
Abstract
Objective
Scar-related cosmetic outcomes were compared prospectively between conventional three-port and single-port access laparoscopic adnexal gynaecological surgery.
Methods
Enrolled patients were randomly assigned to a single- or three-port surgery group. Scar-related outcomes were evaluated at 1 month, 6 months and 1 year. Scars were assessed by an independent observer using the modified Vancouver Scar Scale (mVSS). All patients were asked about pain related to the scar and scar satisfaction; results were recorded using a numerical rating scale.
Results
Seventy-three patients were enrolled between June 2010 and June 2011. Demographic and surgical outcomes did not differ between the groups. mVSS results were similar in the two groups at each follow-up point. The scar satisfaction profile measured at 1 month showed no significant difference between the groups, but the single-port access group had better results than the conventional group at all other follow-up timepoints.
Conclusion
Cosmetic outcome was better for single-port than for three-port adnexal gynaecological surgery at 6-month and 1-year follow-up.
Introduction
Innovations in minimally invasive surgery in the past decade have led to the advent of single-port laparoscopic surgery becoming state-of-the art technology. Single-port access (SPA) gynaecological surgery offers the patient the option of having only one incision through the umbilical region. However, the concept of a single-incision operation is not new. Laparoscopic tubal sterilization through a single umbilical incision was performed in the late 1960s and early 1970s.1,2 Recent advances in instrumentation, access ports and lighting have allowed the laparoscopic surgeon to perform more complex surgery through a single port, however. Reduction in the number of ports offers the possibilities of reducing postoperative pain, improving cosmetic results, decreasing hospital stay and shortening the time needed for recovery.3–8 However, it is not clear whether SPA surgery results in better clinical outcomes, compared with conventional laparoscopic techniques.
In the present study, cosmetic outcomes and scar-related satisfaction were compared prospectively and randomly between patients undergoing SPA or conventional laparoscopic adnexal surgery.
Patients and methods
This study was approved by the Institutional Review Board of Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea. All patients included in the study provided written informed consent to participate.
Patients
Female patients with an adnexal mass, for whom laparoscopic surgery was planned, were enrolled in the study between June 2010 and June 2011. Patients whose adnexal mass raised suspicion of malignancy or who were unsuitable for general anaesthesia were excluded from the study. All participants provided written informed consent and underwent a standardized preoperative evaluation. Patients were randomly assigned to either SPA or conventional laparoscopic surgery by a computer-generated randomization schedule, operated by the surgeon. All patients were enrolled by the primary surgeon (E. H. Y.), who had ample experience of conventional laparoscopic surgery and had performed ≥ 10 SPA laparoscopic operations before enrolment of patients into the present study began. Before surgery, all patients received single-dose antibiotic prophylaxis (1 g cefotiam, administered intravenously). All participants underwent standard operative care under general anaesthesia.
Surgery
Each conventional laparoscopic operation was performed using a three-port method with one 12-mm and two 5-mm ports. An 0° 10-mm telescope was used. The first transverse infraumbilical 12-mm reusable port was placed, using a closed technique, after insufflating the peritoneal cavity with carbon dioxide through a Verres needle. Additionally, two 5-mm disposable ports were placed in the left and right lower quadrants, respectively. Specimens were extracted with a retrieval bag, through a transumbilical 12-mm port, under the guidance of a 30° 5-mm telescope, through the 5-mm port.
Each SPA laparoscopic operation was performed using a surgical technique similar to that used for conventional laparoscopic surgery. A multiport trocar (SILS®, Coviden, Manchester, MA, USA) was placed after making a 2.0-cm curvilinear transumbilical incision, using an open approach. A 30° 5-mm telescope and rigid conventional 5-mm laparoscopic instruments were used. Specimens were extracted with a retrieval bag through the 12-mm SILS® port. The peritoneum and fascia were approximated and closed layer by layer with 2-0 polyglactin 910 suture. The skin was closed with a continuous subcuticular suture. Operative parameters and postoperative complications were recorded prospectively.
Postoperative observations
Participants received the same postoperative analgesia prescription, based on propacetamol (1 g, administered intravenously, twice daily) with tramadol (ampoules of 50 mg, administered via intramuscular injection) on demand, for additional pain control. Patients were asked to rate their pain using a visual analogue scale (VAS, range 0–10, where 10 represented the worst possible pain) at 6, 12, 24 and 48 h after surgery. Amounts of nonsteroidal anti-inflammatory drugs used during hospitalization were recorded daily. All patients received the same regimen of oral analgesia – 600 mg of dexibuprofen, daily – for the first 5 days following surgery, and returned to the outpatient clinic of the Department of Obstetrics and Gynaecology for suture removal, 7 days postoperatively.
Scars were evaluated by an investigator using the modified Vancouver Scar Scale (mVSS), 9 6 months after surgery. The mVSS provides a numerical assessment of four scar characteristics: vascularity (range 0–3), pigmentation (range 0–3), pliability (range 0–4) and height (range 0–4), with a total score ranging between 0 and 14; a score of 0 indicates normal skin. 9 The investigator scored each scar site based on comparison with the patient’s normal skin, and divided the total score by 3 for patients undergoing conventional laparoscopic surgery, to obtain an average (mean) score.
One month, 6 months and 1 year after surgery, participants underwent physical examination by an investigator and were asked about pain related to the scar and scar satisfaction, using a numerical rating scale (NRS, range 0–10, with a score of 10 representing supreme satisfaction) by a nurse who was blinded to the treatment assignment.
Statistical analyses
The mVSS scores, scar-related satisfaction (NRS), postoperative pain (VAS), analgesia requirements, morbidity, duration of operation, length of hospital stay and change in haemoglobin concentration between 1 day before and 1 day after the operation were compared between the groups, using the two-sided Pearson F2 test or Fisher’s exact test for dichotomous variables and the Mann–Whitney U-test for parametric continuous variables. A two-tailed P-value of <0.05 was considered statistically significant. Statistical analyses were performed with SPSS® Software, version 12.0 (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of patients undergoing single-port access (SPA) or conventional laparoscopic adnexal (gynaecological) surgery.

There were no significant differences between the two groups.
Haemorrhagic corpus luteum cyst, paratubal cyst, fibrothecoma, simple cyst.
Operative results of patients undergoing single-port access (SPA) or conventional laparoscopic adnexal (gynaecological) surgery.
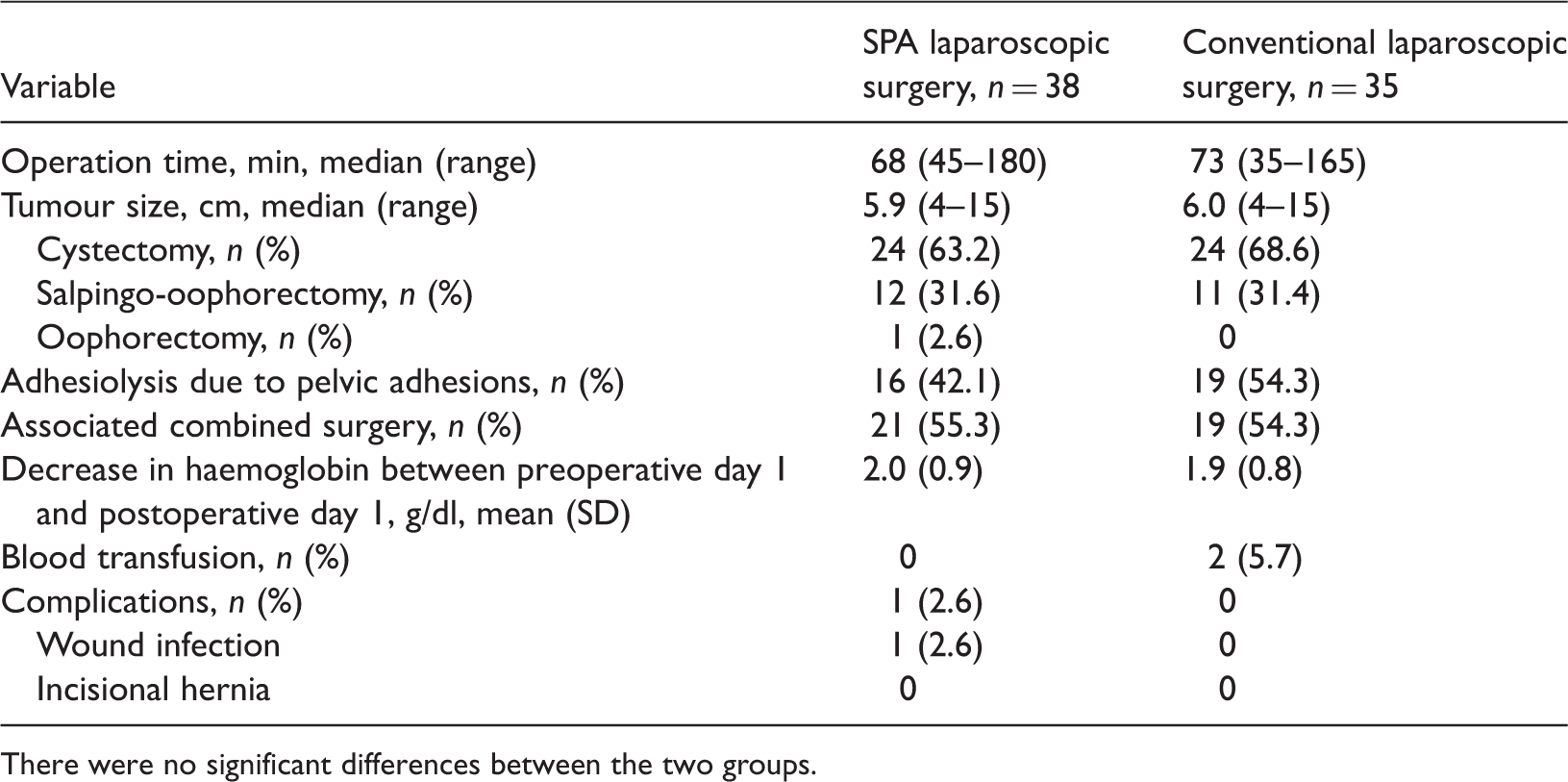
There were no significant differences between the two groups.
Postoperative results of patients undergoing single-port access (SPA) or conventional laparoscopic adnexal surgery.
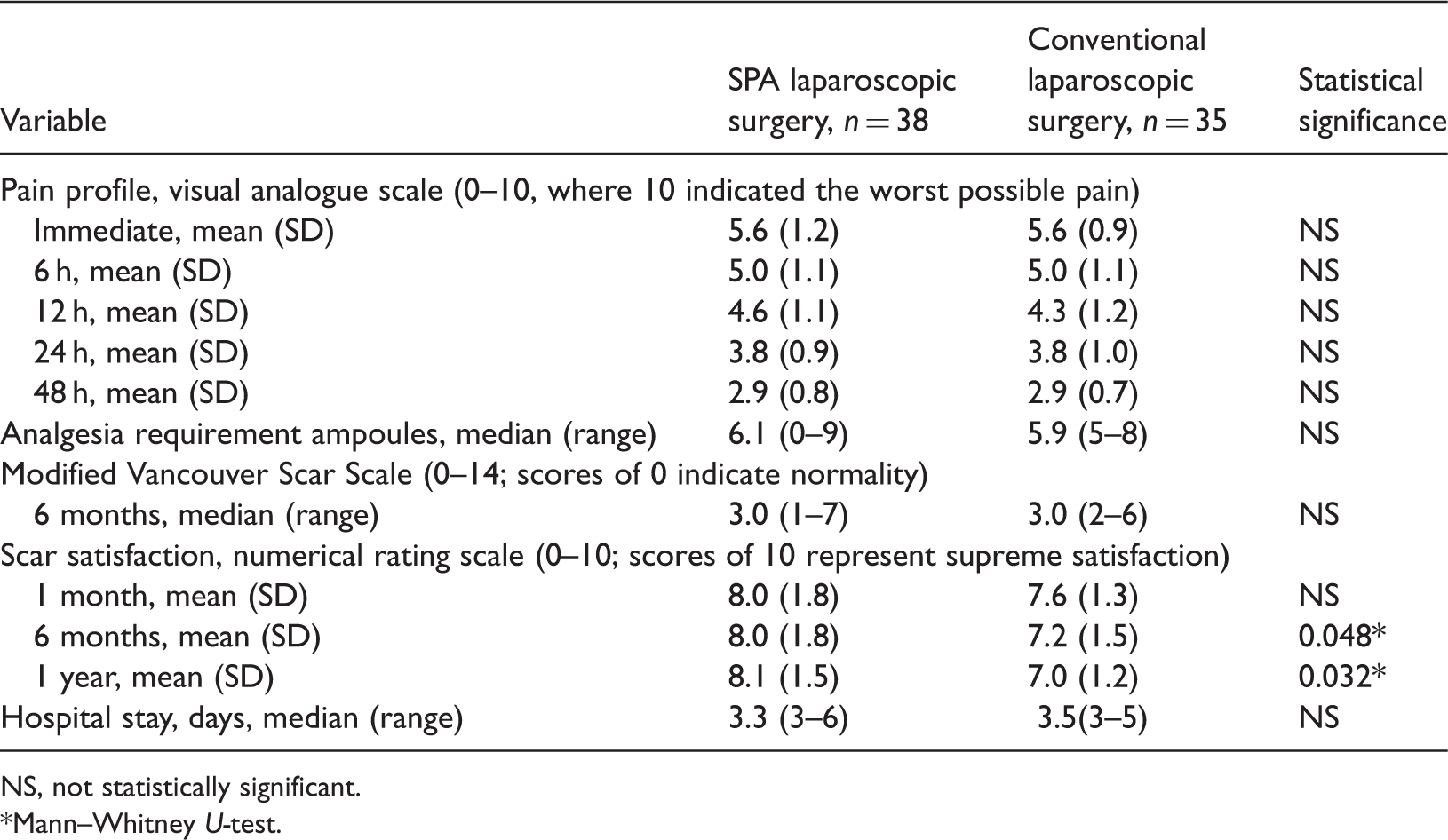
NS, not statistically significant.
Mann–Whitney U-test.
Discussion
The findings of the present study showed that SPA laparoscopic surgery was associated with better cosmetic outcomes in terms of scar satisfaction evaluated by the patient at 6 months and 1 year, though not at 1 month after surgery. There were no significant differences between the groups for operation time, complications, hospital stay, postoperative pain and analgesic requirements.
Randomized trials of SPA laparoscopic surgery have demonstrated that SPA laparoscopic surgery has perioperative outcomes comparable with those of the conventional technique.5,10–13 SPA laparoscopic surgery is not easy to learn: the surgeon (even if experienced in conventional laparoscopic surgery) must overcome obstacles such as instrument crowding and loss of triangulation. In spite of many technical challenges, however, SPA laparoscopic adnexal surgery has proven to be effective and to have a good safety profile; in addition, it is not associated with an increase in complication rates, or longer operation times.6,14–17
The original VSS was designed for burns; a modified version of it was used for this study.9,18 Like the VSS, the mVSS is regarded as being clinically useful in evaluating a wide range of scar types and has become the standard mode of scar assessment around the world.19–21 The mVSS assesses scar characteristics in terms of pigmentation, vascularity, pliability and height. However, because it does not include assessment from the patient’s perspective, or assessment of symptoms associated with the scar, the present study used an NRS to record scar-related pain and satisfaction, as assessed by the patient. SPA laparoscopic surgery is expected to provide excellent cosmetic results, with almost-invisible scars and greater satisfaction. In the present study, although better cosmetic results were evident in the SPA group than in the conventional laparoscopy group 6 months after surgery, results were similar in the two groups at 1 month. The reasons for similar scar-related satisfaction in the two groups at 1 month may be related to the very good scar-scale results and the high degree of scar-related satisfaction after conventional laparoscopy. It was difficult to demonstrate a statistically significant difference between the groups. The participants were aware that this was a treatment trial, but they accepted the randomization of the treatment groups and were not blinded to the treatment after operation. The additional two 5-mm scars on the lower abdomen in the conventional group became linear scars and lowered scar satisfaction scores were evident at 6 months after surgery. The literature on cosmetic outcome is sparse; two studies have found SPA laparoscopic surgery to have a better cosmetic outcome, compared with the conventional approach,13,22 but other studies have found no difference in cosmetic outcome, satisfaction scores and health-related quality of life between SPA laparoscopic surgery and other techniques.13, 22,23 Ma et al. 23 found that SPA laparoscopic cholecystectomy caused more complications without providing any significant benefits in patients’ overall and cosmetic satisfaction, compared with conventional four-port laparoscopic cholecystectomy. Bignell et al. 24 found that 92% of patients were satisfied with their cosmetic outcome 4 years after conventional laparoscopic cholecystectomy, and commented that single-port laparoscopic cholecystectomy seems to have a limited role in improving cosmetic results after cholecystectomy. To demonstrate more definite cosmetic benefits, a well-designed study is necessary, with a larger number of patients and a longer follow-up period, using a more suitable tool than mVSS or NRS for the evaluation of scars after laparoscopic surgery.
In general, pain after laparoscopic surgery is considered to be related to either the size or the number of ports. However, randomized trials comparing single-port and conventional laparoscopic hysterectomy have yielded conflicting results regarding postoperative pain.10,11 The findings for postoperative pain in the present study showed no difference between the two groups. There could be several reasons for our failure to find any improvement in postoperative pain after SPA laparoscopic surgery. First, with the patients being provided with adequate analgesia, pain intensity measured by the VAS was already low throughout the postoperative period. It was therefore difficult to detect any difference in pain intensity between the groups in the absence of any significant pain-provoking event. Secondly, we used a 12-mm port in the umbilicus, and used this port for specimen retrieval in conventional laparoscopic surgery. This technique did not appear to make any difference in postoperative pain compared with 20-mm transumbilical SPA laparoscopic surgery. This finding is supported by Chou et al, 25 who reported a significant decrease in immediate postoperative pain with the use of a transumbilical port, in a randomized study comparing transumbilical and transabdominal ports for laparoscopic retrieval of benign adnexal masses. Various surgical techniques in single-port surgery (such as using a soft wound retractor or commercial access ports) and conventional laparoscopic surgery (such as number of ports and location of the 12-mm port) affect postoperative pain, which could explain the conflicting results that we and others have obtained. Lastly, pain scores measured by the VAS and analgesia requirements may not fully reflect differences in pain intensity. In general, pain after laparoscopic surgery can be caused by multiple factors, such as: residual pneumoperitoneum; neuropraxia of the phrenic nerve due to pneumoperitoneum; temperature of the insufflated gas and irrigation fluid; direct tissue trauma from electrocoagulation or mechanical injury; size and number of ports; sociocultural and individual factors.26–28 The lack of a proper assessment tool for reflecting differences in these factors could explain the conflicting results that have been observed.
In the present study there was no between-group difference in the length of hospital stay. However, the duration of hospital stay is determined by cultural background, the health insurance system and patient’s expectations. Therefore, the duration of hospitalization could not be used as a measure of the speed of recovery in this study.5,10,11
The strengths of our present study include its prospective, randomized design, the use of a validated questionnaire and the long follow-up period after surgery. A limitation of our study is that it was inadequately powered to assess differences in postoperative pain and immediate cosmetic outcomes because of the small number of participants. However, our study demonstrated the favourable safety profile of SPA laparoscopic surgery, in experienced hands.
Our present study results demonstrate that SPA laparoscopic surgery for adnexal pathology had a good safety profile and was comparable with conventional laparoscopic surgery, in terms of perioperative outcomes and complication rates. However, our findings do not support a clear advantage for SPA in terms of postoperative pain and immediate cosmetic outcome. Further investigations are warranted, to establish the potential benefits of in terms of postoperative pain and cosmetic outcomes, using validated tools, in double-blind randomized trials with adequately long follow-up periods.
In conclusion, in this prospective randomized study, the clinical outcomes of SPA laparoscopic adnexal surgery were comparable with those of conventional three-port surgery, in a gynaecological setting. A better cosmetic outcome was evident in the SPA group than in the conventional surgery group, at both 6 months and 1 year after surgery.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.