a dose-dependent manner. 107 The results were later confirmed in other experimental models using both mouse and human adipocytes.140–142
Epidemiological Evidence on Associations between Vitamin D and Inflammation in Nonpregnant Adults
While experimental models clearly suggest direct effects of vitamin D on inflammatory pathways, epidemiological evidence from human samples of both metabolically healthy and unhealthy individuals is equivocal at present. 107 Some, but not all, epidemiological reports have found associations between proinflammatory factors and lower vitamin D status (see Table 2). In an observational study on 69 healthy women aged 25-82 years exploring the association of inflammatory biomarkers with vitamin D status, TNF-α showed a linear inverse relationship with serum 25(OH)D concentration. 143 Similar results were observed in another study on 19 healthy runners with TNF-α concentration (R 2 = 56.5, P < 0.001). 144 Another study on 957 older adults from Northern Ireland aged >60 years has demonstrated significant negative correlation with IL-6, CRP, IL-6/IL-10, CRP/IL-10, and TNF-α/IL-10 ratio with serum 25(OH)D concentration. 145 A similar inverse relationship was found between IL-6, soluble IL-6 receptors, and serum 25(OH)D concentration in InCHIANTI study on 867 older adults aged >65 years. 146 Another cross-sectional study on 95 healthy adults from Japan, aged 21-69 years, has showed a positive association between IL-17 and serum 25(OH)D concentrations. 147 The major limitations of these studies are its cross-sectional design, low sample size, and inclusion of individuals from wide age groups. In addition, the evidence from available RCTs fails to establish an effect of vitamin D supplementation of the modulation of inflammation in obese and healthy individuals. Subsequently, many analytical and methodological shortcomings have yet to be considered to understand in detail the physiological role of vitamin D in the modulation of the inflammatory stress in vivo. The analysis should be better corrected for a number of cofactors, allowing us a better capture of the life style and behavioral confounding. Stratified or personalized analyses taking into account the gender, the age, the ethnicity, and the adiposity should also be considered. Finally, only a limited number of inflammatory makers have been considered that limits the possibility to underpin the relevant metabolic pathways. Observations in epidemiology and animal models are suggestive of a protection of cardiometabolic status by serum 25(OH)D. It must be acknowledged that the relation between vitamin D and metabolic health raises a large debate whether the vitamin D status might be simply a mere reflection of individual's own health. For instance, two large-scale Mendelian randomization studies do not support a causal link between low vitamin D and the onset of obesity 3 and incident type 2 diabetes. 148 A number of residual confounding might explain some associations and warrant further well-designed research. In particular, it might be essential to account for factors of physical fitness and well-defined measures of insulin sensitivity to correct the effects.
A summary of recent epidemiological evidence for an association between serum 25(OH)D and the inflammatory component.

Conclusion
The immune system interface between the mother and her fetus is essential for maintaining a healthy pregnancy, sustaining maternal immunocompetence, and supporting the development of the offspring immune system. 149 One association study using data on 153 pregnant Indian women observed that altered maternal 25(OH)D could have a wide range of effects on regulatory T-and B-cells with IgE receptors. 150 In fact, the placental vitamin D-deficient women was characterized by a downregulation of the regulatory T-cell transcription factor FOX3, VDR, retinoic acid receptor in comparison to control placenta. In contrast, CD23, CD21, and vitamin D-binding protein expression was upregulated by vitamin D. 150 An RCT following 225 infants examining the association of 25(OH)D in cord blood in relation to innate immune response has observed that increasing maternal vitamin D during pregnancy and early life will lessen the risk of allergy induced by cytokines. 151 An observational study from Germany evaluating the association of season at birth, cord blood 25(OH)D, and the markers of allergy (IL-10 and IgE) reported that serum 25(OH)D was correlated with IL-10 levels. 152
The current knowledge on maternal vitamin D status in pregnancy and its association with metabolic and neonatal outcomes cannot be easily translated into guidelines for clinical practice due to many inconsistencies in findings and heterogeneity of evidence sources. The Lancet's Nutrition Interventions Review Group and Maternal and Child Nutrition Group, which made a comprehensive literature-based analysis, have identified that vitamin D status has an essential role in child nutrition and termed it as emerging intervention. The study calls for additional good-quality RCTs to support the findings. 153 Our present review reports a lack of robust evidence to support systematic vitamin D supplementation in pregnancy in the general population with a purpose to moderate metabolic ill health. The review of the current biochemical evidence suggests that an empirical function for vitamin D has a potent modeling factor of the metabolic functions in human fetus. An adequate vitamin D status might act through various epigenetic and trophic factors to program the activity and the responsiveness of the metabolic organs. The current knowledge supports that vitamin D would act through the modulation of placental function and the regulation of systemic inflammation. However, there remain some important shortcomings and methodological pitfalls to be ascertained. Future studies shall carefully consider the research design, the implementation stage, and the dose of supplementation. 154 The challenge ahead must also help to identify an international definition of the vitamin D status that might be personalized according to the ethnic group, the stage of pregnancy, and the season. This later appears particularly challenging to test as both the programming of metabolic health and the vitamin D status are linked to specific windows with potential differential effect. The Finnish Vitamin D Trial (results expected 2020), Vitamin D and Omega-3 Trial study (results expected 2017), CAPS study (results expected 2015), Do-health (results expected 2017), and D-tect study will provide the future evidence on a long-term association between the vitamin D status in the early stage of the life course and long-term metabolic outcomes.155,156
Author Contributions
Designed and written the review and its illustration: SP under the supervision of SS. Contributed intellectually to the drafting of the manuscript: SP, DW, M-RJ, and SS. All authors reviewed and approved the final manuscript.