
Abstract
Objective
To estimate the safety and feasibility of laparoendoscopic single-site surgery (LESS) in pregnant patients with acute abdomen.
Methods
Baseline characteristics, surgical results, and obstetric and neonatal outcomes were retrospectively compared between single and multiport procedures in patients who underwent laparoscopic surgery during pregnancy between 2017 and 2021.
Results
Fifty-four pregnant patients were included: 26 who underwent LESS (salpingectomy, 11 cases/cystectomy, 15 cases) and 28 who underwent conventional laparoscopic surgeries (salpingectomy, 12 cases/cystectomy, 16 cases) during pregnancy. One patient in the single-port group required additional ports. No patients converted to laparotomy. In patients undergoing salpingectomy, the single-port group showed lower 8- and 24-h postoperative pain scores, shorter hospital stays, and lower Self-rating Anxiety Scale scores prior to discharge versus conventional laparoscopy. One patient experienced postoperative vaginal bleeding and a missed abortion during follow-up. In patients receiving cystectomy, 8- and 24-h pain scores, postoperative hospital stay, and anxiety scores were lower in the single-port versus multiport group. Other outcomes were comparable between the groups.
Conclusion
The feasibility and efficacy of laparoscopic surgery during pregnancy is similar between single- or multiport routes, however, the single-port route may be associated with less postoperative pain, shorter hospital stay, and lower anxiety.
Keywords
Introduction
At present, 0.2–2.2% of gravid women require surgical interventions for a variety of non-obstetric problems, such as acute abdomen, a large benign mass, or potentially malignant tumours.1–3 Though there are risks of pregnancy-related complications perioperatively, some procedures, such as cystectomy, salpingectomy and salpingo-oophorectomy, are often performed, particularly in patients with acute abdomen.1,4,5 During pregnancy, such procedures are usually performed via a conventional laparotomy approach, however, with rapid advances in the development of microinvasive technologies, laparoscopic surgery is considered a suitable alternative, due to the advantage of reduced physiological response to manipulation versus that produced by laparotomy. 6 In this respect, laparoscopy is associated with improved maternal outcomes through reduced postoperative pain, use of analgesics, and length of overall hospital stay. Moreover, laparoscopy may confer several advantages to fetal outcomes, such as reduced potential for fetal respiratory depression due to lower postoperative exposure to narcotics, and a reduced possibility of spontaneous abortion or preterm labour as a result of decreased uterine irritability due to minimized manipulation.6–9
Laparoendoscopic single-site surgery (LESS) has emerged in response to the increased requirements for more minimally invasive surgery, and has been widely used for various gynaecological conditions, including occasional use in obstetrics.10,11 The LESS procedure, performed via a single umbilical incision, may minimize incision pain, particularly in gravid patients, since a progressively enlarging uterus leads to increasing distension of the abdominal wall postoperatively, and thus, LESS may promote the continued optimization of pregnancy outcomes.12–16 Another possible advantage of LESS is umbilical entrance to the abdominal cavity, which may help to reduce the potential for injury to the enlarged uterus and displaced viscera during pregnancy, caused by insertion of the Veress needle. 13 Moreover, specimens may be easily extracted through the large umbilical incision without the need for extending the incision.
Though widely considered safe and feasible for gynaecologic disease, many clinicians have been hesitant to perform LESS in pregnant women, due to the scarcity of relevant literature and relatively high-quality evidence. Few multicentre studies involving patients undergoing LESS during pregnancy have been reported to date,10,17 and the role of LESS in surgical intervention during pregnancy remains unclear. Thus, the aim of the present study was to investigate the role of LESS during pregnancy, by retrospectively comparing LESS with conventional laparoscopic surgery.
Patients and methods
Study population
This retrospective study comprised patients who underwent laparoscopic surgery for acute abdomen during pregnancy at Shenyang Women’s and Children’s Hospital, between 2017 and 2021. Pregnant patients who underwent laparoscopic single cystectomy or salpingectomy were included, and those who underwent additional procedures during the operation were excluded. Patients’ electronic records were searched for baseline characteristics, age, body mass index (BMI), parity, estimated gestational age (EGA), history of previous abdominal surgery, cyst size and comorbid medical disease. Data relating to surgical outcomes, operating time, estimated blood loss, transfusion, open or multi-port surgery conversion, duration of hospital stay, postoperative pain score, and perioperative complications were extracted and analysed. Obstetric and neonatal outcomes were recorded, including Self-rating Anxiety Scale (SAS) score, 18 missed abortion (fetal death at <20 weeks), preterm labour (<37 weeks), postpartum haemorrhage, postpartum infection, term labour, normal or caesarean delivery, Apgar scores at 1 and 5 min, neonatal intensive care hospitalization and neonatal mortality or morbidity. Perioperative complication was defined as any complication that occurred during the operation and within 30 days following surgery.
This study was approved by the ethics committee of Shenyang Women’s and Children’s Hospital. All details relating to treatment methods were shared and discussed with patients, and all patients provided verbal informed consent for their treatment and for the study. The reporting of this study conforms to STROBE guidelines. 19
Surgical procedure
All procedures were performed by experienced surgeons (XN, JN) using a Stryker endoscopy system (Stryker, Kalamazoo, MI, USA) and disposable trocar (Kang Ji, Hang Zhou, China). General anaesthesia was induced and maintained using standard procedures, and patients were positioned in the supine position. After creating a 2.0- to 2.5-cm umbilical incision, the inner ring of the wound retractor was inserted to stretch the fascial incision, and the outer ring of the wound retractor was rolled for connecting the sealing member. Except for the number of ports, identical surgical procedures were followed for LESS and for the conventional route. The abdominal wall was closed using a layer-by-layer method, and the umbilical contours were restored with a subcutaneous running closure using a 3-0 absorbable suture (Covidien, St. Louis, MO, USA).20,21 The fetal heart rate (FHR) was detected immediately after surgery to confirm the viability of the fetus, and abdominal Doppler ultrasound was performed before surgery, and at 3 days after surgery, to confirm the presence of a live fetus inside the patient’s uterus.
Statistical analyses
Categorical variables are presented as numbers and percentages and continuous variables are presented as median (quartile 1 [Q1] and quartile 3 [Q3]). Data were statistically analysed using SPSS software, version 25.0 (IBM, Armonk, NY, USA) on an intention-to-treat basis. Thus, patients who converted to open surgery, or who required additional ports, remained in their primary group for analysis. Between-group differences in baseline characteristics, surgical results and obstetric and neonatal outcomes were analysed using Mann–Whitney U-test or Fisher’s exact test. A P-value <0.05 was considered statistically significant.
Results
A total of 54 eligible cases were included in this study (summarised in Table 1), comprising 26 patients who underwent LESS and 28 who underwent conventional laparoscopic surgery for acute abdomen during pregnancy: 49 in the first trimester (7–13+5 EGA), and five in the second trimester (14+2–17+1 EGA). In the LESS and conventional groups, respectively, median age was 33 (30.5, 35.0) years and 31.5 (29.0, 35.3) years for patients undergoing single salpingectomy (P = 0.642); and 32 (29.5, 35.0) years and 33 (29.8, 35.3) years for patients undergoing single cystectomy (P = 0.795). There were no statistically significant between-group differences in BMI, parity, history of previous abdominal surgery, comorbid disease, and gestational age at surgery (Table 1), regardless of whether salpingectomy or cystectomy was performed. In patients who underwent cystectomy, ovarian cyst size was not statistically different between the LESS and conventional multiport groups (P = 0.921).
Baseline demographic and clinical characteristics of pregnant patients who underwent LESS or conventional laparoscopic surgery for acute abdomen.
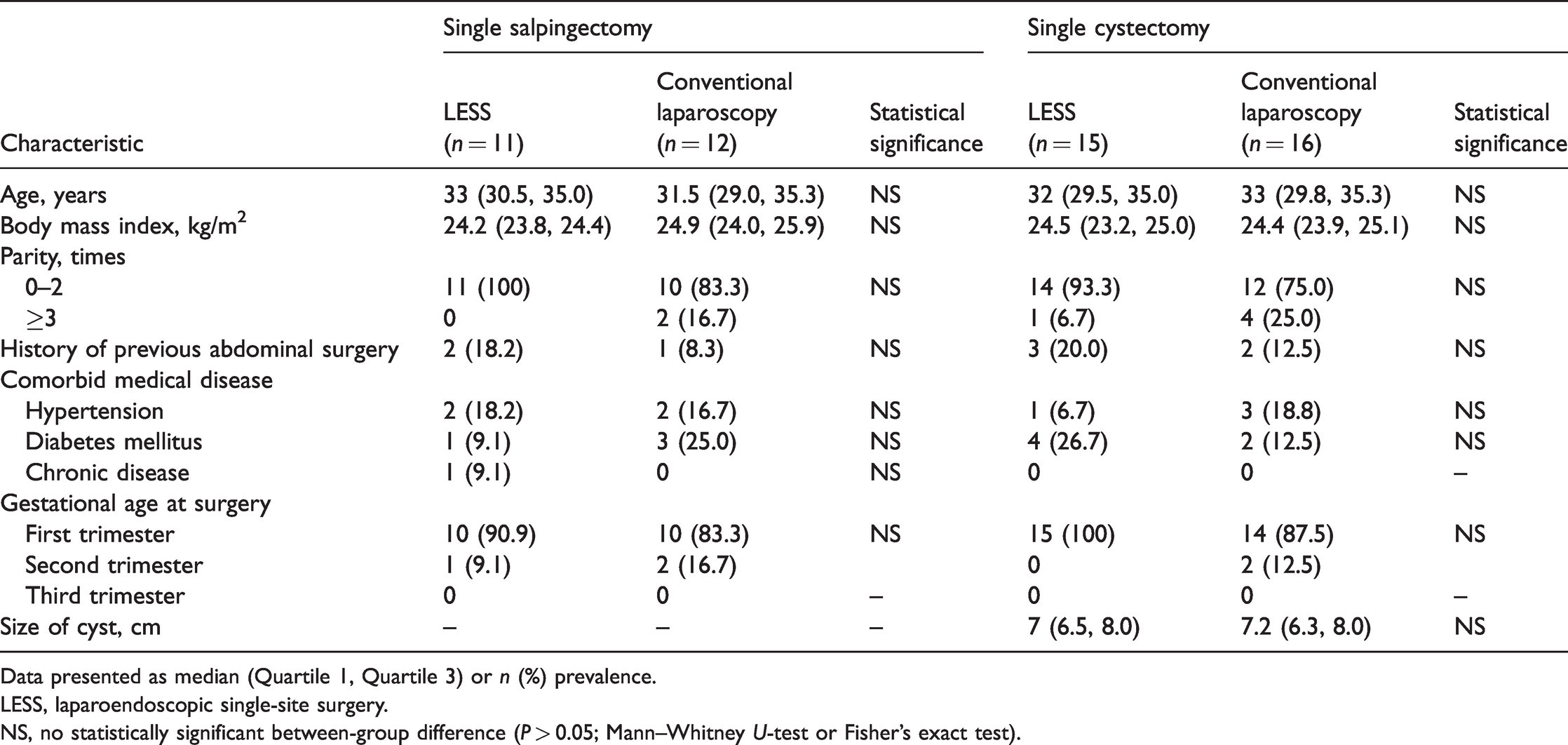
Data presented as median (Quartile 1, Quartile 3) or n (%) prevalence.
LESS, laparoendoscopic single-site surgery.
NS, no statistically significant between-group difference (P > 0.05; Mann–Whitney U-test or Fisher’s exact test).
Among patients undergoing cystectomy, no patients in the conventional laparoscopy group, but one in the LESS group, required additional ports (P = 0.484). The patient in the LESS group who required additional ports presented with pelvic adhesion and limited view, so the additional port was used to ensure the safety of both mother and fetus. No patients who underwent salpingectomy required additional ports or converted to laparotomy, and no patients in the study required a blood transfusion. Doppler ultrasound revealed a live fetus inside the uterus in all cases.
Laparoscopic single salpingectomy was performed in 23 patients with acute abdomen: 11 who underwent LESS and 12 who underwent conventional laparoscopy. All patients presented with vaginal bleeding, and this was combined with acute abdominal pain in 12 patients, one of whom reported experiencing syncope. Operating time ranged between 35 and 59 min in the LESS group and between 32 and 55 min in the conventional group, with estimated blood losses of 50–450 ml and 90–600 ml, respectively. Cases of heterotopic pregnancy (intrauterine coexisting with extrauterine pregnancy) were confirmed postoperatively by pathology results. Operating time, estimated blood loss, and postoperative pain scores at 48 and 72 h were not significantly different between the groups (Table 2). The LESS group showed lower 8- and 24-h postoperative pain scores and shorter duration of hospital stay (P = 0.016; P < 0.001; and P < 0.001, respectively) versus the conventional group. Also, patients in the LESS group presented with lower SAS scores 3 days after surgery (P = 0.042; Table 2). One patient in the LESS group experienced vaginal bleeding following surgery, which was managed conservatively. No patients in the conventional group experienced perioperative complications. There were no statistically significant between-group differences in maternal and neonatal outcomes, including postpartum haemorrhage, preterm labour, caesarean section, neonatal Apgar scores, and neonatal intensive care hospitalization (Table 2). Of note, one patient in the LESS group experienced a missed abortion during postoperative follow-up (at 11 weeks’ EGA).
Comparison of surgical and pregnancy outcomes between LESS and conventional laparoscopic surgery.

Data presented as median (Quartile 1, Quartile 3) or n (%) incidence.
LESS, laparoendoscopic single-site surgery; SAS, Self-rating Anxiety Scale; NICU, neonatal intensive care unit.
NS, no statistically significant between-group difference (P >0.05; Mann–Whitney U-test or Fisher’s exact test).
Single cystectomy for acute abdomen was performed in 15 patients in the LESS group and 16 patients in the conventional group. All patients reported different degrees of abdominal pain, with six patients reporting pain accompanied by nausea and vomiting. Cyst torsion or rupture (29 versus two cases) were diagnosed intraoperatively during the subsequent single or multiport surgeries. Operating times ranged between 45 and 75 min, and between 42 and 70 min, for the LESS and multiport surgeries respectively, with estimated blood losses of 30–75 and 25–80 ml, respectively. Of patients who received single cystectomy, five were diagnosed with simple cyst, five with corpus luteum cyst, eight with serous cystadenoma, 11 with mature cystic teratoma and two were diagnosed with mucinous cystadenoma. In patients with corpus luteum cyst, progesterone supplementation via vaginal suppositories were administrated preventively. There were no statistically significant between-group differences in operating time, estimated blood loss, or postoperative pain score at 48 and 72 h (Table 2), however, 8- and 24-h postoperative pain scores were lower in the LESS group (P = 0.001 and P = 0.007, respectively). In addition, patients in the LESS group had shorter lengths of postoperative hospital stay (P = 0.001) and significantly lower SAS scores at 3 days after surgery (P = 0.021; Table 2). No perioperative complications occurred in patients who underwent cystectomy. There were no differences in maternal and neonatal outcomes, such as postpartum haemorrhage, preterm labour, caesarean section, neonatal Apgar scores, and neonatal intensive care hospitalization (Table 2), and no missed abortion occurred in this group.
Discussion
The results of the present study indicate that LESS may be a feasible procedure in pregnant patients with acute abdomen, as only one patient (3.8%) required additional ports and no case converted to an open operation to complete the surgery. In pregnant patients, LESS has several advantages compared with conventional laparoscopy routes. First, one umbilical incision only is associated with decreased postoperative pain and discomfort caused by a large gravid uterus and scar expansion, which greatly reduces patients' anxiety and fear, and may improve the health of both mother and fetus. In addition, the umbilical port is a safe approach to enter and work in the abdominal cavity, as it may help to avoid the potential injury risk of an enlarged uterus and displaced viscera. Moreover, the umbilical incision in LESS offers an efficient outlet for safely extracting large specimens without the need to extend the port incision to accommodate the mass, and the in-bag procedure reduces the risk of spillage of the mass contents in cases where a potential malignancy is suspected. 22 The operation may then be performed externally, and the use of pneumoperitoneum may be stopped at this point, thereby reducing the duration of CO2 insufflation, with lower adverse effects on the fetus. 23
Although LESS is technically safe and feasible in pregnancy, the LESS procedure remains associated with several concerns. First, it may be difficult to manoeuvre instruments due to obstruction of view, proximity of the working instruments, loss of triangulation, and limited range of motion in one port. 24 In addition, the LESS procedure may be less useful in gravid patients with endometrioma or other conditions that are prone to pelvic sidewall scarring, which may require substantial manipulations to remove safely. In the present study, one patient in the LESS group presented with pelvic adhesion and limited view, so the additional port was used to ensure the safety of the mother and fetus. Other concerns associated with LESS surgery performed during pregnancy include perioperative maternal and neonatal outcomes. The present results indicate that LESS may significantly decrease postoperative pain, as well as reduce hospital stays for pregnant women. Patients' mental health condition was also evaluated in the present study using the SAS, and patients who underwent surgery via LESS were revealed to have lower SAS scores at 3 days after surgery compared with those who received multiport surgery. These results may indicate a potential advantage of LESS over conventional laparoscopic surgery in decreasing the risk of depression during pregnancy, and even postpartum depression. Doppler ultrasound, performed before and 3 days after surgery, revealed a live fetus inside the uterus in all cases. All cases in the present study had an uncomplicated pregnancy perioperatively, however, one patient who underwent LESS salpingectomy reported vaginal bleeding at 1 week following surgery, and then experienced a spontaneous abortion at 11 weeks’ EGA. Subsequent review of this patient’s medical history suggested that the patient had experienced two previous unexplained abortions, which may suggest confounding factors when considering the cause of this miscarriage. Moreover, the possibility that certain unknown factors (e.g., different maternal care, and psychological or social causes) may have accounted for the finding, could not be ruled out.
The LESS procedure may be associated with several technical issues. The first concern is a higher risk of umbilical hernia formation due to an increase in the incision size, however, the overall risk of umbilical hernia formation in LESS is currently considered low. 25 In the present 26 patients, the fascial defects were repaired using a layer-by-layer method to minimize the potential for umbilical hernias, 21 and no hernias were detected during the postoperative follow-up. Concerns related to pneumoperitoneum during pregnancy include possible damage to the uteroplacental perfusion due to compromised venous return to the mother's heart and fetal acidosis caused by absorption of carbon dioxide gas. 26 Insufflation with 10–15 mmHg of carbon dioxide is basically safe and recommended for gravid women. 8 For all surgeries at Shenyang Women’s and Children’s Hospital, insufflation at 9–12 mmHg is used, which is lower than the suggested insufflation levels. No difficulties were reported during the operations in the present study, and we believe that insufflation levels at 9–12 mmHg are feasible for performing surgeries successfully, and further reduce risk to the fetus. Additionally, in our opinion, uterine manipulation should be avoided, to optimize infant prognosis as well as to reduce the potential of adverse pregnancy outcomes. Regarding surgical timing, the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) 2017 guidelines state that laparoscopic procedures may be safely performed in pregnant patients during any trimester. 8 In the present study, 49 patients were in the first trimester and five were in the second trimester during surgery, and all surgeries were conducted for relieving acute symptoms, demonstrating that the LESS procedure may be safely performed in the early stage of pregnancy. Furthermore, progesterone supplementation via vaginal suppositories was administrated preventively in five patients who underwent corpus luteum cyst excision for torsion, as the ovary actively secretes progesterone to maintain the pregnancy in the first seven weeks of gestation. 27
In conclusion, LESS surgery appeared to be a safe and feasible alternative to conventional laparoscopic surgery for the management of gynaecological acute abdomen during pregnancy, with comparable perioperative surgical and pregnancy outcomes. In addition, LESS was associated with decreased postoperative pain, earlier discharge and lower SAS scores compared with conventional laparoscopy, and is associated with better cosmetic results (due to a single umbilical port versus multiple abdominal port incisions). With rapid development of laparoscopic technology, LESS promises to provide continued optimization of the prognosis of both mother and fetus in patients requiring surgical intervention during pregnancy.