
Abstract
We aimed to evaluate the association between serum vitamin D status and elastic properties of aorta in patients with diabetes mellitus (DM). We studied 136 patients with newly diagnosed DM (mean age: 62.9 ± 10.6 years). Serum 25-hydroxyvitamin D was measured using a direct competitive chemiluminescent immunoassay. Aortic distensibility was calculated from the echocardiographically derived ascending aorta diameters and haemodynamic pressure measurements. Left ventricle mass index (LVMI) was determined according to the Devereux formula. Multiple linear regression analysis showed that vitamin D level is independently associated with LVMI (β = −0.259, p = 0.001), aortic distensibility (β = 0.369, p < 0.001), high-sensitive C-reactive protein (hs-CRP) (β = −0.220, p = 0.002) and body mass index (β = −0.167, p = 0.015) in patients with DM. In diabetic patients, serum 25-hydroxyvitamin D level is independently associated with aortic distensibility. Vitamin D may play a role on pathogenesis of impaired elastic properties of aorta in type 2 DM.
Introduction
Type 2 diabetes mellitus (DM) is an established major independent risk factor for cardiovascular disease. Serum 25-hydroxyvitamin D (vitamin D), the major circulating form of vitamin D deficiency, is a substantially prevalent condition in patients with type 2 DM. 1 Low serum levels of 25-hydroxyvitamin D have been associated with all-cause mortality. 2
Aortic distensibility (AD) is a measurement of vascular elasticity and impaired AD reflects increased aortic stiffness. Arterial stiffness is an early marker of systemic atherosclerosis. 3 Moreover, increased arterial stiffness has been shown to be an independent risk factor for both cardiovascular disease and overall mortality. 4
Macrovascular complications of DM are associated with stiffening of the aorta, which is a major contributing factor to the target organ damage. 5 However, the potential role of vitamin D in diabetic macrovascular complications remains unclear. In this study, we aimed to evaluate the association between serum vitamin D status and AD in patients with DM.
Methods
Study population
Between June 2012 and February 2013, 136 (male/female = 60/76, mean age: 62.9 ± 10.6 years) patients with newly diagnosed type 2 DM were enrolled to this cross-sectional study. The patients were divided into two groups according to serum vitamin D level: vitamin Ddeficiency group (<20 ng/mL, n = 80) and vitamin Dsufficient group (≥20 ng/mL, n = 56). 5 Type 2 DM was defined according to the Standards of Medical Care in Diabetes of the American Diabetes Association. According to the criteria of the World Health Organization, 6 newly diagnosed diabetes was defined as having two or more elevated blood glucose levels (fasting plasma glucose of ≥126 mg/dL or 2-h postprandial plasma glucose of ≥140 mg/dL) in two occasions at least 1 week apart in subjects without a history of diabetes. To exclude the potential pharmacological effects, previous diabetic patients were not included in the study. None of the patients were taking calcium or vitamin D supplements. Institutional ethics committee approved the study, and written informed consent for participation in the study was obtained from all individuals.
Serum 25-hydroxyvitamin D was measured using a direct competitive chemiluminescent immunoassay (Elecsys; Roche Diagnostics, Mannheim, Germany).
Echocardiography and AD
Left ventricular mass (LVM) was calculated using the Devereux formula; left ventricular mass index (LVMI) was obtained by the following formula: LVM/body surface area. The AD was calculated: AD = 2× (ascending aorta systolic diameter − ascending aorta diastolic diameter)/(ascending aorta diastolic diameter × pulse pressure) (cm2 dyn−1 × 10−6). 7
Statistical analysis
Comparison of categorical variables between the groups was performed using the χ2 test. Independent samples t test was used in the analysis of continuous variables. The correlations between vitamin D and laboratory haemodynamic and echocardiographic parameters were assessed by the Pearson correlation test. Multiple linear regression analysis was performed to identify the independent associations of vitamin D. A value of p < 0.05 was considered statistically significant.
Results
Deficient vitamin D levels were observed at 58.8% of patients with DM (80 patients). Comparisons of baseline, laboratory and echocardiographic characteristics between the groups were summarised in Table 1. LVMI values of vitamin Ddeficiency group were higher than vitamin Dsufficient group (p < 0.001). The lowest AD values were observed in vitamin Ddeficiency group compared with vitamin Dsufficient group (p < 0.001).
Comparison of baseline, laboratory and echocardiographic findings between the groups.
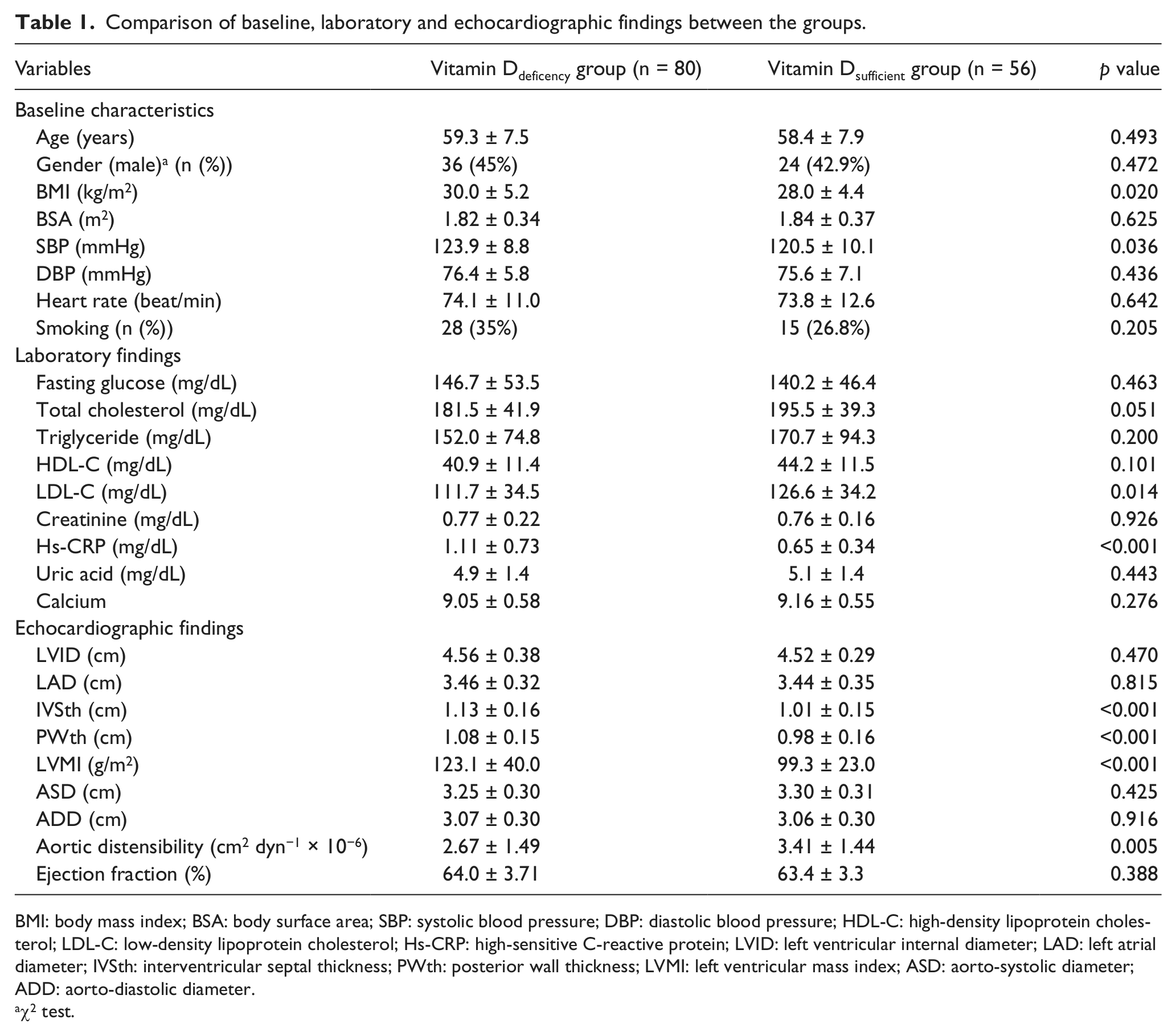
BMI: body mass index; BSA: body surface area; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; Hs-CRP: high-sensitive C-reactive protein; LVID: left ventricular internal diameter; LAD: left atrial diameter; IVSth: interventricular septal thickness; PWth: posterior wall thickness; LVMI: left ventricular mass index; ASD: aorto-systolic diameter; ADD: aorto-diastolic diameter.
χ2 test.
Bivariate and multivariate relationships of vitamin D
In patient group, vitamin D was associated with haemoglobin A1C (HbA1C) (r = −0.201, p = 0.019), hs-CRP (−0.448, p < 0.001), LVMI (r = −0.451, p < 0.001), systolic blood pressure (r = −0.225, p = 0.008), AD (r = 0.573, p < 0.001), low-density lipoprotein (LDL) cholesterol (r = 0.333, p < 0.001) and body mass index (BMI) (r = −0.184, p = 0.032) in bivariate analysis. Relationship between vitamin D and AD is shown in Figure 1. Multiple linear regression analysis showed that vitamin D level was independently associated with LVMI (β = −0.259, p = 0.001), AD (β = 0.369, p < 0.001), BMI (β = −0.167, p = 0.015) and hs-CRP (β = −0.220, p = 0.002).
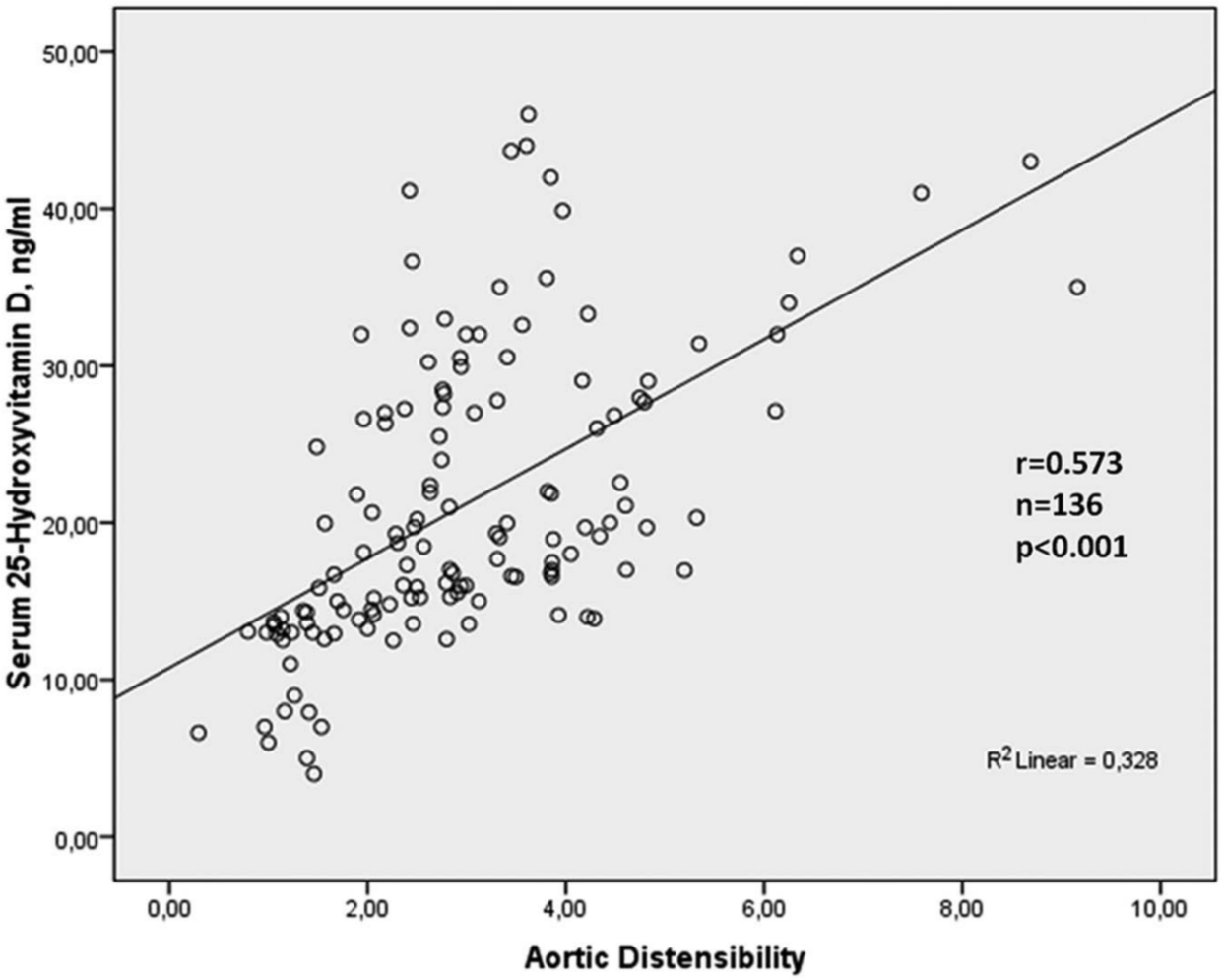
Relationship between serum 25-hydroxyvitamin D level and aortic distensibility.
Discussion
The main findings of the present study are that (1) patients with vitamin Ddeficiency group have higher LVMI and lower AD values compared with patients with vitamin Dsufficient group and (2) vitamin D level is independently associated with AD, LVMI, hs-CRP and BMI on multiple linear regression analysis.
Association between hypovitaminosis D and DM is well known. Such relationship between vitamin D and DM is not surprising given that vitamin D deficiency has been associated with insulin resistance and impaired β-cell function. 8 Recently, Lee et al. 9 reported that low 25-dihydroxy vitamin D level is significantly associated with increased arterial stiffness in patients with DM. Moreover, relationship between endothelial dysfunction and low vitamin D level was reported in patients with DM. 10
Previous studies were reported that lower vitamin D is associated with increased arterial stiffness. 9 In diabetic patients, relationship between arterial stiffness and vitamin D level was reported in only one study. 9 However, in previous studies, AD was not investigated according to vitamin D levels. In our study, we showed that lower vitamin D level is independently associated with impaired AD. The precise pathophysiological mechanisms between lower vitamin D level and impaired AD are still unknown. Impaired AD may reflect an underlying high inflammatory state, 10 increased vascular calcification, impaired endothelial function, 11 activated renin–angiotensin system 12 and atherosclerosis10–12 that are associated with low vitamin D levels. Vitamin D regulates the renin–angiotensin system, suppresses proliferation of vascular smooth muscle, modulates vascular inflammation and improves insulin resistance and endothelial cell-dependent vasodilatation.10,12 Lower serum vitamin D level may promote proliferation of vascular smooth muscle, inhibit endothelial cell-dependent vasodilatation and increase vascular calcification. There is evidence that vascular calcification might contribute to the increase in arterial stiffness. 13 Lower vitamin D levels may be effective on impaired aortic distensibility by increasing arterial calcification. Another possible mechanism for link between AD and low vitamin D may be via endothelial dysfunction. 11 It is well known that there is an association between endothelial dysfunction and increased arterial stiffness. In the present study, hs-CRP values were higher in patients with vitamin Ddeficiency group compared with vitamin Dsufficient group, and vitamin D was independently associated with hs-CRP. Finally, Salum et al. 5 showed that vitamin D supplementation prevented the fragmentation of elastic fibres in the aortic media in animal model. This finding shows that vitamin D has effects on the fragmentation of elastic fibres of aorta, which may be compatible with our findings revealing the lowest AD values to be observed in vitamin deficiency group.
In addition to impaired AD, our results showed that low vitamin D level is also an independent predictor of increased LVMI in diabetic patients. Prior studies showed a relationship between vitamin D deficiency and left ventricular hypertrophy in patients with chronic kidney disease. 14 Actual mechanisms underlying vitamin D deficiency–mediated aortic stiffness still remain unclear. However, several plausible mechanisms can explain how vitamin D may influence arterial stiffness and left ventricular hypertrophy. Molecular and cell biology research has shown vitamin D receptors to be present on vascular smooth muscle, endothelium and cardiomyocytes. 15 Vitamin D influences cardiac and vascular functions by exerting antiproliferative effects on vascular smooth muscle 16 and mediates vascular inflammation by regulating lymphocyte and monocytes/macrophage differentiation and release of inflammatory cytokines. 15
In the present study, lower vitamin D level is independently associated with BMI as well as AD and LVMI. Patients with 25(OH)D deficiency has significantly higher BMIs compared to those with sufficient levels of 25(OH)D. 17 This result supports research that suggests sequestering of 25(OH)D in adipose tissue and decreasing the amount of circulating 25(OH)D. 17
Conclusion
Our study showed that low vitamin D level is independently associated with AD as well as left ventricle hypertrophy and inflammation in newly diagnosed diabetic patients. Low vitamin D level may play a role in pathogenesis of impaired elastic properties of aorta and left ventricle hypertrophy in diabetic patients.
Footnotes
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.