
Abstract
Objective
To evaluate the relationship between cholesterol and triglycerides and bone mineral density in patients with vascular disease (hypertension and acute coronary syndrome).
Methods
The study included 217 patients (83 men and 134 women), aged between 36 and 76 (mean age 59 ± 10), with hypertension and acute coronary syndrome. Information obtained included anthropometric measurements, total cholesterol, HDL cholesterol, LDL cholesterol and triglycerides; bone mineral density (BMD) was recorded at the lumbar spine.
Results
BMD was significantly lower in patients in the higher tertiles of cholesterol (p = 0.041). The effect was maintained after adjustment for age and Body Mass Index (BMI). However, there was no association between the range of triglycerides, LDL cholesterol, HDL cholesterol and bone mass.
Conclusions
A relationship was found between total cholesterol and bone mineral density in patients with vascular disease.
Introduction
Atherosclerosis and osteoporosis are chronic degenerative diseases with a high incidence in developed countries, whose prevalence will increase as the population ages(1,2). They are silent processes with a high economic cost that becomes evident when the acute complications, including vascular accidents and osteoporotic fractures become overt. Various epidemiological studies have shown an age-independent association between the two diseases(3,4).
Atherosclerosis, which plays a role in heart disease, cerebrovascular accidents and peripheral arterial disease, is responsible for most cardiovascular disease. It is characterized by chronic arterial inflammation caused and exacerbated by disorders of the lipid metabolism and other clearly-identified risk factors (5). Calcification, induced by an active process in which inflammatory cytokines and other mediators that regulate the phospho-calcium metabolism, is characteristic of atherosclerosis(6). In contrast, the same mechanisms can intervene at the level of the bone, reducing bone mineral content and altering the bone microarchitecture, leading to osteoporosis. Therefore, the two diseases, although with a different expression, share common mechanisms.
There are various well-known risk factors for cardiovascular diseases, some of which can also influence bone metabolism, modifying bone mass and facilitating osteoporosis. Lipids can play an important role in both processes. Few studies have evaluated plasma lipids (a surrogate marker of atherosclerosis) with bone mineral density (BMD) and/or osteoporotic fractures and the results are not concordant.
The objective of this study was to evaluate the relationship between cholesterol and triglycerides in patients with vascular disease (hypertension and acute coronary syndrome).
Matherial and Methods
Subjects and study protocol
The study included 217 patients (83 men and 134 women), aged between 36 and 76 (mean age 59 ± 10), with systolic and/or diastolic stage I-II hypertension, according to JNC VII criteria or acute coronary syndrome according to European Society of Cardiology guidelines. The exclusion criteria were: alcoholism, neoplasia, secondary arterial hypertension, chronic renal failure, hyper- and hypocalcemia, diabetes, hyperparathyroidism and use of drugs modifying BMD (calcium, vitamin D, estrogens, calcitonin, bisphosphonates, and fluorine).
Measurements
Blood samples were obtained after 8 fasting hours in the morning. Total serum cholesterol and triglyceride concentrations were determined by enzymatic colorimetric assay (Roche Diagnostics GmbH, Mannheim, Germany), while HDL cholesterol was determined enzymatically in the supernatant after precipitation of other lipoproteins with dextran sulfate-magnesium. LDL-cholesterol was calculated using the Friedewald formula.
Densitometry studies were conducted in the lumbar spine (L2–L4) using an X-ray densitometer (DEXA, Lunar Corporation, Madison, Wisconsin, U.S.A.). The BMD results were expressed in g/cm2 and as peak percentage of bone mass in normal subjects (T-score) and percentage of subjects of the same age and sex (Z-score), depending on the software used in the device.
Statistical analyses
A descriptive statistical analysis, including central and dispersion trends, was conducted for quantitative categories, and absolute and relative variables were analyzed for the different categories. The Student's t-test was used to analyze the data that matched the aim of the study and the Anova method was used to compare multiple groups. The relationship between variables was assessed using Pearson's correlation coefficient. Multiple regression analysis was used to assess the relationship between BMD and plasma lipid levels. The results are expressed as mean ± standard deviation.
Ethical issues
This study was approved by the hospital's ethics committee and the patients signed an informed consent form.
Results
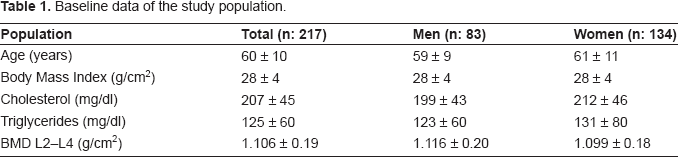
Baseline data of the study population.
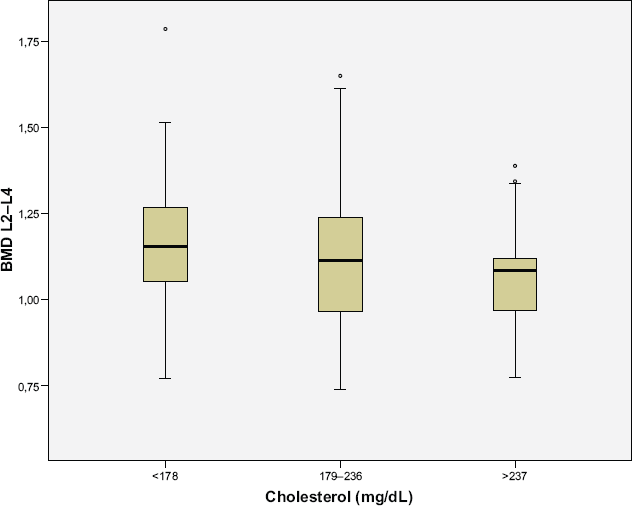
Cholesterol levels (tertiles) and BMD.
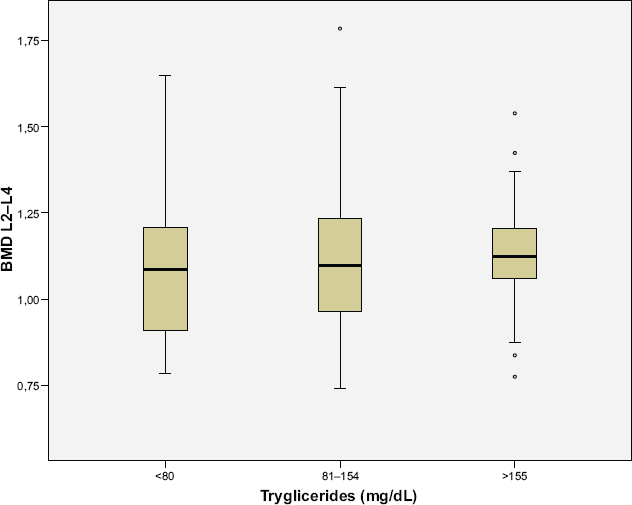
Triglyceride levels (tertiles) and BMD.
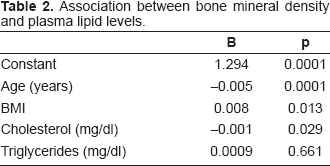
Association between bone mineral density and plasma lipid levels.
Discussion
We found evidence for a weak association between total cholesterol and spine BMD in patients with vascular disease. Patients with higher levels of total cholesterol had lower BMD. Few clinical studies have investigated the link between plasma lipids and BMD. Broulik et al.(7) reported that osteoporotic women had higher cholesterol levels than female controls. Yamaguchi et al.(8) found that LDL cholesterol was inversely and significantly related to BMD while the reverse occurred with HDL cholesterol. Furthermore, patients with a low bone mass had higher plasma lipid levels associated with more severe vascular disease(9). Other studies found differing results. The Framingham Osteoporosis Study found no association between cholesterol levels and subsequent osteoporosis(10). Similarly, Tanko et al.(11), in a study of 340 postmenopausal women aged <76 years, found no relationship between cholesterol and mean BMD 8 years later. Our group found no relationship between plasma lipids and bone mass in type 2 diabetic patients(12).
Recently, Solomon et al.(13) have analyzed 13592 participants in the National Health and Nutritional Examination Survey (NHAMES) III in whom BMD and lipid levels were recorded. In the crude analysis, higher total cholesterol and LDL levels were associated with lower BMD whereas higher HDL-levels were associated with lower BMD. However, in fully adjusted models, there was no significant relationship. Dennison et al.(14), in a British study, demonstrated a relationship between lipid profile and BMD that was greatly attenuated by adjustment for total body fat. Our results are similar. There was a relationship between total cholesterol and BMD but the relationship remained significant in the adjusted model, although weak (Table 2).
The results of other studies are not concordant, probably due to the heterogenous nature of the study populations, which vary from healthy cohorts to patient series. Key factors are body fat and BMI, which attenuates the relationship and makes the comparison of results difficult.
Both direct and indirect reasons may explain the possible association between bone mass and the lipid profile. During the menopause there is an abrupt fall in estrogens accompanied by greater bone mass loss and an increase in cholesterol and triglycerides. In addition, various drugs (estrogens, statins, estrogen receptor modulators, and bisphosphonates) can act on both parameters. On the other hand, osteoblasts and adipocytes share common progenitor cells in the bone marrow. Some authors, such as Parhami et al.(15), suggest a possible lipid etiology for osteoporosis. The coexistence of vascular calcification and osteoporosis is not infrequent, and a significant role is attributed to oxidized low-density lipoproteins. This author suggests that these proteins would act in pluripotential stem cells of the bone marrow, enhancing their progression to adipocytes instead of osteoblasts. Furthermore, oxidized lipids induce the expression of chemotactic factors for monocytes and M-CSF in the endothelium, a significant catalyst of osteoclastic differentiation(16).
Our study had several limitations. The study population was small and there were two groups of participants, patients with hypertension and those with coronary syndrome, who could have different regulation of BMD and lipidic metabolism.
In conclusion, we found a relationship between total cholesterol and BMD in patients with vascular disease. Cholesterol and BMD are only two of the variables associated with atherosclerosis and osteoporosis and other parameters can play a key role in the association between the two diseases(17).