
Abstract
Group A
Introduction
Respiratory tract infections, such as acute sinusitis, acute otitis media, pharyngitis, community-acquired pneumonia, and acute bronchitis, are widespread and represent a major health concern particularly in low-resource settings. In developing countries, they contribute significantly to morbidity and mortality in the pediatric setting, with an estimated lethality rate of 15% in young children. 1
Group A
Recently, the increase in the incidence of antibiotic-resistant clinical isolates of
As in developed countries, studies have been initiated in Dakar to monitor the development of resistance of
Materials and Methods
S. Pyogenes Isolates
From November 2008 to April 2009, clinical specimens from sputum, bronchoalveolar lavage, middle ear, throat swap, and sinus fluids were collected from patients with upper respiratory tract infections (sinusitis, acute otitis media, and pharyngitis) or lower respiratory tract infections (community-acquired pneumonia, acute bronchitis) in Aristide Le Dantec university hospital in Dakar, Senegal. The samples were analyzed as previously described.
6
Briefly, samples were cultured on agar trypticase-soya supplemented with 5% sheep blood and incubated in 5% CO2 for 24 to 48 hours at 37°C.
Antibiotic susceptibility testing
The antimicrobial susceptibility profile of seventeen antibiotics belonging to 9 classes, including β-lactams (penicillin G 10 µg, amoxicillin 25 µg, cefixime 5 µg, cefpodoxime 10 µg, cefotaxime 30 µg, and ceftriaxone 30 µg), macrolides (erythromycin 15 µg, spiramycin 100 µg, and azythromycin 15 µg), lincosamins (clindamycin 2 µg), streptogramins (pristinamycin 15 µg), ketolids (telithromycin 15 µg), fluoroquinolones (levofloxacin 5 µg), glycopeptides (teicoplanin 30 µg, and vancomycine 30 µg), phenicols (chloramphenicol 30 µg), and cyclines (tetracycline 30 µg), was performed using standard disk diffusion method (Oxoid Ltd, Basingstoke, Hampshire, UK), and the minimum inhibitory concentration (MIC) was determined for 10 antibiotics by E-test (AB Biodisk, Solna, Sweden), as described elsewhere.
6
Briefly, bacterial suspensions at a concentration of 10
5
CFU/mL were inoculated on sheep blood Mueller-Hinton agar plates and incubated in 5% CO2 for 24 to 48 hours at 37°C. The ATCC 29213 strain of
Analysis of results
The WHONET software (version 5.4) was used to analyze the antimicrobial susceptibility test results. Mean values and standard deviation for diameter of inhibition zones, and geometric mean MICs were calculated. The results were expressed as mean values ± SD or as geometric means.
Results
Antimicrobial susceptibility rates of S. pyogenes isolates
A total of 40 strains of
Susceptibility rates of
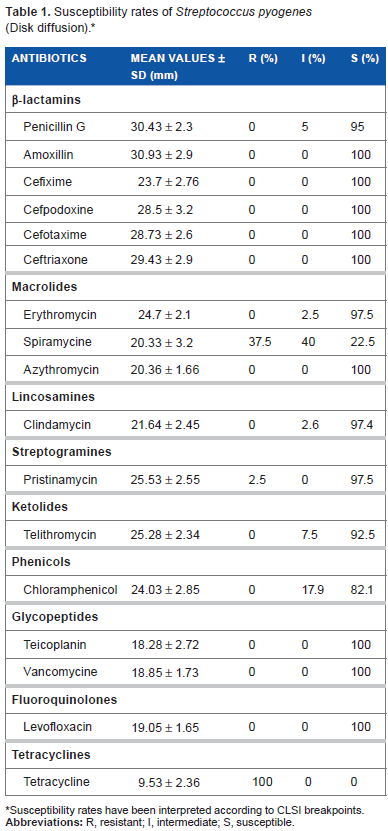
Susceptibility rates have been interpreted according to CLSI breakpoints.
Susceptibility rates of
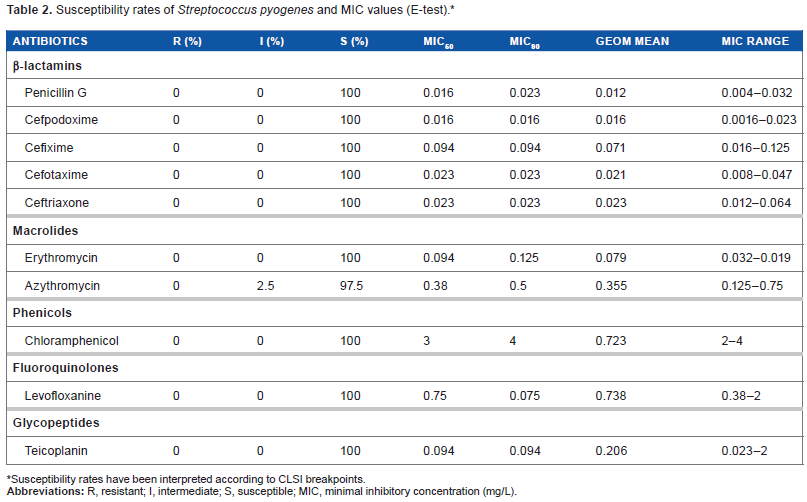
Susceptibility rates have been interpreted according to CLSI breakpoints.
Susceptibility to β-lactams
The β-lactam antibiotics showed high activity with low MIC90 ranging from 0.016 to 0.094 mg/L. Penicillin remains effective with an MIC90 value of 0.023 mg/L, although two strains showed intermediate susceptibility to this molecule. All isolates were found to be susceptible to amoxicillin, cefixime, cefpodoxime, cefotaxime, and ceftriaxone.
Susceptibility to macrolides, lincosamins, streptogramins-B, and ketolids (MLSB K)
Erythromycin showed good activity with 97.5% of isolates displaying susceptibility and only 2.5% with intermediate susceptibility. Azythromycin remains fully active as all 40 isolates are completely susceptible. Erythromycin and azythromycin had MIC90 values of 0.0125 mg/L and 0.5 mg/L, respectively. In contrast, more than half of the isolates were resistant to spiramycin with 37.5% of resistance and 40% intermediate susceptibility. Clindamycin showed high activity with 97.4% of the strains susceptible. Only 2.5% of the isolates were resistant to pristinamycin. 92.5% of the strains were susceptible to telithromycin, and 7.5% showed reduced susceptibility.
Susceptibility to chloramphenicol
Chloramphenicol was sensitive in 82.1% of isolates with the disk diffusion method, and fully sensitive with by the E-test method with MIC90 value of 4 mg/L.
Susceptibility to other antibiotics
Discussion
Susceptibility to β-lactam antibiotics
In our study, we observed that all strains were susceptible to penicillin G with only 5% of strains presenting an intermediate susceptibility, which could be the result of poor reading of inhibition diameter (27 mm). This high activity of penicillin G was confirmed by the E-test with a susceptibility of 100%. A similar result was obtained in a previous study conducted in Dakar from patients with acute tonsillopharyngitis. 6 The same high activity of penicillin G had been reported in many countries, namely Morocco, 8 France, 9 and Germany. 10 However, penicillin treatment failures have been reported in patients with tonsillopharyngitis, 11 which has suggested a possible emergence of penicillin-resistant strains, probably by β-lactamase production or copathogens interference and alteration of microbial balance. Diversification of molecules used could reduce this phenomenon. The teicoplanin (glycopeptides) and pristinamycin (streptogramins) may represent a safe alternative.
In addition to penicillin, amoxicillin and cephalosporins were fully active against
Susceptibility to MLSB K
Erythromycin and other macrolides were recommended as initial alternate choices for patients who are allergic to penicillin.
15
No erythromycin-
More than half of strains of
In this study, activity of clindamycin for group A streptococci was excellent: 97.4% of strains were susceptible, with 2.6% exhibiting intermediate susceptibility. No resistance has been observed in our study, in contrast to that of Soumah who reported, in 2002 in Dakar, 2.7% resistance (Soumah unpublished data). Our result is similar to the lack of clindamycin resistance of
Pristinamycin was very active in our study (97.5% of strains were susceptible, with only 2.5% of strains showing decreased susceptibility). This difference could be due to poor distribution of the strains on the agar and may not reflect true decreased susceptibility.
All strains were susceptible to telithromycin with more than 92% of activity, comparable to observations in Europe (98.5 of the strains tested were susceptible). 24 Such results may justify the use of this antibiotic in the treatment of pharyngitis due to group A streptococci. Indeed, a 5-day regimen of telithromycin is as effective as 10-day regimen of clarithromycin 250 mg twice daily or phenoxymethylpenicillin 500 mg 3 times daily. 25
Susceptibility to others antibiotics
In this present study, levofloxacin showed very good activity with 100% of strains susceptible to this molecule. This is in agreement with high susceptibility rates (90% to 100%) reported in North African countries,
26
in France,
27
and also in the USA.
28
By contrast, resistance to levofloxacin was observed in Poland in 2001.
29
However, based on our results, levofloxacin may represent an effective alternative choice for treatment of patients infected with
Conclusion
Group A β-haemolytic streptococci is one of the major causes of acute respiratory tract infections. Emergence of penicillin-resistant and other antibiotic-resistant clinical isolates of
Treatment of respiratory streptococcal infections is difficult and there are many factors to consider when choosing an antibiotic regimen. Susceptibility to antibiotics of any isolated strain should be evaluated as this is the only guarantee of prompt and effective treatment. The antibiotic therapy should be associated with adequate preventive methods that must include education of nursing staff in order to avoid as much as possible nosocomial infections, education of the general population for a politic of hygiene and abandonment of the common practice of self-medication, and increased scientific cooperation between clinicians and microbiologists in the interest of improving public health.
Author Contributions
Conceived and designed the experiments: MC, AD and CSBB. Analyzed the data: MC and AD. Wrote the first draft of the manuscript: MC and AD. Contributed to the writing of the manuscript: MC, AD and CSBB. Agree with manuscript results and conclusions: MC, AD and CSBB. Jointly developed the structure and arguments for the paper: MC, AD and CSBB. Made critical revisions and approved final version: MC and CSBB. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
We thank Amadou Diop for technical assistance, and Dr Amy Bei for helpful comments.