
Abstract
Aim
To assess the response of postprandial (PP) hypertriglyceridemia to genfibrozil in healthy male subjects with isolated low HDL-Cholesterol but without the metabolic syndrome (MS).
Patients and methods
14 male subjects with isolated low HDL (HDL-C ≤ 33), normal fasting triglycerides and LDL-C levels and without any feature of the MS, were studied. 13 male subjects with HDL-C > 38 mg/dl served as controls. They also had normal fasting triglycerides and LDL-C levels and without any feature of the MS. The 2 groups were statistically similar with respect to age, blood pressure, BMI, body fat composition, waist circumference, waist to hip ratio, fasting insulin, fasting and PP blood sugar, baseline fasting TG level and baseline LDL-C. Postprandial TG levels were measured at 2, 4, and 6 hours following a morning meal. Ten of the patients with PP hypertriglyceridemia were treated with gemfibrozil 600 mg PO twice/day for one month.
Results
Patients had markedly higher levels of the peak PP TG at 4 hours compared to controls (296.0 ± 37.7 vs. 206.7 ± 29.9 mg/dl; P < 0.05) the other two postprandial levels were also higher in patients but the difference was not significant. Treatment with gemfibrozil significantly decreased the levels of fasting and postprandial TG and increased HDL-C by around 3.6 mg/dl (11.7%) without affecting LDL-C.
Conclusion
Postprandial increase in serum TG may be present in patients with isolated HDL-C without the MS. Treatment of patients with PP hypertriglyceridemia with gemfibrozil improves the low HDL-C and postprandial rise in TG.
Introduction
A low concentration of plasma high-density lipoprotein cholesterol (HDL-C) is an independent risk factor for coronary heart disease (CHD).1,2 In the PROCAM study 45% of men and women who developed CHD had an HDL-C level less than 35 mg/dl 3 and the Framingham Heart Study established that a change in cholesterol/HDL ratio is a better predictor for reducing CHD incidence than changes in total cholesterol level. 4 A meta analysis of four large prospective studies has shown that an increase in HDL-C of 0.026 mmol/l reduces coronary events by 2%–3%. 5
Raising HDL-C may be as important as lowering low-density lipoprotein cholesterol (LDL-C) to prevent CHD. 6 Important clinical trials have been designed to investigate the effects of pharmacologic agents on HDL-C raising and CHD risk in large populations independent of the effect of LDL-C lowering. Two of these trials specifically investigated the effect of gemfibrozil: the Helsinki Heart Study 7 and the Veterans Affairs High-Density Lipoprotein Trial (VA-HIT). 8
Multivariate analysis studies have shown that postprandial triglyceride (TG) levels were an independent predictor of CHD.9,10 Many studies have correlated low fasting HDL and/or the metabolic syndrome with postprandial hypertriglyceridemia;11–14 however, only few studies had investigated the link between low fasting HDL-C and postprandial hypertriglyceridemia in healthy subjects with normal fasting TG and cholesterol levels.15–17 In this study we intend to evaluate the correlation between primary low HDL-C and postprandial hypertriglyceridemia in healthy subjects.
Patients and Methods
14 Male subjects with isolated low HDL (HDL-C ≤ 33) were studied. 13 Male subjects with HDL-C > 38 mg/dl served as controls. Both groups had fasting triglycerides less than 150 mg/dl and LDL-C levels less than 130 mg/dl and they had no feature of metabolic syndrome (MS). Subjects and controls were excluded if they had diabetes, history of excessive alcohol intake, hypertension, metabolic syndrome, coronary artery disease, gout, drug intake, renal or liver disease and other associated lipid abnormalities. MS was excluded based on ATP III definition. The 2 groups were statistically similar with respect to age, blood pressure, BMI, percentage body fat composition, waist circumference, waist to hip ratio, fasting insulin, fasting leptin, fasting and PP blood sugar, baseline fasting TG level and baseline LDL-C (Table 1). Total body fat content was determined by impedance technique. LDL-C was estimated using the Friedwald equation. Postprandial TG levels were measured at two, four, and six hours following a morning meal that consisted of one third of the total daily caloric intake of the individual patients distributed as 30% fat, 55% carbohydrate and 15% protein. The breakfast meal was preceded by a 12-hour fast and all subjects were sedentary in the days prior to the study meals. Ten out of the fourteen patients had 4 hours postprandial hypertriglyceridemia higher than 300 mg/dl. These patients were treated with gemfibrozil 600 mg PO twice per day for one month following which fasting and postprandial lipid profiles were determined.
Patients' characteristics.

Statistical methods
Means of the different variables in the two groups were compared using ANOVA test. Comparison between the means of the treated groups before and after treatment was done using ANOVA and a P value of <0.05 was considered significant.
Results
There was no significant difference at baseline between the two groups except for the HDL levels (Table 1). The peak TG level was found to occur at 4 hours postprandially (Fig. 1). Although the baseline fasting TG levels in the two groups were similar (120.0 ± 11.9 and 125.1 ± 12.8 mg/dl in patients and controls respectively), patients had markedly higher levels of peak postprandial TG than controls (296.0 ± 37.7 versus 206.7 ± 29.9 mg/dl; P value <0.05). The postprandial TG levels at two and six hours postprandially were also higher in patients than controls although the difference did not reach statistical significance: 247.4 ± 30.5 versus 207.5 ± 19.0 mg/dl at 2 hours postprandial, and 268.3 ± 46.8 mg/dl versus 178.9 ± 26.7 mg/dl at 6 hours postprandial (Fig. 1).
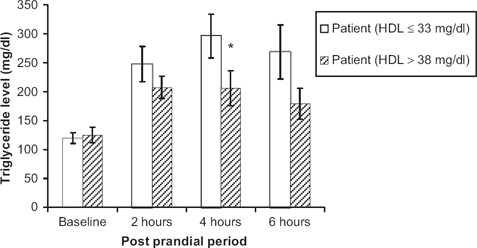
Comparison of triglyceride levels fasting and at three intervals postprandial between subjects with an HDL ≤ 33 vs. subjects with an HDL > 38 mg/dl.
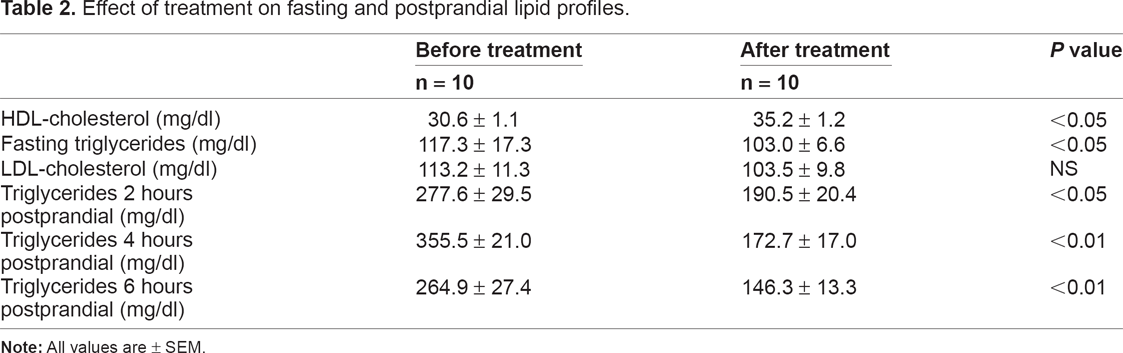
Treatment with gemfibrozil significantly decreased the levels of TG both fasting (from 117.3 ± 17.3 to 103.0 ± 6.6 mg/dl) and postprandial (from 277.6 ± 29.5 to 190.5 ± 20.4, 355.5 ± 21.0 to 172.7 ± 17.0, and 264.9 ± 27.4 to 146.3 ± 13.3 mg/dl at 2, 4 and 6 hours after meal respectively). Treatment also increased HDL-C by 3.6 mg/dl (11.7%) but it did not affect LDL-C (113.2 ± 11.3 before treatment vs. 103.5 ± 9.8 mg/dl after treatment) (Table 2). The treatment with gemfibrozil was well tolerated and no side effects were reported.
Effect of treatment on fasting and postprandial lipid profiles.
Discussion and conclusion
BMI, body fat, waist circumference, WHR, leptin and insulin levels were not statistically higher in the group with low HDL compared to the group with higher HDL. This is in contrast to another study by Couilllard et al which stated that low HDL concentrations is not associated with postprandial hyperlipidemia unless accompanied by other features of the insulin resistance syndrome. 16
The means of the postprandial TG levels were consistently high at different intervals post meal in the group with lower HDL despite the normal fasting TG. This finding is consistent with two other studies. The first study by Patsch et al showed that normolipidemic subjects with low HDL2 subfraction are less able to clear alimentary fat and therefore have higher levels of postprandial TG than those with high HDL2 fractions. 15 A second study conducted recently by Kolovou et al clearly showed that the delayed clearance of TG postprandially seems to result in low HDL cholesterol levels even in subjects with low fasting TG concentration. 17
The peak TG level occurred at 4 hours postprandial, which is consistent with other studies showing that in healthy subjects a significant serum triglyceride peak occurred 4–5 hours postprandially after ingestion of a standardized lipid load.18–20 However, in this study, we elected to measure TG levels after a usual morning meal that was constituted of one third of the total daily caloric intake in an attempt to assess the actual postprandial TG after a regular daily meal. This may explain the fact that the levels of postprandial TG in our study were not as high as reported after a lipid load.
The effect of gemfibrozil on HDL raising was established by the Helsinki study which showed that treatment with gemfibrozil lowered the mortality rate due to myocardial infarction while at the same time exerting the most marked influence on the concentration of HDL-C.7,21,22 Another similar trial is the Veterans Affairs High-Density Lipoprotein Trial (VA-HIT) that showed that therapy with gemfibrozil significantly reduced the incidence of CHD events in patients with known coronary artery disease and a low level of HDL-C by increasing HDL without decreasing LDL and TG.8,23,24
Moreover, other studies have established the role of fibrates in lowering postprandial triglyceridemia.25–28 However no previous studies linked the effect of gemfibrozil on fasting HDL to its effect on postprandial hypertriglyceridemia in a setting where the subjects are healthy and the only fasting lipid abnormality is a low HDL. The reason why PP triglyceridemia should have an effect on HDL-C would be namely due to the recognized role of cholesteryl ester transfer protein (CETP) in HDL metabolism where CETP transfers cholesteryl esters from HDL to the apo B–containing lipoproteins, very low density lipoprotein (VLDL) and LDL. We found, as expected that gemfibozil decreased fasting TG as well as postprandial TG and increased HDL-C without affecting LDL-C. Since the baseline fasting TG levels were within the normal range and there were no significant differences between the two groups in these levels, this implies that the effect of gemfibrozil on HDL-C might be principally mediated by its effect on postprandial TG. The number of subjects enrolled is one of the limitations of this study therefore other similar studies with a larger number of patients should be conducted to establish the association between postprandial TG and HDL-C.
In this study we excluded metabolic syndrome and conditions that may lower HDL-C. We compared BMI and body fat, WHR, insulin levels, glycemia both fasting and postprandial, blood pressure, and fasting triglycerides between the two groups. Because the differences in all of these were not statistically significant we can conclude that postprandial hypertriglyceridemia in the group with lower HDL was present independent of these factors. Finally, its’ speculated that in male subjects, the postprandial increase in serum TG may play a role in the suppression of HDL-C and that treatment with gemfibrozil may improve the low HDL-C by improving mainly the postprandial rise in TG.
Footnotes
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.