
Abstract
Single port transumbilical laparoscopic surgery (LESS, SILS, ENOTES) is a technique which has recently emerged with a view to improving the cosmesis following minimal access surgery, aiming to achieve ‘scarless’ surgery. This rapidly progressing technique is facilitated by developments in port and instrument technology, allowing surgeons to perform a wider range of surgical procedures with increasing ease. This paper aims to summarise the equipment available at present for single port surgery.
Ports
There are four multi-lumen single port trocar options available for transumbilical laparoscopy currently available. These are the Tri- and Quad-ports (Advanced Surgical Concepts, Wicklow, Ireland distributed by Olympus), the Uni-X port (Pnavel Systems, Morganville, NJ, USA), and the SILS port (Covidien, Mansfield, MA, USA). Through a single intraumbilical incision, multilumen access can also be achieved by using standard laparoscopic trocars through adjacent fascial incisions.
Triport, quadport
The ASC ports (also known as the R-port) use a fascial retractor system with an internal distal ring advanced into the abdomen with a blunt introducer and an external proximal ring, joined by a plastic sleeve which is retractable with a removal ring. This allows the distal ring to be pulled flush to the abdominal wall creating a gas-tight seal. Externally there are three or four instrument lumens and an insufflation line. Each channel is covered with a thermoplastic elastomeric gel valve which forms a tight seal to maintain pneumoperitoneum whilst allowing smooth instrument introduction. The Triport has three channels, allowing up to one 12 mm and two 5 mm instruments, whilst the Quadport has four lumens, permitting up to one 15 mm, two 10 mm and one 5 mm instruments.

This system allows a range of incision sizes depending on required instrumentation and the blunt introducer minimises risk of visceral trauma. An effective seal is maintained by the retracting sleeve pulling the internal ring tight to the abdominal wall. Whilst traditional laparoscopic trocars protrude into the operative space, the internal ring lying flush to the abdominal wall allows wider, less cluttered visual field and also improved instrument mobility. The low-profile design also allows the use of bent instruments, previously not possible with the restriction of traditional straight trocars.
SILS port
The SILS Port is inserted via Hassan technique. It is flexible port that sits snugly in the fascia maintaining a seal and contains three lumens. Three short removable ports may be inserted through the lumens allowing an interchangeable combination of up to three 5 mm ports or two 5 mm ports and one 12 mm port. A separate insufflation line controlled by two-way valve.

Uni-X
The Uni-X system consists of a conical plastic outer unit converging on three 5-mm lumens. This is inserted using a Hassan technique. Four fascial sutures affixed to the device effectively create a tight seal for pneumoperitoneum. This port is no longer available commercially.

Multiple standard trocars
Two or three standard 5 mm laparoscopic trocars may be inserted via adjacent fascial incisions through a single umbilical skin incision, providing an alternative means of single port surgery. This has a cost advantage over the multilumen ports available, but due to the bulk of the trocars mobility can be limited by clashing ports. There are also then multiple fascial incisions to close at completion of surgery potentially causing increased risk of port-site hernia.
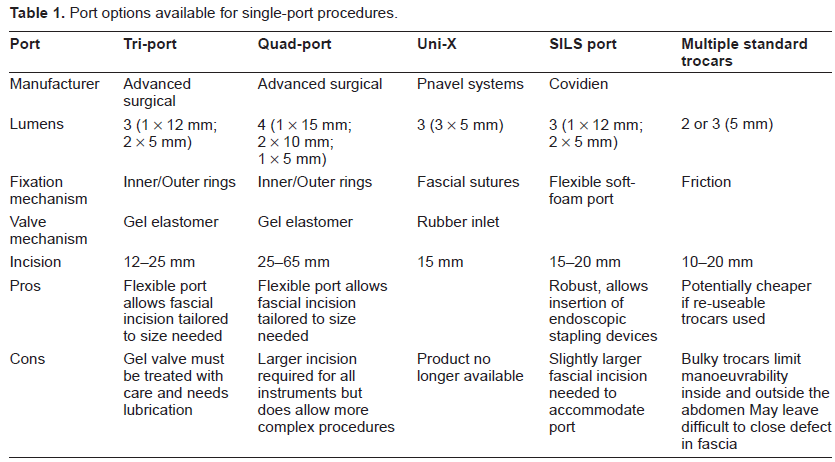
A comparison of the various options for single port laparoscopic surgery can be found in Table 1.
Port options available for single-port procedures.
Instrumentation and Endoscopy Systems
The cornerstones of conventional laparoscopic surgery are triangulation and retraction, which are achieved by ports placed far apart. Single port surgery does not have this option and therefore utilises two different techniques to succeed. The first uses standard straight instruments crossing at the point of entry, resulting in the right hand working the left instrument. The second involves the use of flexible, roticulating or curved instruments.
Optimal instrument position allows proper tissue retraction, essential to effective dissection in anatomical tissue planes. Placing several parallel instruments, as required in single port surgery, makes this considerably more difficult. The use of at least one flexible or curved instrument can adjust the angle enough to allow improved triangulation; however this usually requires the surgeon's instruments to cross, necessitating counterintuitive external movements. This can result in a degree of external crowding of instruments, and clashing of instruments should be expected and allowed for, especially during the training in these procedures.
External crowding can be problematic when the surgeon's and assistant's hands are occupying the same space. This is inevitable when using standard straight instruments with bulky handles and a straight laparoscope with a light lead at 90 degrees to the scope and bulky camera head. The following list of camera systems and instruments can be used with a combination of standard re-useable equipment to minimize expenditure.

Cameras and endoscopes
When deciding upon a camera system for single port surgery the following attributes are advantageous. Firstly a 5 mm diameter scope takes up less space in the port requiring a smaller fascial incision and leaves a 10–12 mm port free for larger instruments e.g. reticulating endoscopic stapling devices. Avoidance of a separate external light lead gives more space to work externally and avoids the camera being knocked by the surgeon when working the instruments. A scope with a field of view of 30 degrees to the axis gives more space internally and externally but a flexible tipped scope allowing a variable angle of view is ideal. If an internally flexible scope is not available then an externally flexible scope will at least remove the assistant's hands from the surgeon's field. Integrated digital cameras also minimize external bulk and give more space. Completely flexible endoscopes are not autoclaveable and therefore can't be used in the UK. They also may not maintain position as desired or give as optimal optical view.
Future possibilities include the use of NOTES (Natural Orifice Transluminal Endoscopic Surgery) equipment such as flexible endoscopes with working channels or integrated diathermy and retraction or wireless camera systems similar to capsule endoscopy inserted internally and mobilized with use of an external magnet.
The following is a list of camera systems that differ from standard rigid conventional laparoscopes offering some advantages for single port surgery.
Endoeye
The EndoEye camera system has a distally mounted camera chip with a streamlined light cable as opposed to the standard laparoscopic light cable which enters the lens at 90°.

This limits camera bulkiness and thus minimises extracorporeal clashing. These instruments are available in 5 mm and 10 mm versions with 0°, 30° or 45° directional views and in two different lengths to accommodate larger patients.
They are also available with a deflectable tip allowing the target site to be viewed from many angles. A 10 mm flexible tip scope is already available in the UK and a 5 mm flexible tipped scope is awaited but may not be suitable for autoclaving.

An externally flexible 10 mm laparoscope has also been used which at least places the assistant's hands out of the way.

The chief advantage of a digital system is that the camera chip is close to the surgical field therefore a longer flexible scope does not degrade picture quality.
Storz
Storz supply a long 5 mm laparoscope which takes an HD camera head, but still has the light lead at 90° making it more bulky and increased length of optics in front of the camera may degrade the image slightly.
Stryker
A long 5 mm bariatric scope is available compatible with HD systems but also risks picture degradation over the length of the scope.

Instruments
Covidien
These reticulating laparoscopic instruments use technology allowing the tips to be angled relative to the shafts and providing the means for articulation of instruments passed through a single port site. Available are the Endo Dissect with unipolar diathermy and standard jaws; Endo Mini-Shears with unipolar diathermy; and Endo Grasp with spin lock; all of which are 31 cm long 5 mm instruments.

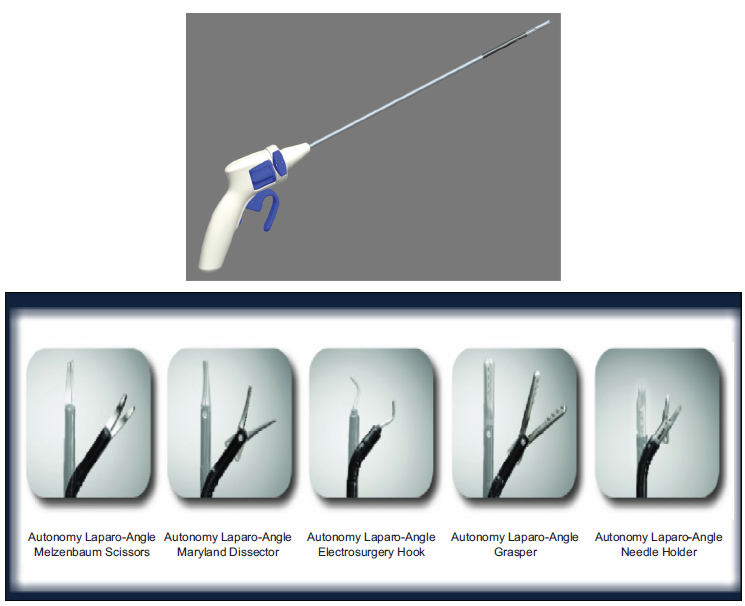
Autonomy Laparo-Angle, Cambridge Endo (Elemental Healthcare UK)
Angle locking mechanism with axial rotation.
Tip can rotate 360° around its axis giving 7 degrees of freedom.
All instruments available in standard (33–34 cm) and long (44–45 cm) shaft lengths.
Instruments include: scissors, dissector, diathermy hook, grasper and needle holder.
Specialised scopes and cameras for single port surgery.

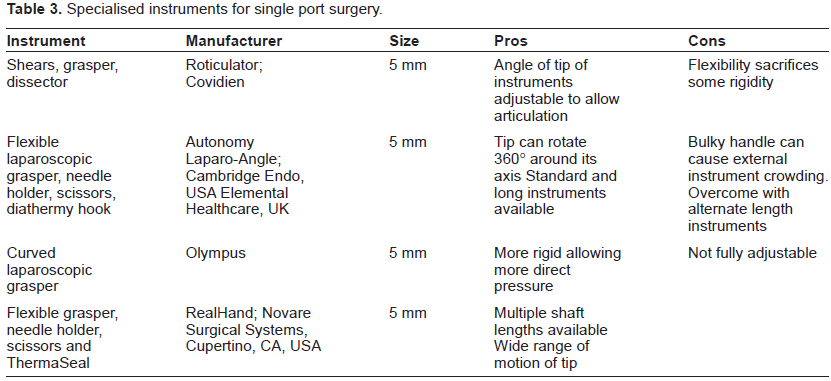
Specialised instruments for single port surgery.
Olympus
Curved instruments are available which rotate but do not reticulate. Thus the angle of curvature is fixed which may be useful when additional stiffness is needed.
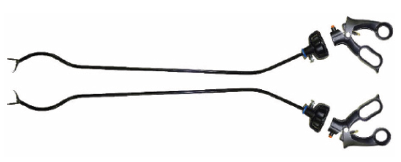
RealHand
7 degrees of freedom with mirrored hand movements.
Ergonomic handle.
Standard (34 cm), long (45 cm) and extra-long (75 cm) shaft lengths.

Summary
Standard laparoscopic instruments can of course still be used for single port surgery and can often be optimal in combination with specialist single port instruments. Fixed straight instruments do offer the advantage of complete rigidity and therefore transmit applied force and retraction consistently. For many simple procedures such as appendicectomy straight instruments are often all that is required.
Future instrumentation
Whilst there have been several developments in laparoscopic instruments to enhance single port surgery, there is still potential for further improvements. Despite these recently introduced bent and flexible instruments, clashing is still a major issue. It may be that motorised instruments would be a solution to this problem. Certainly, instrumentation with streamlined, low-profile handles would lessen extracorporeal crowding.
Disclosures
The authors report no conflicts of interest.